
Abstract
Abstract
Background and Aim:
We report the process of creating a new palliative care service at a large, urban children's hospital. Our aim was to provide a detailed guide to developing an inpatient consultation service, along with reporting on the challenges, lessons, and evaluation.
Methods:
We examined the hiring process of personnel and marketing strategies, a clinical database facilitated ongoing quality review and identified trends, and a survey project assessed provider satisfaction and how referring physicians used the palliative care service.
Results and Conclusion:
The pilot phase of service delivery laid the groundwork for a more effective service by creating documentation templates and identifying relevant data to track growth and outcomes. It also allowed time to establish a clear delineation of team members and distinction of roles. The survey of referring physicians proved a useful evaluation starting point, but conclusions could not be generalized because of the low response rate. It may be necessary to reconsider the survey technique and to expand the sample to include patients and families. Future research is needed to measure the financial benefits of a well-staffed inpatient pediatric palliative care service.
Introduction
Cultural and institutional barriers to integration of palliative care have been well-described, including defining the scope of palliative care as concurrent with curative treatment, differentiating from hospice, increasing awareness among primary physicians of the benefits of palliative care, distinguishing the roles of the primary team and palliative care team, and hiring qualified personnel with experience in managing terminally ill patients. 3 The close partnerships between primary physicians and families, as well as the uncertain prognoses of life-threatening illnesses in pediatrics, amplify these barriers in pediatric palliative care.
We report the process of creating a new palliative care service at a large urban children's hospital, the steps taken to overcome barriers, and an initial evaluation of the effectiveness of the service in meeting the needs of consulting physicians. A scant number of publications have addressed the phases of program development involved in establishing a pediatric palliative care program.4–6 These papers provide guidelines and solutions to common challenges. Based on the variance of institutions and resources, however, many elements may not apply to a majority of new programs. We aim to provide a detailed guide to developing an inpatient consultation service, along with reporting on the challenges, lessons, and evaluation.
Methods
We reviewed the organizational development and evolution of clinical practice within the palliative care service at a large, urban children's hospital from its inception in September 2008 through September 2011. We examined the hiring process of personnel and marketing strategies used to promote palliative care within the hospital and community. From the outset, a clinical database facilitated ongoing quality review. We extracted information from the database to identify trends in the number of patients followed by the palliative care service since it began to serve patients in January 2009 until September 2011, and to determine the proportion of patients who had died in the hospital and had been followed by the palliative care service.
Two years after initiating the service, a survey project assessed provider satisfaction and how referring physicians used the palliative care service. All attending physicians (n=229) were invited to complete the survey online. An informational consent form was included in the introduction to the survey; physicians indicated their consent by proceeding to the survey questions. Items focused on physicians' awareness of the palliative care service, reasons physicians consulted the service, and barriers to consultation. The Institutional Review Board approved the study.
Results
Initial funding
Two primary factors preceded the decision of the hospital's Board of Trustees to financially support the program for an initial 3-year period: 1) the increasing national recognition of the importance of a physician-led, integrated palliative care service; and 2) the awareness by the hospital's medical and nursing staff of the need to centralize palliative care services to be systematically available hospital-wide.
Recruitment and role definition
The medical director of the Comfort, Pain, and Palliative Care Program identified key roles for the palliative care service: physician, nurse practitioner, social worker, and clinical psychologist. A psychologist (0.5 FTE) and social worker (1.0 FTE) were hired expediently, but the service had been launched for several months before a nurse practitioner was hired (1.0 FTE). The medical director provided limited physician coverage due to competing responsibilities overseeing acute and chronic pain programs. A board-certified palliative care physician was hired 10 months after service began, but that physician relocated within a year. Another physician was hired at the end of the study period, and a second physician was recently hired to meet the growing demands of the service. The physician oversees symptom management, coordinates care among different inpatient services involved in patients' care as well as with hospice agencies after hospital discharge, and counsels families on medical decision making. The physician also provides all overnight and weekend care for urgent inpatient medical needs.
The nurse practitioner provides immediate consultation to primary teams and daily symptom management needs. The nurse practitioner coordinates care for patients and families both within the hospital and with outpatient providers (hospice, home health agencies, etc.). Our program has the unique advantage of collaborating with one of the few pediatric hospices in the country. Our team is also developing relationships with adult hospices interested in expanding into pediatrics, which requires substantially more involvement. The nurse practitioner maintains regular communication with hospices and families to ensure a smooth transition and to proactively address problems that could interfere with continuing hospice. This includes weekly updates via e-mail and/or phone with several hospices, and ongoing communication with families regarding their satisfaction.
Differentiating the psychosocial roles on the team required experimentation due to the lack of a model for a team including a social worker and psychologist. In the present model, the social worker focuses on the parents' emotional and resource needs. The psychologist addresses the patient's mental health needs, including emotional symptoms (e.g., anxiety, depression), to maximize decision-making abilities, facilitate communication, and enhance the patient's ability to participate in treatment.
The social worker faced the challenge of distinguishing herself from the primary social worker assigned to each family. She developed a bereavement protocol and provides all bereavement services to families for 18 months; because there is no other bereavement program in the hospital, this is an added value to standard of care. The social worker also developed staff support groups for various disciplines across the hospital to address coping with grief, trauma, and burnout.
Needs assessment
The first phase of development consisted of a needs assessment conducted over a 4-month period. Interviews with key stakeholders within the hospital elicited information about existing resources, unmet patient needs, and the cultural attitude toward integrating a palliative care service.
A Palliative Care Advisory Board (PCAB) functioned for several years prior to the hospital funding a palliative care service. This group included physicians, nurses, social workers, and chaplains who championed palliative care principles throughout the hospital. Members of the PCAB were interviewed separately to describe current standards and practices.
The PCAB identified several palliative care needs, including improved symptom management, assisting families and staff with decision making about advanced care, and improving end-of-life care processes. The management of complex patients was frequently described as fragmented, with poor communication among multiple services, resulting in inadequate coordination of care. Specifically, the transitions between hospital to home (with or without hospice) had been especially problematic.
Based on feedback from interviews with division heads, a consulting service model was developed to provide palliative care while respecting the primary role of patients' physicians. In this model, health care professionals from any discipline could recommend a palliative care consultation; however, the patient's primary physician must express verbal or written agreement prior to the palliative care team meeting the family.
Three key areas of focus emerged from this needs assessment for the implementation of the palliative care service: clinical care, education, and visibility.
Clinical care
Service delivery began with a brief “pilot” phase, during which consultations were invited from oncology and pulmonology. These divisions were well-represented on the PCAB and self-identified as having immediate need. Consultation and follow-up forms designed for the palliative care service were added to the electronic medical record system, allowing for prompt identification of palliative care notes within each patient medical record (Appendixes 1 and 2). These forms were created based on models from other palliative care programs and accepted standards for palliative care assessments; they received internal approval before use. Ten patients were referred within the first 6 weeks. These initial consultations were well-received by patients, families, and staff so the service expanded to the whole hospital.
Clinical care included symptom management (pharmacologic and nonpharmacologic); psychosocial support for patients, parents, and siblings; assisting the family in medical decision making; and providing complex care coordination, including transition to home with or without hospice. Whereas patients had historically been referred to a single hospice agency, the palliative care service identified additional providers to increase the coverage within Los Angeles County and beyond. The service has strived to market its scope as broader than death and dying while also being regarded as experts in end-of-life care. Physicians explicitly stated they would “never” refer their families to palliative care because it signified “giving up.” This led to naming the service the Comfort and Palliative Care Team, allowing physicians to refer to the “Comfort Team.”
New interventional procedures, including peripheral nerve blocks, epidural and spinal catheters, and implantable devices were introduced to help manage pain, improve quality of life, and minimize opioid use. The medical director is an anesthesiologist with expertise in these procedures. Because he oversees the pain and palliative care programs, synergies have been created between the two services with respect to patients' symptom management. At times, each service refers patients to the other service as a more appropriate consult. The palliative care service established relationships with home health care agencies, delivery services, and outpatient pharmacies to provide safe management of devices in the home. Home agencies assess these devices on a daily basis, but the patients come into the palliative care outpatient clinic at least biweekly for exam. The palliative care medical team members are available at all times to manage changes and help the home agencies troubleshoot problems.
In total, the team consulted in the care of 117 patients in the first year of service, 236 during the second year, and 117 during the first 8 months of the third year. The reduction in patients seen in the fourth quarter 2010 and first quarter 2011 corresponds to the departure of the board-certified palliative care physician. The most recent increase in patients corresponds to the hiring of a new physician (Fig. 1). It is possible this fluctuation was due to the medical director's limited availability compared with physicians devoted exclusively to palliative care.

Number of patients referred to the palliative care service.
The nurse practitioner and physician see patients with acute symptom management or medical decision-making needs daily. The psychologist and/or social worker see patients with primarily psychosocial needs two to three times a week; the physician and nurse practitioner see these patients once or twice a week. During weeks with greater demands, the nurse practitioner and physician divide patients. The average daily census ranges from 11 to 23. The physician is the only team member who bills for services.
Members of the palliative care service created several new policies and procedures, including policies describing the scope of services encompassed by palliative care and the procedure for consultation, and a policy for the management of dyspnea at end of life. Policies regarding the authorization of continuous infusion of medications (i.e., midazolam, pentobarbital) only in intensive care units for end-of-life care were revised to allow this intervention on regular patient care units. These policies underwent review by multiple committees that provided feedback before approval.
Education
The palliative care service assumed responsibility for the PCAB's monthly palliative care lecture series. Providers across disciplines attend these lectures. Topics have ranged from the nature of suffering, to ethical dilemmas in end-of-life care. The team also regularly participates in other educational opportunities within the hospital, including lectures for various nursing units, grand rounds, and orientation for new employees. The social worker and psychologist conduct monthly wellness groups for pediatric residents to offer support for coping with grief and trauma.
Visibility
To increase visibility and encourage referrals, the medical director met with the directors of medical and surgical departments to discuss the scope of palliative care. The psychosocial team members also met with key hospital leaders who could help champion palliative care around the hospital (e.g., directors of spiritual care, child life, and social work). During the initial 6 months, team members attended weekly medical rounds for various oncology groups (e.g., leukemia and lymphoma, neural tumors) and participated in clinical rounds for the pediatric and cardiac intensive care units.
A handout for medical staff was created with bullet points articulating the palliative care service's philosophy of care, specific interventions, and examples of consultation triggers. Team members distributed these handouts at staff meetings and educational presentations throughout the hospital.
To educate families, the team offers brochures during initial consultations to describe how this “additional” team fits within the overall care plan. A page dedicated to the palliative care service was added to the hospital website to address the scope of palliative care and common myths and misconceptions.
Program evaluation
Within the first 2 years, an online survey was sent to every practicing physician to review whether the service had successfully achieved some of its initial goals. A total of 77 of the 229 physicians who received the survey (34%) responded. Two phases of recruitment produced this final number: 1) requesting via e-mail that division heads send the survey request to respective attendings; and 2) directly e-mailing each physician. Seventy percent of the physicians answering the survey had consulted palliative care. Of these consults, 21% originated from the three critical care units, followed by the hospitalist (19%), and hematology/oncology services (15%). Respondents identified end-of-life medical and psychosocial support to patients and families as the main reasons they consulted palliative care (75% and 71%, respectively; Fig. 2). Of physicians who had not consulted palliative care, respondents identified the primary reason as perceiving that families were “not ready” for palliative care (Fig. 3).

Reasons physicians consulted the palliative care service.
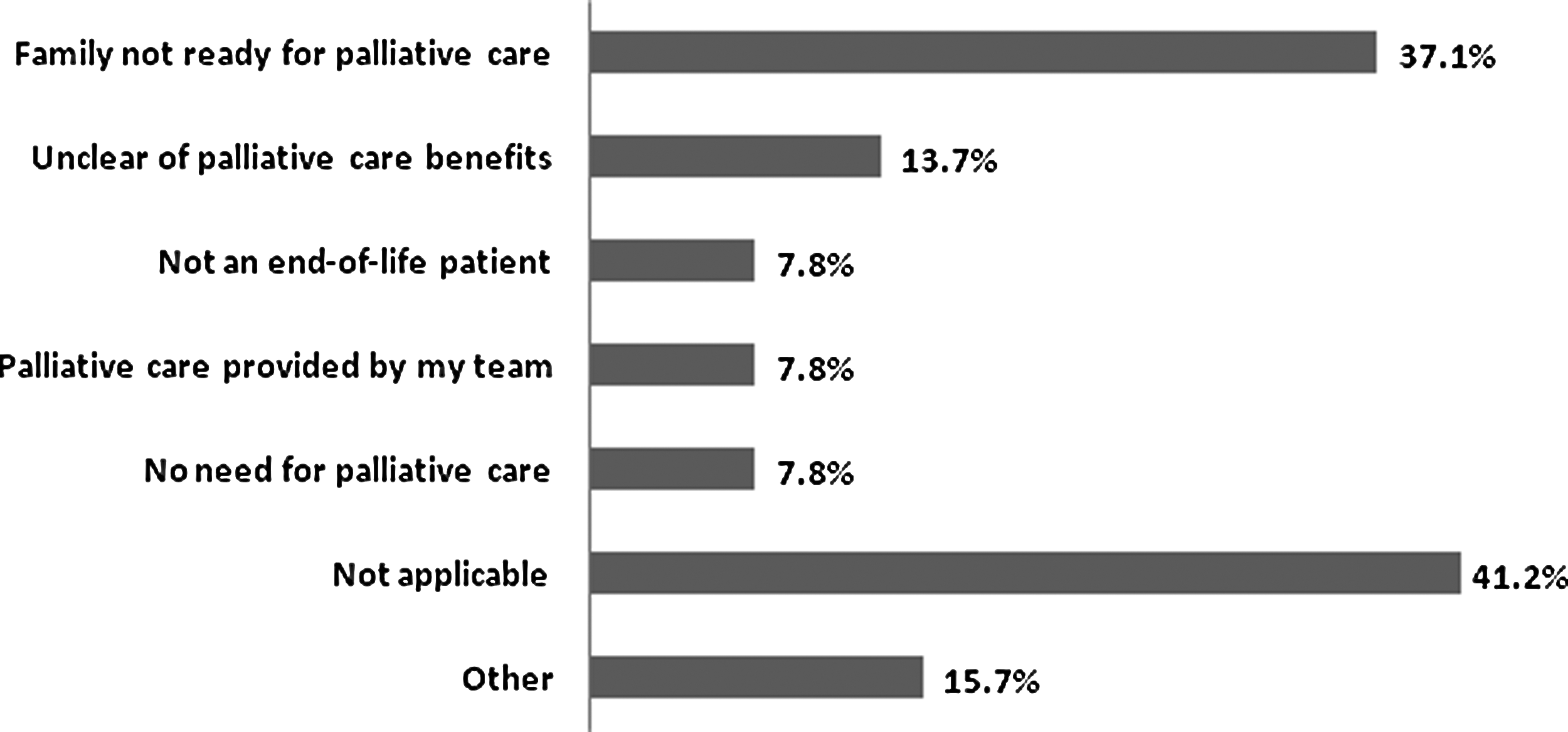
Reasons physicians decided against palliative care consult.
Of patients who died in the hospital each year, the percentage who received care from the palliative care service remained stable during the initial years of service, but significantly increased during the last year of analysis (Fig. 4).
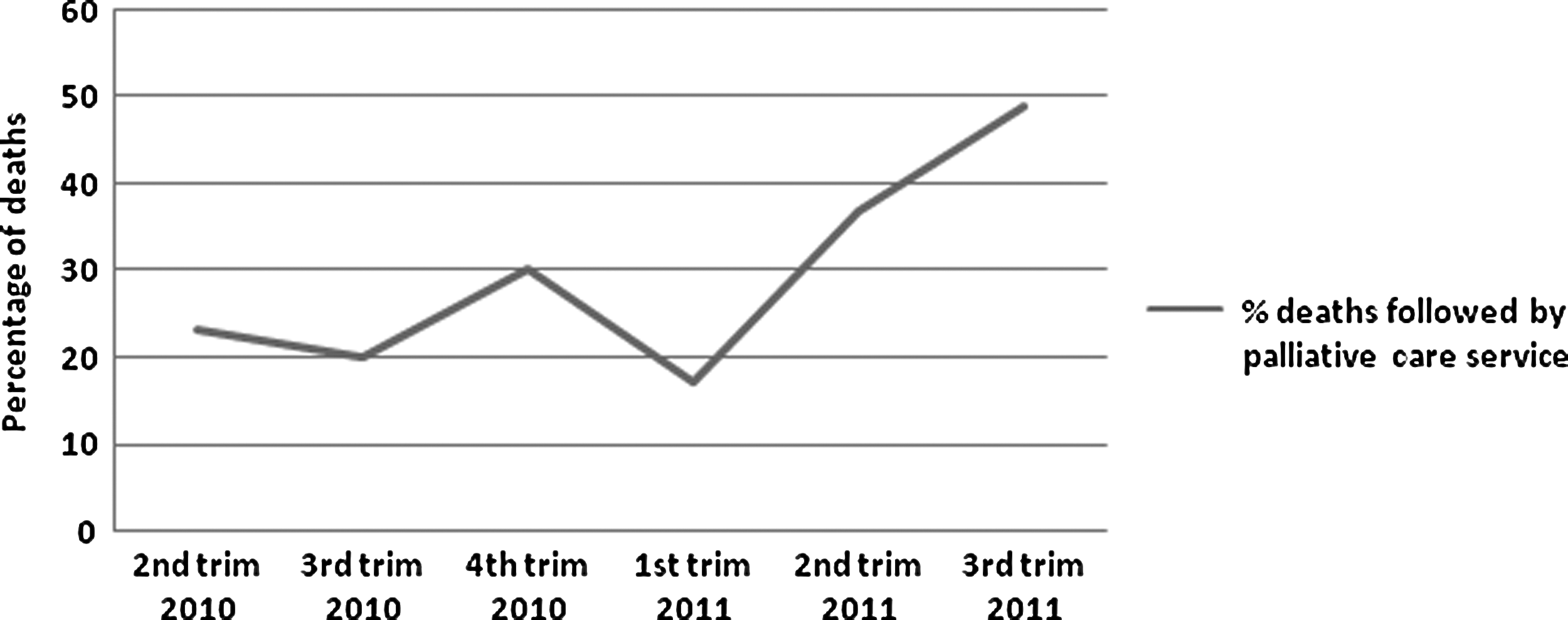
Percentage of patients who died in the hospital and had been referred to the palliative care service.
Discussion
Statistics suggest that palliative care has become increasingly recognized as essential over a short period of time. For example, a 2008 survey of hospitals with 50 or more beds indicated an increase in palliative care programs of 126% since 2000. 7 These data, however, do not specify which hospitals serve pediatric patients. Advancement in clinical care has significantly improved the life expectancy of the 25,000 children per year in the United States who are born or diagnosed with a life-threatening disease 8 ; however, significant improvements in quality of life have not matched these gains in longevity. 9
We described here the process of creating a palliative care service in a large, urban children's hospital, including successes and barriers.
Lessons learned
Establishing a pilot phase of service delivery laid the groundwork for a more effective service by creating appropriate documentation templates and identifying relevant data to track growth and outcomes. 10 This phase also allowed time to establish a clear delineation of team members and distinction of roles, a process identified as crucial for successful palliative care programs. 11
Initially, primary social workers communicated they did not see a role for another social worker. Over time, however, the palliative care social worker established herself as an expert in anticipatory grief counseling, and a valuable bereavement resource. She tailors collaboration with each social worker based on family needs and the relationship between the family and primary social worker. Our social worker also created ongoing staff support groups as a way to distinguish her role as a social worker in palliative care.
The fluctuation in referrals that correlated with the presence or absence of a dedicated palliative care physician emphasizes the importance of physician availability and visibility. An ongoing barrier, however, is that primary teams have expressed wanting 24-hour coverage by the entire team.
Addressing barriers
To promote “successful families and good outcomes for children,” the focus of care in pediatrics includes the entire family. This approach results in strong partnerships between pediatricians and families. 12 This context presents a major barrier for newly created palliative care services to introduce additional caregivers and care components.
Perhaps the most challenging part of establishing and growing the service is articulating specific ways palliative care benefits patients in addition to their primary teams. Over time, what other teams want and what we can offer crystallized and referrals became more consistent. Survey and anecdotal data suggest primary teams consult palliative care for: 1) innovative pain management techniques; 2) continuity of care from hospital to home (with or without hospice); 3) a psychologist; 4) end-of-life expertise; and 5) bereavement. If a hospital has separate pain and palliative care services, it is imperative these teams collaborate and differentiate their purposes. Although bereavement support is a primary reason for referrals, growth of our palliative care service has threatened the sustainability of bereavement follow-up as the number of families balloons each year.
To address the common misconceptions about palliative care and scope of practice, dialogue should include division chiefs and palliative care champions across disciplines to discuss views of palliative care and what the new service could offer. An initial honest discussion among providers must clearly define the boundaries between services in addition to identifying patients' needs and the potential benefits of a new service. Defining our team as strictly a consulting service has increased the comfort level of referring physicians, reflected in repeated referrals from individual physicians.
Difficulty recruiting qualified pediatric palliative care physicians faces all programs. In the United States, there are currently 88 accredited hospice and palliative care fellowship programs with 171 trainees. Only five of these programs specifically focus on pediatric palliative care. 13 Our program required specialization and board certification in related fields, which allowed for a wider applicant pool to fill the two physician positions. This program, like many others in the United States, is possible only because of significant financial support from hospital administration.
State-specific insurance and billing regulations make it impossible for a palliative care service built around our staffing model to be self-supporting (i.e., only physicians can bill and actual reimbursement covers approximately 5% of the costs). The administration recently funded the program for an additional 3 years. This decision was based on metrics showing utilization and satisfaction rather than cost-savings (e.g., number of referrals, care providers' satisfaction surveys).
These financial constraints substantially limit further development of this program. Future research must identify techniques to measure the financial benefits of a well-staffed inpatient pediatric palliative care service to justify cost for insurance companies and government programs.
Evaluation
Program evaluation is critical to the development of new palliative care programs. 14 In the program we report on here, a survey of referring physicians proved a useful starting point in evaluating the achievement of clinical and educational goals. Conclusions from this survey cannot be generalized, however, because of the low response rate. This has led the team to reconsider the survey technique for future surveys to improve the response rate and expand the sample to include patients and families. Results from family surveys would potentially address the primary barrier identified by physicians: “The family is not ready for palliative care.” The methodology required to implement a family survey project, however, would require more staffing.
As part of assessing the impact of our service, we chose as criterion the proportion of patients who died in the hospital and had been followed by the palliative care service. This number more than doubled over a 15-month period, indicating a gradual, greater involvement of the palliative care service in the care of terminally ill children.
Conclusions
A large part of what our program accomplished in its early years resulted from learning from mistakes and reconfiguring clinical and marketing strategies. The goal of our report here was to provide generalizable and specific strategies to help other new programs find success. As we move forward, we plan to elaborate our survey research and enhance the usability of our clinical database to maximize the application of data to program development. The success of our program confronts us with the challenge of not only expanding our resources to meet the demands of the caseload, but also of identifying ways to sustain the program beyond temporary financial support from the administration.
Footnotes
Author Disclosure Statement
No competing financial interests exist.
Appendix
| CC: |
| HPI: |
|
|
|
|
|
|
|
|
| The Comfort and Palliative Care Service will follow, |
| Call for any issues or questions Monday – Friday from 8am – 5pm. |
| Total Time Spent: _______________, the majority of time spent (> 50%) of interaction was related to counseling and information giving. |