
Abstract
Abstract
Background:
The transition to hospice care is a stressful experience for caregivers, who report high anxiety, unpreparedness, and lack of confidence. These sequelae are likely explained by the lack of an accurate cognitive schema, not knowing what to expect or how to help their loved one. Few interventions exist for this population and most do not measure preparedness, confidence, and anxiety using a schema building a conceptual framework for a new experience.
Objective:
The purpose of this study was to test the feasibility and preliminary effects of an intervention program, Education and Skill building Intervention for Caregivers of Hospice patients (ESI-CH), using an innovative conceptual design that targets cognitive schema development and basic skill building for caregivers of loved ones newly admitted to hospice services.
Design:
A pre-experimental one-group pre- and post-test study design was used. Eighteen caregivers caring for loved ones in their homes were recruited and twelve completed the pilot study. Depression, anxiety, activity restriction, preparedness, and beliefs/confidence were measured.
Results:
Caregivers reported increased preparedness, more helpful beliefs, and more confidence about their ability to care for their loved one. Preliminary trends suggested decreased anxiety levels for the intervention group. Caregivers who completed the intervention program rated the program very good or excellent, thought the information was helpful and timely, and would recommend it to friends.
Conclusions:
Results show promise that the ESI-CH program may assist as an evidence-based program to support caregivers in their role as a caregiver to a newly admitted hospice patient.
Introduction
Building a cognitive schema of what to expect may be one strategy to decrease caregivers' possible anxiety and enhance their preparedness and confidence for the new experience of caring for dying loved ones. Johnson's self-regulation theory defines a cognitive schema as a picture in a person's brain that contains knowledge and meaning about an experience and provides a way to interpret one's experience. 3 Specific, detailed, concrete, objective information leads to an accurate cognitive schema. When used with family caregivers of newly admitted hospice patients, a cognitive schema will likely allow caregivers to experience a new situation with confidence and preparation for their role, to plan actions to cope with new experiences, to set priorities for using resources, and to effectively obtain additional information. Thus, caregivers may be less anxious and feel more confident and prepared to care for their dying loved ones. To date, no study has used self-regulation and role theories for caregivers of hospice patients.4–6 The purpose of this study was to test the feasibility and preliminary short-term effects of an education and skill building intervention for family caregivers of loved ones newly admitted to hospice.
Education and Skill building Intervention for Caregivers of Hospice patients (ESI-CH) Intervention
Based on self-regulation theory, the research team developed a conceptual framework (see Figure 1) to guide development of a schema and skill building intervention to provide caregivers with information and caregiving skills for their new caregiver role. 7 Role theory was added to address caregiving skills needed for this role. Information content included four domains: (1) the range of possible physical sensations and symptoms pertaining to the dying patient and the caregiver, (2) the range of possible causes of the sensations and symptoms experienced by both the patient and the caregiver, (3) possible temporal characteristics for both the patient and caregiver, and (4) possible environmental features. 3
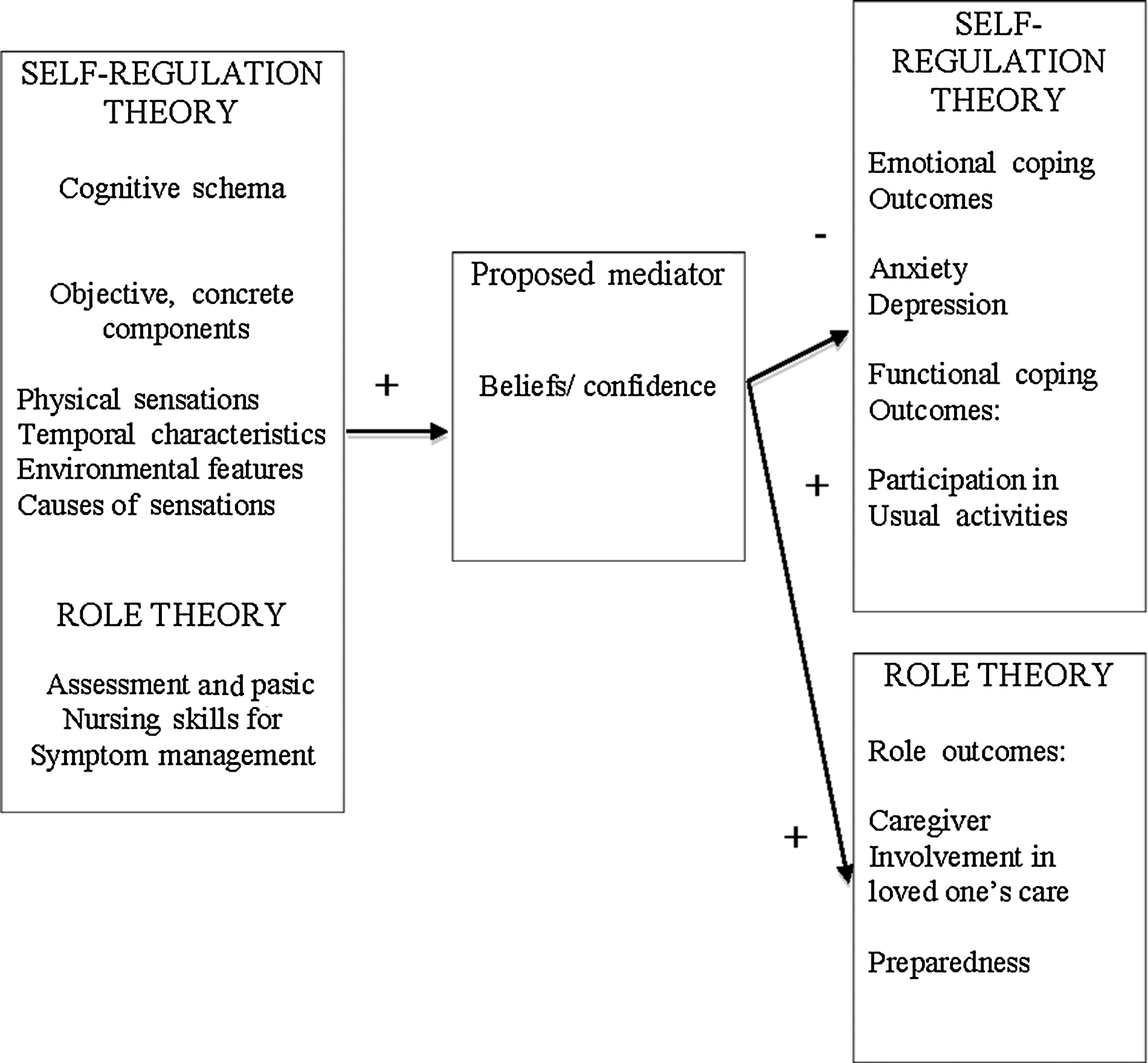
ESI-CH theoretical framework
The ESI-CH program consisted of two sessions on a professionally recorded compact disc (CD). Session One included a 30-minute CD addressing what to expect when a person is expected to die within three to four months. Session Two consisted of an 18-minute CD and covered the final three days to 24 hours of life. At the end of each session, participants chose two additional topics, based on their particular role and the severity of their loved one's symptoms. Additional topics included (1) pain, (2) dyspnea, (3) eating and drinking issues, (4) delirium, (5) fatigue and weakness, and (6) caring for the caregiver.
Methods
Design
A pre-experimental one-group pretest-posttest design was used to test the feasibility and preliminary effects of ESI-CH for family caregivers of loved ones newly admitted to hospice home care services.
Participants
After institutional review board and hospice approval, family caregivers were recruited to participate in the study from a hospice company. Inclusion criteria included (1) being a caregiver of a newly admitted hospice patient, living with the patient, and 40 to 85 years of age; (2) ability to read, write, and speak English; (3) lacking a dementia diagnosis and lacking a hearing disorder; and (4) a patient's Palliative Performance Scale score of 40 or more.
Measures
Feasibility measures
A Likert scale (1–5) evaluated the overall experience of the program. Program feasibility was evaluated via yes/no items and open-ended questions regarding (1) helpfulness, (2) timing, (3) whether participants would recommend the program to friends, (4) length of the program, (5) ease of using the CD player, and (6) acceptability of the program manual and CD format. Five multiple-choice questions evaluated participants' understanding of each session.
Depressive symptoms were measured by the 20-item, 4-point Likert scale Center for Epidemiological Studies-Depression (CES-D) scale (alpha=.89), with higher scores indicating depressive symptoms. 8 A cut-point score of 16 was used to differentiate someone at risk for suicide.
Anxiety was measured using the State-Trait Anxiety Inventory, comprised of two self-report 20-item scales on a 4-point Likert scale, where higher levels indicate anxiety. 9 Cronbach alpha was .93 on the State Anxiety (A-State) scale and .90 on the Trait Anxiety (A-Trait) scale.
An adapted version of the Caregiver Activity Restriction Scale measured the degree to which a caregiver's activities were restricted due to his or her caregiver responsibilities. 10 Higher scores indicated that individuals' activities were restricted by their caregiving role. Cronbach alpha ranged from .85 to .86.
Preparedness
The 5-point Likert scale Family Preparedness Scale measured caregivers' perception of feeling prepared. 11 Higher scores indicated greater feelings of preparedness. Cronbach alpha was .88.
Beliefs/confidence
The adapted Family Beliefs Scale for Caregivers of Hospice patients (FBS-CH) included 20 statements about a caregiver's confidence in what to expect and confidence level in helping the loved one. 7 Higher scores indicated stronger belief and confidence in caregiver abilities. Cronbach alpha was .95.
Procedures
Eleven trained hospice registered nurses (RN) recruited caregivers during the first primary nurse visit (see Table 1). Caregivers who were interested in participating in an education and skill building program for family caregivers of newly admitted hospice patients made an appointment during the next two days to sign the informed consent. Caregivers received $20 at each of two data collection appointments. If a participant's loved one died prior to the completion of the study, caregivers left the study but kept all materials and money up to that point.
CD, compact disc; ESI-CH, Education and Skill building Intervention for Caregivers of Hospice patients; PI, principle investigator; RN, registered nurse; T0, T1, T2, T3, Time 0, Time 1, Time 2, Time 3.
Data analysis
Data analysis was performed using SPSS 18.0 (SPSS Inc., Chicago, IL) for Apple software. Descriptive statistics were computed on all variables. Participants' open-ended comments on program feasibility were analyzed through content analysis. Paired t tests determined the preliminary effects of ESI-CH from pre- to post-intervention. A significance level of .10 was used to minimize a type II error. 12
Results
Eighteen caregiver participants enrolled between the months of September 2009 and January 2010 (see Table 2). Twelve participants completed the study. Caregivers rated the ESI-CH program very highly (see Tables 3, 4, and 5). Overall, results from the ESI-CH program were statistically significant from pre- to post-intervention in improving participants' beliefs and confidence (p=.04) in what to expect and improving feelings of being prepared (p=.09). Depressive symptom mean scores were relatively unchanged from pre- to post-intervention. While decline in anxiety from pre- to post-intervention was not statistically significant, there was a trend toward lowering anxiety post-intervention (see Table 6). The decrease in anxiety from pre- to post-intervention was statistically significant for a subset analysis of 13 caregivers reporting high anxiety.
CD, compact disc; ESI-CH, Education and Skill building Intervention for Caregivers of Hospice patients.
ESI-CH, Education and Skill building Intervention for Caregivers of Hospice patients; RN, registered nurse.
p<.10
p<.05
p<.01
Cohen d
+small effect
++medium effect
+++large effect
A-State, State Anxiety; CARS, Caregiver Activity Restriction Scale; CES-D, Center of Epidemiological Studies-Depression; CI, confidence interval; ESI-CH, Education and Skill building Intervention for Caregivers of Hospice patients; FBS-CH, Family Beliefs Scale for Caregivers of Hospice patients; PREP, preparedness; Diff, difference; T0, Time 0; T3, Time 3; Cohen d, significant effects.
Discussion
This study tested the feasibility and preliminary effects of an innovative intervention targeting schema development for caregivers of newly admitted hospice patients. Not only did caregivers highly rate the intervention format—they felt less anxious and more prepared and confident in their caregiver role. Preparedness is a key component in helping caregivers to perform in a role, and yet few studies measure preparedness. Improving caregivers' preparedness to care for dying loved ones and decreasing caregiver anxiety are important. 13 Although a recent problem solving intervention reported a decrease in anxiety, preparedness and belief and confidence levels were not measured, making it challenging to know how the caregiver felt about his or her ability in a caregiver role. 6
Caregivers positively rated the CD and written materials, felt the timing was appropriate, and would recommend it to friends (see Table 3). Additionally, caregivers reported how the program increased their understanding for what to expect in their loved one's disease trajectory and care needs (see Table 4). They wished they had had this information years prior to the initiation of hospice to more optimally care for their loved one.
The content of the ESI-CH program delivers information and was chosen based on studies that report the significance of providing information to develop a schema for new experiences.7,14,15 When a schema fits the new experience, individuals are better able to navigate experiences with confidence and hope that they are providing good care to their dying loved one.
Limitations
Although preliminary results show promising positive effects for a cognitive schema building program in decreasing anxiety and improving levels of preparedness and confidence levels for caregivers of newly admitted hospice patients, findings from this study should be cautiously interpreted due to a small sample and one-group design.
Conclusions
The ESI-CH program is based on an innovative framework to build a schema for caregivers of dying loved ones. These results suggest that ESI-CH is a promising intervention for building a cognitive schema to decrease anxiety and increase preparedness and confidence for people caring for dying loved ones. This pilot study adds to the body of interventional science for caregivers of hospice patients by using a new conceptual framework. Future research should include two groups and care receiver outcomes to further evaluate this preliminary efficacious intervention in supporting caregivers caring for their dying loved ones.
Footnotes
Acknowledgments
Funding for this study was supported by a National Research Service Award (NRSA) pre-doctoral fellowship from the National Institutes of Health/National Institute of Nursing Research (#1F31NR010418-01).
Thank you to all the caregivers, patients and staff of a mid-south hospice company. A special thanks to Terrah Foster, PhD for her guidance on editing this manuscript.
Author Disclosure Statement
No competing financial interests exist.