
Abstract
Abstract
Background:
The longer-term effects of opioids for breathlessness are not known in people with chronic heart failure (CHF).
Objective:
Our aim was to assess the longer-term effect of oral opioids on breathlessness due to CHF.
Methods:
We conducted a 3-month open-label extension to a crossover randomized controlled trial (RCT) comparing 4 days of morphine, oxycodone, and placebo. Thirty-five participants from a tertiary cardiology clinic completed the RCT. Thirty-three were followed for 3 months, continuing open-label opioids if they wished. Thirteen participants continued an opioid; 20 did not. Four measures of breathlessness intensity (0–10 numerical rating scale [NRS] and modified Borg score, each recording worst and average breathlessness during 24 hours) were combined using principal component analysis to give a single measure for the primary analysis. Groups were compared using analysis of covariance. Secondary measures included quality of life (SF-12® Health Survey), cardiorespiratory, and global impression of change in breathlessness at 3 months.
Results:
At 3 months, the composite breathlessness measure improved to a greater extent in the opioid group (p=0.017). The opioid group had an improvement in global impression of change (mean 2.62 [opioids] versus −0.65 [nonopioids]; p=0.0009). The SF-12 physical component improved more in the opioid group (p=0.014). Cardiorespiratory variables were unchanged.
Conclusions:
Opioids given for 3 months were well tolerated and safe. Opioid-related improvement in breathlessness in people with CHF might not be seen until longer-term administration. We cannot conclude from these data that they are effective and a longer-term RCT is needed.
Introduction
Opioid receptors are found throughout the cardiorespiratory system. Overactivity of the sympathetic nervous system, breathlessness, and endogenous opioid production may be linked. Sympathetic activation leads to an enhanced ergoreflex mediated ventilatory response to exercise. 2 As a possible counteracting system, endogenous opioids are released as part of the neurohormonal response to CHF3–5 : Opioid receptor activation inhibits sympathetic drive by reducing intracellular cyclic adenosine monophosphate (cAMP),6,7 suggesting that exogenous opioids might modify both breathlessness and sympathetic activation. However, physicians may be reluctant to use opioids for fear of adverse events, despite evidence that monitored low-dose oral morphine is safe. 8
Opioids are more commonly thought of as an analgesic, and although pain appears to be a problem for many people with CHF, 9 for whom opioids may be helpful, the use of opioids for breathlessness is less well recognized. A Cochrane review and meta-analysis found that there was an improvement in breathlessness with oral and parenteral morphine or diamorphine compared with placebo. 10 A subsequent adequately powered randomized placebo-controlled trial confirmed benefit with morphine. 11 However, most participants included in these studies had refractory breathlessness due to cancer or chronic obstructive pulmonary disease (COPD). The only previous repetitive dosing randomized controlled trial (RCT) in people with advanced CHF showed improvement of breathlessness with morphine, but the study was a pilot. 12
We therefore conducted a trial comparing short-term (4 day) low doses of two opioids (Oramorph™ [morphine] and OxyNorm™ oxycodone]) versus placebo in a three-arm crossover RCT in patients with symptomatic CHF 13 (trial number ISRCTN 85268059). The study was powered to show a difference of 1 point on a numerical rating scale of patient-rated intensity of breathlessness (0=no breathlessness to 10=the worst breathlessness imaginable) with 80% certainty. We found no statistically significant difference among the study arms. Following the RCT phase of the study, participants were able to choose to continue with opioids for a further 3 months. We report here on the effect of longer-term opioid treatment on breathlessness in the first study in people with CHF to last for more than 4 days.
Methods
The details of the methods and justification of outcome measures are reported elsewhere. 13 Adults with CHF due to left ventricular systolic impairment (defined as ejection fraction of <45% on transthoracic echocardiography) and in New York Heart Association functional class III or IV were recruited. They had to be on standard medical therapy (diuretics and angiotensin converting enzyme inhibitor [ACEI] or angiotensin receptor blocker [ARB] and beta blocker [BB], which had been unchanged for at least one month). Participants were randomized into a three-way double-blind placebo-controlled crossover RCT comparing Oramorph with OxyNorm and placebo. Participants were assessed at baseline, day one, day one hour one, and then daily for 4 days on therapy. This was followed by 3 days washout prior to the next intervention. The process was repeated for each of the three interventions.
Participants were asked at the end the RCT, while still blinded, which of the three interventions they preferred (Oramorph, OxyNorm, or placebo). In a nonrandomised observational extension to the main study, participants were given the option of continuing their preferred therapy if this was an active treatment (the “opioid” group). Those not wishing to continue or those who selected placebo did not receive further opioids (the “nonopioid” group). All participants, whether taking opioids or not, were followed up for 3 months. Our study complies with the Declaration of Helsinki, the research protocol was approved by the Leeds East Ethics Committee UK, and written informed consent was obtained from all participants.
Participants opting to continue an open-label opioid, but who then either declined to take it, or did not take it regularly, were still classed as being in the opioid group. Likewise, if participants opting not to continue with opioids did use opioids during their follow-up, they were classed as being in the nonopioid group.
Study measurements
Baseline assessments were made as part of the RCT. After 3 months, participants completed a final assessment of breathlessness scores, quality of life using the SF-12, 14 and physical ability using the Karnofsky Performance Status Scale. 15
We used four measures of breathlessness intensity: an 11-point numerical rating scale [NRS] and a modified Borg score, each recording worst and average breathlessness during the previous 24 hours.16,17 The NRS measures patient-rated intensity of breathlessness on a scale of 0=no breathlessness to 10=the worst breathlessness imaginable. Following the recommendations of a consensus statement and the authors of systematic reviews, we recorded average and worst breathlessness over the past 24 hours for both the Borg and NRS.18–20 The NRS is validated for use in chronic breathlessness, 17 and is the primary outcome measurement scale used in recent studies of refractory breathlessness due to a variety of advanced diseases.21–23 In addition, we measured the patient's global impression of change in breathlessness score from baseline to 3 months (−7 “a very great deal worse” to +7 “a very great deal better”) (see Box 1). 24 Distress, satisfaction, and coping with breathlessness were also assessed using an 11-point NRS. We also measured N-terminal pro B-type natriuretic peptide (NT-proBNP) at baseline and 3 months.
Box 1.
Participant-reported increments on the Global Impression of Change scale. Increments may show an improvement or worsening of breathlessness (−7 to +7) or can be rated as the same (value=0). A one-point increment is defined as the lowest detectable change in an individual.
In the RCT, the question was phrased as:
• • •
[Continue if participants indicate a worse or better response]
1. ALMOST THE SAME, HARDLY ANY BETTER / WORSE AT ALL 2. A LITTLE BETTER / WORSE 3. SOMEWHAT BETTER / WORSE 4. MODERATELY BETTER / WORSE 5. A GOOD DEAL BETTER / WORSE 6. A GREAT DEAL BETTER / WORSE 7. A VERY GREAT DEAL BETTER / WORSE
Statistical methods
For outcome variables, the two groups of participants were compared using analysis of covariance on baseline measure. Logarithmic transformations were used where distributions were highly skew. To allow for the problem of multiple testing with breathlessness variables, the four scales of intensity were combined using principal component analysis. The first principal component is the single combination of the four breathlessness measurements, which contains the maximum information. Principal component analysis was carried out for the baseline breathlessness variables before the groups were formed. The coefficients for the first component were used to calculate the component using the breathlessness variables observed after 3 months. We took this as the primary outcome variable and decided that we would only consider that we had a significant difference if this principal component calculated for the outcome variables produced a significant difference between the groups after adjustment for the component calculated at baseline. For observations at baseline, demographic and clinical, we compared groups using Fisher's exact test for categorical variables and the two-sample t test for quantitative variables.
Results
Of the 35 participants who completed the RCT, 23 said they preferred a study arm with an opioid prior to unblinding. Eleven preferred the placebo arm. One did not feel any intervention was better than any other. The order of interventions in the RCT did not affect the preference. Those participants preferring an opioid were given the option to continue that opioid for 3 months. Two participants were lost to follow-up (one moved abroad and one declined further assessment) and included the participant who did not express a preference, leaving 33 participants who completed the 3-month assessment. There were 13 who chose to continue opioids and 20 who did not, although 11 of these 20 had stated a preference for the opioid in the double-blind phase.
Description of the two groups
Of those who chose to continue to take opioids (seven OxyNorm and six Oramorph), eight took their medication regularly either 3 or 4 times daily; five took their opioids only “as required” for breathlessness. Of the five, two stopped regular treatment due to abdominal cramps or diarrhea.
Demographic data for the two patient groups are shown in Table 1. There was no difference in age or sex. The opioid group tended to have worse renal function, lower ejection fraction, and higher NT-proBNP measurements, although these differences were not statistically significant.
After logarithmic transformation.
ACEI, angiotensin converting enzyme inhibitor; ARB, angiotensin receptor blocker; BB, beta blocker; DCM, dilated cardiomyopathy; EF, ejection fraction; eGFR, estimated glomerular filtration rate; IHD, ischaemic heart disease; NT-proBNP, N-terminal pro-beta-natriuretic peptide; NYHA, New York Heart Association; RCT, randomized controlled trial; SD, standard deviation.
Change in outcome measure over three months
Mean values for breathlessness measures at baseline and at 3 months are shown in Table 2 for the two groups. For the principal component, negative scores represent improvement. For NRS and Borg scores, high scores signify worse symptoms. For global impression of change, negative scores indicate deterioration.
0=no breathlessness, 10=worst imaginable breathlessness.
The change from baseline at 3 months is compared between groups. Global impression of change scores at 3 months are also included and values at 3 months compared between groups.
NRS, numerical rating scale; SD, standard deviation.
The principal component analysis yielded only one meaningful component, which accounted for 74% of the total variance. After analysis of covariance adjusting for baseline, intensity of breathlessness at 3 months was significantly improved in those who chose to continue an opioid (p=0.017). Figure 1 shows the summary measure at 3 months plotted against the measure at baseline, for each group. The figure suggests that the summary measure predominantly decreased (improved breathlessness) in the opioid group, but was unchanged in the nonopioid group. Of the four individual measures of breathlessness intensity, both NRS measures showed statistically significant improvement for the opioid group. The global impression of change in breathlessness score improved significantly in the opioid group compared with the nonopioid group.
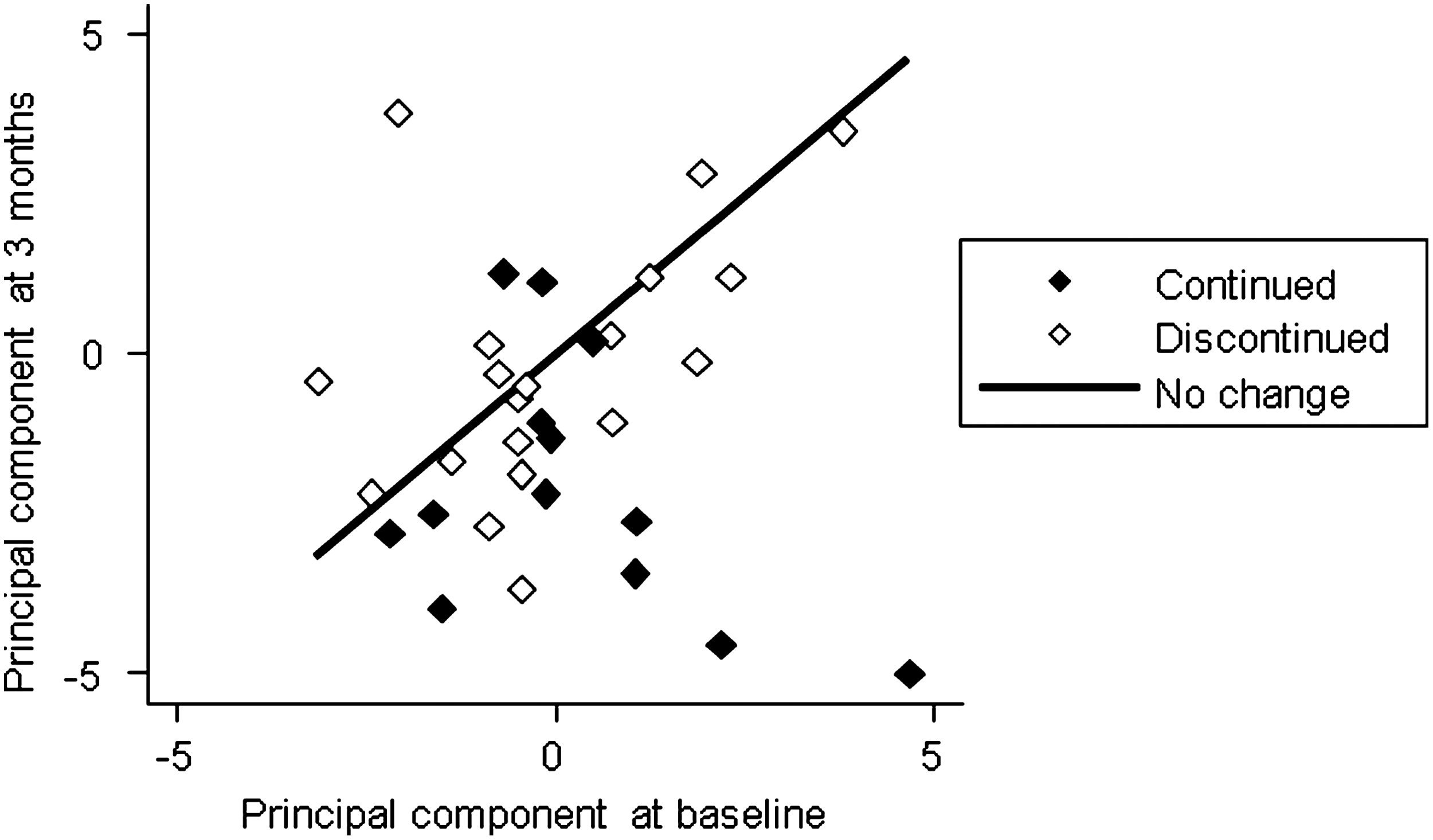
Principal component summary of breathlessness variables; 3- month values plotted against baseline values. Low values represent less breathlessness.
Distress, coping with breathlessness, satisfaction with treatment, and quality of life scores are shown in Table 3. There was a statistically significant advantage to opioids for satisfaction and the physical component of the SF-12. For Karnofsky score, in the opioid group 4/13 participants improved and 1/13 deteriorated, whereas among the nonopioid group 1/20 improved and 3/20 deteriorated (p=0.075, χ2 for trend). There were no clinically or statistically relevant differences in pulse rate, blood pressure, respiratory rate, oxygen saturation, or NT-proBNP (Table 4).
0 to 10 scales, high scores represent greater distress due to breathlessness, better coping with breathlessness, or greater satisfaction with management of breathlessness.
Mean 50, SD 10 in normal reference population, high score=high quality of life.
After logarithmic transformation.
SD, standard deviation.
after logarithmic transformation.
BP, blood pressure; bpm, beats per minute; NT-proBNP, N-terminal pro-beta-natriuretic peptide; SD, standard deviation.
Discussion
This study was an open-label extension of a short term (4 day) study. The data support the hypothesis that the benefits of opioids on breathlessness might require longer than 4 days to become apparent.
It may be that there is a group of people more likely to respond to opioids than others. We found that while blinded two thirds of participants preferred opioid to placebo, but 9/22 (41%) did not want to continue treatment into the open-label extension. A dose-titration study assessing the effect of opioids on refractory breathlessness from any etiology estimated the number needed to treat (NNT) as 1.6 in order to gain at least one point improvement on a NRS score. 8 A post hoc analysis of a study of 20 mg morphine daily for refractory breathlessness due to any cause found that younger people, those with a better performance status, and those with an underlying cardiovascular etiology for their breathlessness might be more likely to respond, 25 but the study was too small to draw firm conclusions.
Nearly half of those who felt that the opioid had helped their breathlessness chose not to continue with it for the immediate extension, and of those who did continue, several did not use it in the prescribed manner. This raises the question of net benefit in different situations and over time: Although a drug may be well tolerated in the context of a clinical trial, adverse effects may be less well tolerated in daily clinical practice and this may affect concordance. Long-term pharmacovigilance data might be helpful in determining optimal use.
In the present study we used four measures of intensity of breathlessness plus the global impression of change, so we were concerned about the possible chance findings due to multiple testing. We combined our breathlessness measures into one unified variable as a primary outcome to avoid this problem. The groups were significantly different on the combined measure, so we think that this provides evidence that the differences are real. In addition, the four individual scales and the global impression of change scale together remain significant after a Bonferroni correction, as both NRS worst breathlessness and global impression of change had p values<0.05/5.
During the 3-month extension, there was little difference among the groups in the change in the intensity of the participants' heart failure, as shown by clinical variables, particularly Karnofsky Performance Scale scores and NT-proBNP measurements, suggesting that any differences in breathlessness were not related to a change in severity of heart failure. Cardiorespiratory variables (heart rate, blood pressure, and respiratory rate) remained stable throughout the follow-up in keeping with recently reported pharmacovigilance data, 8 consistent with evidence that longer-term low-dose opioids are safe.
Breathlessness due to advanced CHF is a refractory and distressing symptom with few available helpful interventions. If the result of the present study were replicated in a randomized study, then the response would represent an important improvement for patients. The response is larger than those reported either from opioid studies of shorter duration11,12 or from studies of other interventions directed at breathlessness. 26 An adequately powered parallel-group placebo-controlled trial with 3 months follow-up is needed to test the hypothesis.
Limitations
Participants in this small study elected to continue a treatment they believed was effective and the study was unblinded and nonrandomized. These factors could have influenced the results leading to an overestimate of benefit.
Our data do not allow us to distinguish the various presentations of breathlessness (at rest, on exertion, nocturnal); although we asked patients to report their worst experience of breathlessness over the previous 24 hours, we did not ask what might have provoked it or what the person was doing at the time. Gaps remain in the evidence base for the use of opioids for breathlessness, optimally tailored for the individual; hence the need for further work. 27
Conclusions
Studies of opioids in respiratory disease show a small but statistically significant benefit. Studies of repeated dose of opioids over 4 days in CHF have not shown a benefit. Our study found opioids given for 3 months were well tolerated and safe. Opioid-related benefit for breathlessness in CHF may not be seen until longer-term administration. An adequately powered, parallel-group RCT with a longer follow-up should now test the hypothesis arising from our preliminary data.
Footnotes
Acknowledgments
This study was supported by a Clinical Research Fellowship from Hull York Medical School, which remains independent of the research process. The sponsor of the study had no role in the study design, data collection, analysis and interpretation, writing of the report, or the decision to submit for publication. All authors had access to the data in the study and take responsibility for its accuracy and integrity.
Author Contributions
SGO: Literature search; study design; regulatory approval; data collection; data analysis; data interpretation; writing. MB: Study design; data analysis; writing. ALC: Study design; data interpretation; writing. JGC: Study design; data interpretation; writing. MJJ: Literature search; study design; regulatory approval; data analysis; data interpretation; writing.
Author Disclosure Statement
No competing financial interests exist.