
Abstract
Abstract
Background:
Community physicians are often ill-prepared for the management of complex symptoms. With a shortage of board certified physicians in palliative medicine to assist, the result is a lack of access to critical pain and symptom management expertise to care for seriously ill Californians. We report on a palliative medicine telephone hotline available to health care professionals.
Methods:
San Diego Hospice and The Institute for Palliative Medicine received a grant to provide a telephone hotline for health care professionals to assist in answering clinical questions relating to palliative care. An extensive marketing campaign was initiated to publicize the service. Information from the calls was collected over a 2.5-year period. The data included referral source, geographic area, diagnosis, and reason for call. Satisfaction surveys were sent following each call.
Results:
During the first 2.5 years of operation 498 calls were recorded. Although marketing was directed within the state of California, the majority of calls originated outside the state after the first year (66%). Approximately 43% of calls came from physicians, followed by 22% from registered nurses, 15% from nurse practitioners, and 6% from pharmacists. Nearly half of the calls were received from repeat callers. The most frequent topics for callers were related to pain and symptom management (29%), followed by hospice care (21%), medication dosing, and general palliative care (14% each). Ninety-five percent of the callers completed the satisfaction survey with 89% likely to use the service again.
Conclusions:
The hotline proved to be a valuable resource for health care providers caring for patients requiring palliative care as evidenced by the steady increase in the number of calls over the initial 2.5 years of operation. Future research on how the information directly impacted patient care might generate data to support the continuation of this service via partnerships with other organizations.
Introduction
In 2008, The Institute for Palliative Medicine at San Diego Hospice received a grant to develop and implement a palliative care hotline available to all health care providers in California. The hotline aimed to provide “curbside consultation” to primary care providers caring for patients suffering with life-limiting illnesses. Review of the literature found only four other services that provided palliative care consultation services over the phone, only one of which was based in the United States.7–10 This program originated in the state of Maryland and reported 56 calls in 10 months of service. 7 The second service in the United Kingdom reported 93 calls in the first year. 8 In 2007, a telephone consultation service in The Netherlands reported on 5 years of experience with a telephone consultation palliative care hotline for cancer patients, not providers. 9 Lastly, a telephone consultation service in British Columbia, Canada, reported receiving 692 calls for palliative medicine assistance from family doctors and registered nurses over a 4-year period. 10
The primary goal of PAL-MED CONNECT
We describe the calls received by PAL-MED CONNECT
Methods
The Institute for Palliative Medicine at San Diego Hospice (SDHIPM) employs 18 board-certified palliative medicine physicians and seven hospice nurse practitioners (NPs). The Institute has the largest physician fellowship training program for palliative medicine in the United States. It also has internship programs for pharmacists, NPs, and counselors specializing in the treatment of hospice and palliative care patients. SDHIPM is recognized internationally as a focal point for palliative care education.
Funding for a toll-free telephone hotline for questions relating to palliative care was provided through a grant from PacifiCare/UnitedHealthcare in 2008. After a 6-month planning process, the hotline was launched in July 2009 in San Diego County as part of the pilot testing process and statewide in California in September 2009. A marketing strategy was developed to introduce clinicians in California to the PAL-MED CONNECT® hotline resource. The PAL-MED CONNECT® team initially worked with local associations and SDHIPM staff to promote the hotline to various medical centers and clinics in San Diego. Marketing activities were expanded to include members of the target audiences throughout the state of California via mailings, press releases, e-mail updates, and attendance at specialty conferences and the AAHPM annual meeting. SDHIPM clinicians included a PAL-MED CONNECT® slide at the conclusion of their presentations to further promote the hotline. Through these presentations and electronic media, information about PAL-MED CONNECT
The hotline was answered 24 hours per day, 7 days per week by a SDHIPM customer service advocate, who immediately paged the NP first responder. Response time was generally within 15 to 30 minutes. Nurse practitioners trained in palliative care were first responders, answering the calls from 8:00
Callers were asked basic patient information such as age, race, diagnosis, results of relevant diagnostic tests, list of medications, and symptom issue(s). Discussion surrounding the specific symptom was recorded with disclaimer that responders did not assume responsibility for care of the patient. If further assistance was needed, the NP responder was responsible for collecting additional information or referring the call to another member of the team. No specific patient identifying data were obtained. A satisfaction survey was sent to all callers following their inquiry to determine caller satisfaction with the service. The survey was developed by the PAL-MED CONNECT® team after reviewing in-house and satisfaction survey forms from other entities; two satisfaction surveys served as the primary resource: the SDHIPM patient satisfaction survey and the University of California, San Francisco's satisfaction survey for the National HIV Telephone Consultation Service (Warmline). 11 The survey form included open-ended questions to encourage more detailed information regarding the caller's experience with the PAL-MED CONNECT® hotline.
First responders collected demographic information from each caller that included caller name, profession, location, phone number, gender, race, referral source, and responder completing the call. The objective of the PAL-MED CONNECT® hotline was to reach clinicians who lack access to palliative medicine expertise as there are a limited number of board-certified clinicians in palliative medicine in rural California communities. Location information was obtained to determine if the hotline was reaching the target clinicians. Data were entered into a custom designed SQL database and stored on a secured network server. There were specific a priori questions about how geographic location (rural versus urban) and number of repeat callers would change over time. These were analyzed using one-way analysis of variance (ANOVA) repeated measures.
To provide the most up-to-date information for callers, the PAL-MED CONNECT® team collected and organized a resource database. The database included numerous journal articles, book excerpts, and the latest research on palliative medicine topics and pharmaceutical interventions.
Quality control meetings were held quarterly to ensure consistent information was provided to callers regardless of who was responding to the call. Several quality measures were reviewed including the advice and educational materials discussed with callers, call response times, and caller follow-up satisfaction survey responses.
Results
A total of 498 calls were received over the 2.5-year grant period (July 2009–December 2011). The number of calls rose steadily during this time. In the last half of 2009, assistance was provided to 63 callers with 33 calls originating within the state of California. In 2010, 174 calls were made to the hotline with 82 originating within the state of California and 92 outside the state. In 2011, 261 clinicians called the hotline, 90 within the state of California and 171 nationwide (Fig. 1). Although marketing was targeted to providers within California, a majority of the calls came from outside the state (66%).
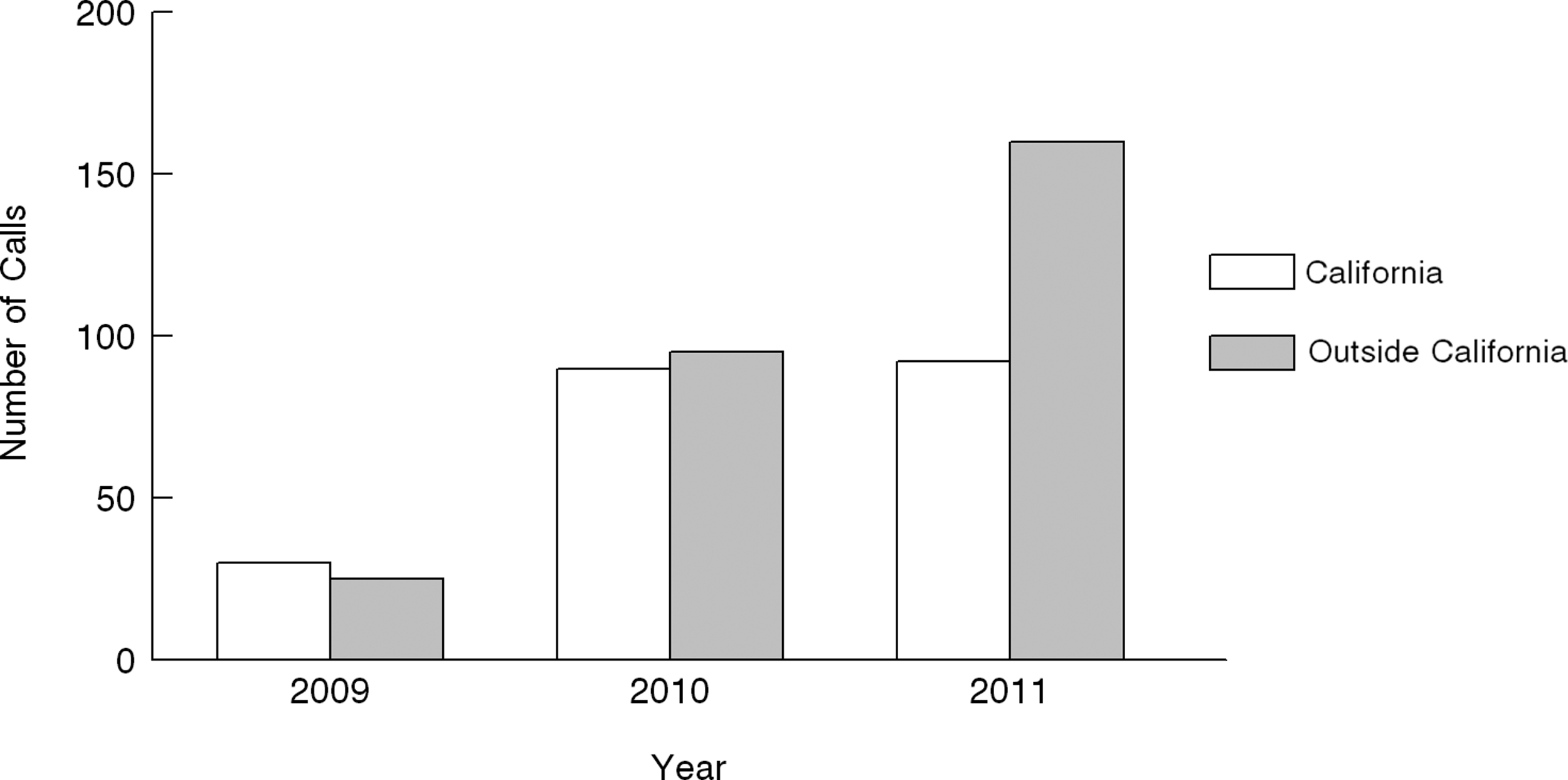
Number of calls to the PAL-MED CONNECT® hotline.
Calls to the hotline were received from a range of health professionals. Approximately 43% of calls came from physicians, followed by 22% from registered nurses, 15% from NPs, and 6% from pharmacists. A majority of the physicians identified themselves as palliative medicine providers.
Most calls (n=498) were answered by the NP first responder (n=403 calls, 81%), with pharmacists (n=29, 6%) and psychiatrists (n=13, 3%) providing significant support on specialty topics. However, the numbers do not reflect the collaborative process employed by the NP responders as they frequently solicited additional information from SDHIPM physicians as part of their response to the caller.
The largest source of calls to the hotline was repeat callers (n=178), beginning in the last quarter of year 1 and continuing across each following quarter. A statistically significant difference was seen with source of referrals, with significantly more repeat callers over time (F(8,72)=58.18, p<0.0001). The second highest source of referrals resulted from individuals at conferences attended by the PAL-MED CONNECT® team (n=85, 18%), with “word of mouth” (n=47, 10%) and personal reference (n=42, 9%) also important sources of referrals (Fig. 2).
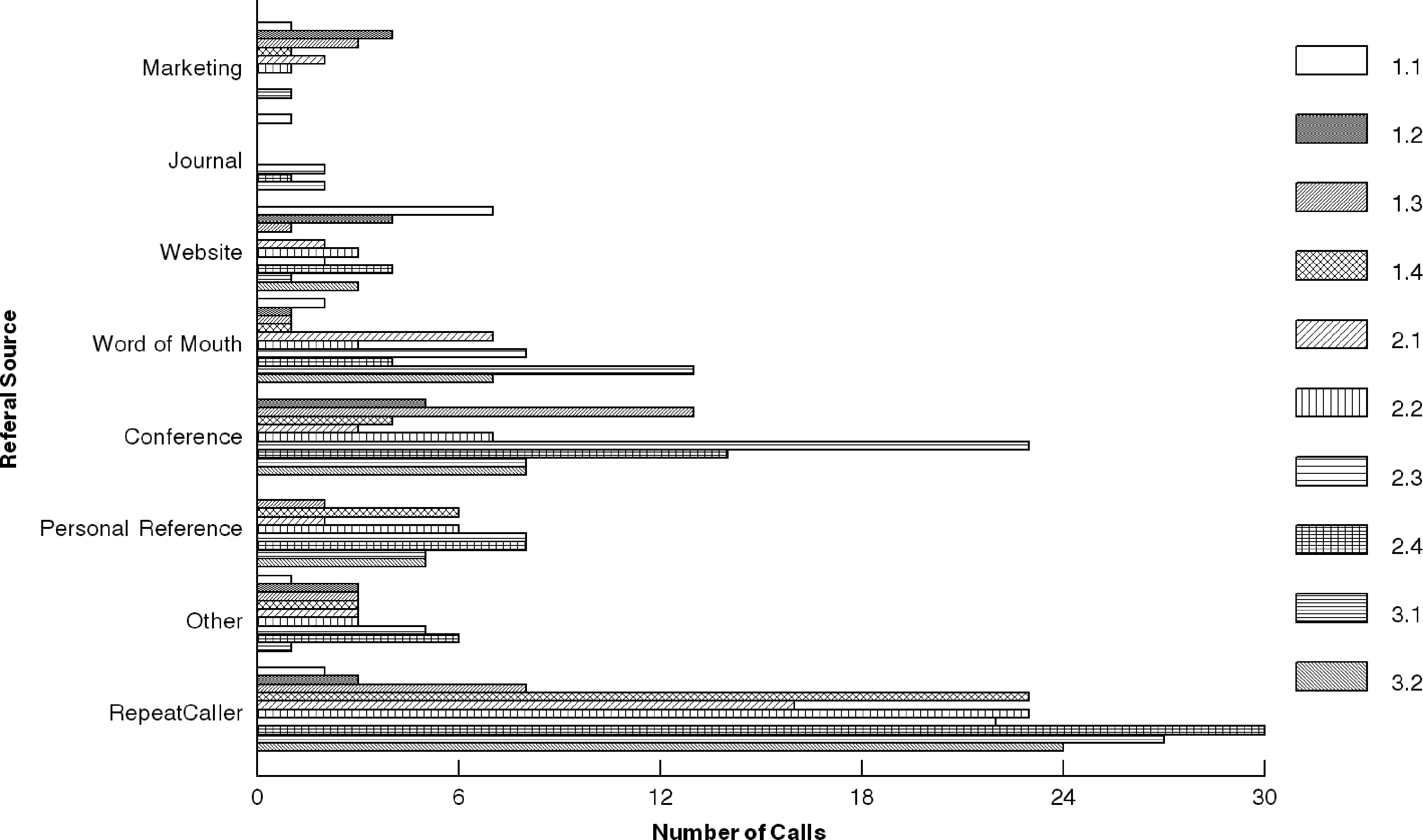
Referral source of calls to the PAL-MED CONNECT® hotline.
Callers were asked to provide their geographic location in order to track calls from rural versus urban areas. Most calls originated from urban areas in California (n=158, 33%), followed by rural areas in other parts of the United States (n=122, 25%), urban areas in other parts of the country (n=114, 24%), and rural areas in California (n=47, 10%). Overall, calls from rural areas accounted for 35% of all calls (Fig. 3). Analysis of the location of the caller over time reveals there was a main effect for location (F(5, 45)=53.83, p<0.001), a main effect for study quarter (F(9, 45)=2.18, p=0.014), and a location by study quarter interaction (F(9, 45)=2.901, p=0.086). The simple effects for location over time found that there was no significant change in the number of calls not recorded or from international sources. Calls from within California (both urban and rural) remained steady over time and showed no significant change. Calls from urban areas outside of the state of California did not change significantly, whereas calls from rural areas outside of the state of California showed a significant increase (p<0.001) over the course of the study; quarters 2.3 and 2.4 were significantly higher than the other quarters (p values<0.01). More calls were made from urban areas within California (p<0.001) and rural areas outside California (p=0.37), with no significant difference among the other locations.
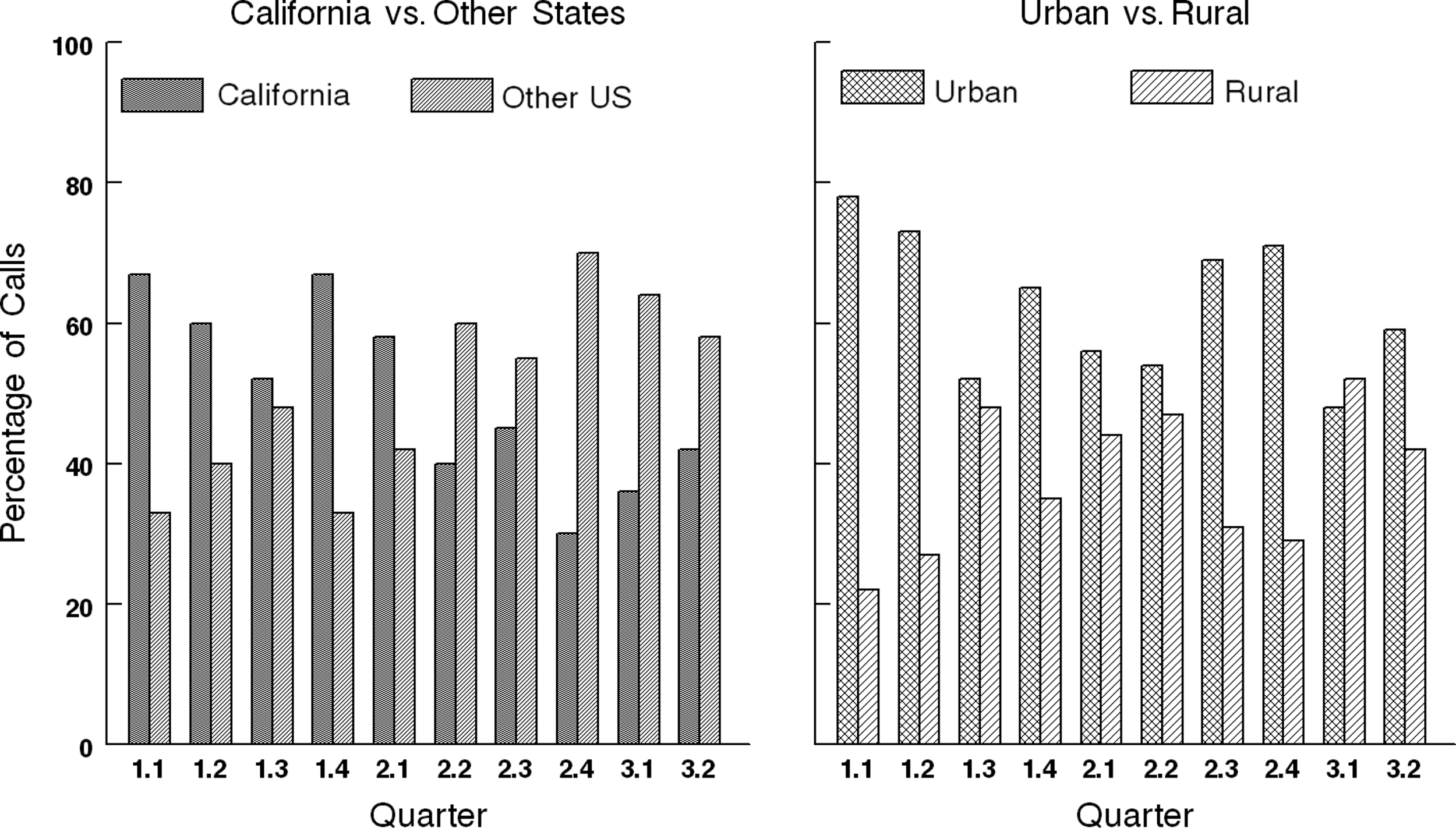
Geographic location of callers to the PAL-MED CONNECT® hotline.
The most frequent topics for callers were related to pain and symptom management (29%), followed by hospice care (e.g., billing, hospice diagnosis criteria; 21%), medication dosing and general palliative care (e.g., the difference between palliative and hospice care; 14% each) (Table 1). Several calls were received requesting information on cancer management (11%) and aromatherapy (3%), a service pioneered by SDHIPM.
To assess the quality of the service, relevance of the information provided and caller satisfaction, an automated follow-up survey was created. The vast majority of callers completed the survey (95% response rate), which we believe is indicative of the positive response to the PAL-MED CONNECT® service. As seen in Table 2, the majority of callers strongly agreed they were pleased with the consultation (80%), would use the service again (89%), and would recommend the service to a colleague (88%). The great majority also strongly agreed (79%) that the information was presented clearly, was up to date (77%), and the responding clinician was knowledgeable about the topic under discussion (74%).
Callers were also given the opportunity to share their experience with the hotline:
I am thrilled to have this resource. I am the Director of Hospice here at.…I have posted the PAL-MED number for my staff. Thank you for this service! – Physician
It was so helpful to talk with someone who is comfortable with specific uses of medications in the hospice/palliative medicine setting and the information will positively impact our patient care. – Registered Nurse
Thank you, it is really a relief to have help when you work solo in that field. – Registered Nurse
Discussion
PAL-MED CONNECT® offers a unique service to callers as there is currently no other service of its kind in the United States. The hotline proved to be a valuable resource for health care providers caring for patients requiring palliative care as evidenced by the steady increase in the number of calls over the initial 2.5 years of operation.
The majority of callers identified themselves as palliative medicine specialists. Although marketing was directed to primary care providers, it was surprising to learn that many of these providers did not understand or recognize the value of palliative care. Many primary care providers viewed palliative care as synonymous with end-of-life care and thus failed to recognize the opportunity for assistance in managing serious chronic conditions. We found face-to-face education with providers to be the most effective means for promoting the hotline. Reaching providers in rural areas proved to be challenging. Unfortunately, funding was limited to the larger conferences so smaller health care meetings in target areas could not be included in the marketing plan. Outreach takes time and resources to build rapport with primary care providers. Future plans should include additional resources to allow for greater one-on-one interaction with providers in rural or remote areas. Palliative care practitioners, on the other hand, reported they often felt isolated in their practices as they had no colleagues to consult with locally. The hotline proved to be a much-needed source of support. Discussions were held with a national organization about a partnership that would support marketing the hotline. Although external funding for the hotline is no longer available, SDHIPM continues to respond to questions regarding palliative care.
Several trends were identified with the nearly 500 calls. The value of the service is evidenced by its repeat usage. Although the number of calls received was not as high as originally estimated, it is significant that more than 49% of the calls were from repeat callers. Many of the comments from the satisfaction surveys reflected satisfaction with the hotline and requests for continued service.
The decision to have an NP as the first responder proved to be a good choice. The NP first responders were specialists in palliative medicine with extensive experience in the field. A total of 43% of the calls came from registered nurses, NPs, and pharmacists. The NP first responders were able to answer their questions with the information from the resource database and their own experience. In fact, the NP first responders were able to answer most of the questions from the community physicians as well. Backup was always available from a pharmacist and/or physician, and the caller could request to speak with a specialist. It was also interesting that callers often began the conversation with a request to speak with a certain professional, but actually needed something entirely different. Many of the inquiries involved requests for policies or procedures on a variety of palliative care topics such as subcutaneous infusions and aromatherapy.
Despite the fact that marketing the hotline was focused within California, a majority of the calls originated outside the state as word spread throughout the palliative care community. In addition, several e-mail requests originated outside the United States. A key objective of the grant was to reach providers in rural areas with limited access to palliative care expertise. Approximately 35% of calls originated from clinicians located in rural areas with limited consultants. Comments from clinicians in rural areas across the country lacking palliative care resources demonstrate the importance of this service. Sustainability of a national hotline is a challenge as funding is not readily available for this type of service. Future research on how the information directly impacted patient care might generate data to support the continuation of this service via partnerships with other organizations.
Footnotes
Acknowledgments
We would like to thank nurse practitioners Sarah Livermore and Roger Strong at San Diego Hospice and The Institute for Palliative Medicine for their willingness to act as first responders. We would also like to thank our funders, PacifiCare/UnitedHealthcare, the members of the quality control committee, Rosene Pirrello, R.Ph., SDHIPM pharmacists, Dr. Laurel Herbst, Dr. Charles von Gunten, Dr. Steven Oppenheim, and the SDHIPM physicians for their consistent support of the hotline.
Author Disclosure Statement
No competing financial interests exist.