
Abstract
Abstract
Background:
Patients and caregivers living with advanced chronic obstructive pulmonary disease (COPD) have complex care needs and may benefit from palliative care intervention. Little is known about how best to implement and evaluate such initiatives.
Objectives:
To determine the feasibility of: 1) implementing a customized home-based palliative care service for patients and caregivers living with advanced COPD and 2) measuring outcomes of providing such services.
Design:
Single-centre cohort longitudinal observational study.
Setting/Subjects:
Patients with advanced COPD and their caregivers were followed in their homes for 6 months.
Measurements:
Health-related quality of life (HRQoL), caregiver burden, symptom severity, patient/caregiver satisfaction, utilization of acute care services, end-of-life (EOL) outcomes.
Results:
30 patients and 18 caregivers were enrolled over 33 months. 25 patients (83%) and 14 caregivers (77%) reached our study endpoint. 13 patients (52%) and 5 caregivers (36%) completed outcome measurements at baseline and endpoint. HRQoL, caregiver burden and symptom severity did not change. Palliative care services were welcomed and valued, yet, despite a stated preference to die at home, 16 patients who died within 18 months of study enrollment died in hospital.
Conclusions:
Providing home-based palliative care services for patients with advanced COPD is feasible but completing repeated questionnaires is impractical. Despite significant palliative supports, managing terminal symptoms exceeded caregivers' capacity to cope and forced hospital admission. Insights into systemic barriers and limitations of current palliative care service models can provide opportunities for local program innovation aimed at improving care for advanced COPD.
Introduction
Barriers to provision of quality palliative care in COPD include the unpredictable disease trajectory, the reality that many patients and their caregivers fail to appreciate that COPD is a life-threatening disease, 6 patients' limited understanding of treatment options, communication barriers due to attitudes of patients and health care professionals, 7 and our limited ability to judge when palliative care services might be helpful. 8
The cancer community has highlighted the need to support patients' caregivers in an effort to minimize their risk of exhaustion or burnout.9–11 Many patients in the advanced stages of COPD are housebound, and despite a protracted disease trajectory, they and their caregivers receive little support from traditional community health services.1,4,12 Professional societies—the American Thoracic Society (ATS), the Canadian Thoracic Society (CTS), and the American College of Chest Physicians (ACCP)—have called for greater involvement from palliative care service providers in this setting,13–15 and studies describe how patients and caregivers suffer,3,16–18 but little is known about the impact of providing such services.
To provide effective palliative care services to this population, we require a better understanding of (1) effects on patient and family outcomes and (2) organizational challenges to service delivery. We designed a customized palliative care intervention aimed at meeting the needs previously identified by patients and caregivers living with advanced COPD19, 20 and evaluated outcomes within a feasibility framework.
Methods
Upon approval of the protocol by the Capital Health Research Ethics Board, we enrolled study participants in a single-centre, prospective, cohort observational study designed to determine the feasibility of (1) implementing customized home-based palliative care services to patients and caregivers living with advanced COPD and (2) measuring patient and caregiver outcomes associated with providing such services.
Patients attending ambulatory respirology clinics in Halifax, Nova Scotia, were referred to the study by their attending respirologist and were subsequently contacted by the study coordinator, who provided written information about the study and enrolled those who met the inclusion criteria. Subjects were eligible to participate if they resided within the geographic boundaries served by the Capital Health Palliative Care Program and had either moderate or severe COPD according to CTS criteria (Table 1). We excluded patients and/or caregivers with cognitive impairment or language barriers that precluded questionnaire completion, patients with estimated survival of less than six months, and those with prior palliative care service contact. The informal caregiver was identified by the patient as the individual most involved in helping to care for the patient at home. Patients who did not identify a primary caregiver or whose primary caregiver did not wish to participate were not excluded from the study. Our intervention consisted of two parts:
MRC, Medical Research Council.
Part a: Education on disease self management and end-of-life issues in COPD
We developed a modified format of the seven-module disease educational program Living Well with COPD used in a previous Canadian randomized controlled trial of self management. 22 We modified the program to include an eighth module developed by a member of our research team to provide additional education to patients and caregivers about end-of-life (EOL) issues, including information about mechanical ventilation similar to the decision aid described by Wilson and colleagues 23 (Table 2). The eighth module had undergone prior evaluation in a cohort of patients attending the Pulmonary Rehabilitation Program in Halifax. The modified education program was delivered in the patient's home by a respiratory therapist who had completed COPDTrec® and was certified as a COPD educator by the Canadian Network for Respiratory Care. Patients received a written COPD Action Plan as recommended by the CTS, 24 which provided detailed instructions for self initiating oral corticosteroids and antibiotics for those who were experiencing symptoms consistent with acute exacerbation of COPD (AECOPD).
Part b: Enrollment in Capital Health Integrated Palliative Care Program
After completion of the education program, patients were followed at home by the Capital Health Integrated Palliative Care Service for a period of four months. All subjects were initially seen together by a palliative care nurse case manager and consultant physician who completed a comprehensive individualized palliative care assessment and treatment plan which was forwarded in writing to the patient's primary care physician. The nurse case manager continued regular weekly follow-up by phone and coordinated delivery of additional home support services customized to individual need (Table 2). The nurse case manager made unscheduled follow-up visits if there was a need for reassessment based on a change in status. When required, follow-up physician home visits were coordinated through the nurse case manager and occurred either together or separately depending on the clinical situation. All patients were provided with contact information for the nurse case manager and for after hours support by the on-call palliative care physician.
All patients were reviewed at weekly multidisciplinary team rounds to facilitate coordinated care between the consultant and primary care members of the team.
Our aim was to determine the feasibility of implementing a program of research. 25 We estimated, based on projections from incomplete data from previous similar studies,22,26 that 10% to 30% of patients would provide incomplete data or die during the study intervention. Table 3 outlines the feasibility criteria developed to assess the practicality of our intervention and inform the sample size of future phases of research in this patient population.
Data collection and analysis
We collected baseline demographic data from patients and caregivers. For our secondary outcomes we used validated quantitative assessments to evaluate disease-specific health-related quality of life (The Chronic Respiratory Disease Questionnaire, CRQ 27 ); symptom prevalence and severity (The Edmonton Symptom Assessment Scale, ESAS 28 ); and satisfaction with care (CANHELP Questionnaire 29 ). Patients were asked to complete three questionnaires and caregivers two questionnaires at baseline, two months and four months after enrollment with the palliative care home team. In order to standardize their administration and maximize the completion rate, the research coordinator administered the questionnaires in each patient's home. We also asked patients and caregivers to rate the burden of completing the questionnaires on a scale of 0 to 10 (Table 3).
Using institutional databases, we tracked frequency of and reasons for emergency room visits and hospital admission during the intervention. We analyzed all deaths during and up to one year following completion of the study, noting the cause and location of death, presence or absence of documented established goals of care and do-not-resuscitate (DNR) order, and the incidence of provision of either CPR or intubation/ventilation. We compared place of death to stated preference for place of death at baseline.
Results
Between July 2007 and March 2010, 30 patients with advanced COPD and 18 informal caregivers were enrolled (Figure 1). Three patients (10%) were hospitalized and died prior to completion of the education program and were never evaluated by the palliative care home team. One patient died in hospital during the palliative care home team intervention after presenting to the emergency room with delirium secondary to respiratory failure. One patient dropped out after completing the education phase, choosing not to be seen by the palliative care team because of significant improvement in clinical status. A total of 25/30 patients (83%) and 14/18 caregivers (77%) were enrolled with the palliative care home team and completed the intervention to the four-month endpoint.
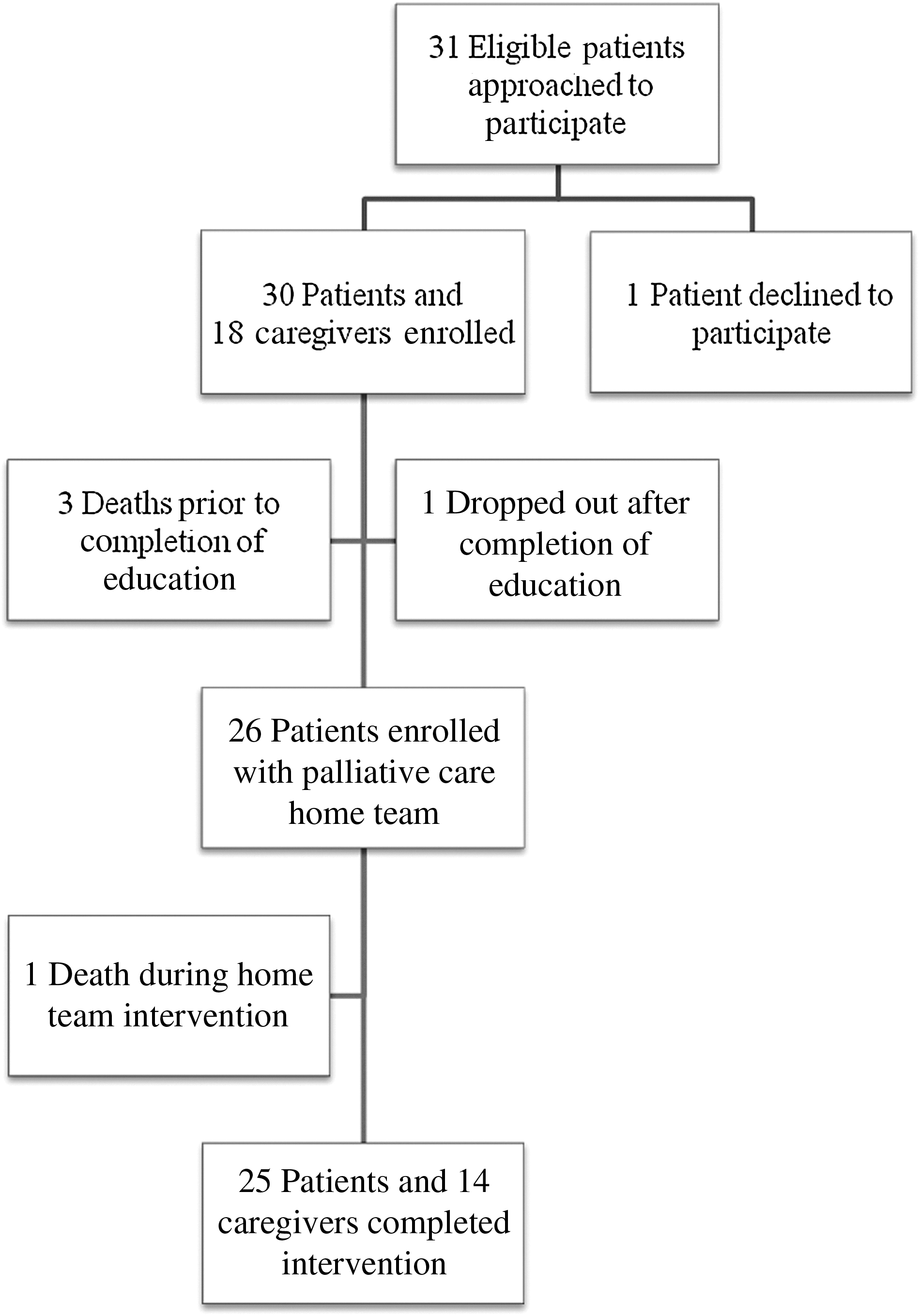
COPD IMACT Study patient flow diagram.
The majority of patients were male (53%), aged 70 years or over (60%), Caucasian (97%), and married (53%). Most had severe COPD with MRC (Medical Research Council) 5 dyspnea (60%) (Table 1) and were ex-smokers (80%), and half were on long-term home oxygen therapy. The remainder had moderate COPD with additional qualifying criteria for poor outcomes (Table 1). Most lived with a spouse (50%) or other family member (23%); the remainder lived alone. Among those who named an informal caregiver, a spouse was identified by 65%. All were either retired or unemployable due to disability from COPD, with a median reported household income of less than $20,000 CAN per year.
Outcomes
Overall we achieved two of our five original feasibility criteria (Table 3). Our most significant failings were an overestimate of both how quickly we would enroll patients and their capacity to complete multiple questionnaires. Less than 60% of patients were enrolled over the course of one year. The completion rate of questionnaires was 52% and 36% for patients and caregivers, respectively. For those who did complete multiple questionnaires, the average score for burden of completion was less than 1 (out of 10) by both patients and caregivers. The following summarizes the results of our secondary outcomes.
HRQoL and caregiver burden
There was no significant difference in HRQoL (n=13; change=0.31) or caregiver burden (n=5; change=0.65) from baseline to four months.
Symptom prevalence and severity
Dyspnea was the most prevalent and severe symptom, noted by all patients, with a mean severity score of 5.13/10 on the ESAS. Tiredness and decline in overall well-being were the next most common symptoms. Symptom severity remained unchanged over the course of the intervention.
EOL outcomes
Four patients (13%) died while participating in the study. All died in an acute care hospital ward setting due to complications of end-stage COPD. Twelve patients died within one year of completing the study, increasing overall mortality rate to 53%. Seven of 12 patients died from complications of COPD, and three due to comorbid illness. Two deaths occurred under unknown circumstances. Overall, 56% of the deaths occurred in an acute care setting. Of these, three patients died in a hospital-based palliative care unit, two died on a transitional care unit waiting for long-term care placement, and five patients died on an acute care hospital ward.
Three patients (10%) who completed the study continued to be followed by the palliative care team because of symptom instability and functional decline with anticipated short time prognosis. All three died of end-stage COPD and were admitted to a hospital palliative care unit in the last days because of caregiver exhaustion and inability to cope with symptoms of terminal dyspnea and delirium. None of the known circumstances of death during the study and in the year after study completion were associated with ICU admission, intubation/mechanical ventilation, or attempts at CPR. Seventeen of 30 patients specified a preferred location of death on baseline assessment; 12/17 (70%) identified home as the preferred location of death under ideal circumstances. None of the deaths occurred at home.
Health Care Utilization
There were 43 emergency room presentations in 15 patients (range 1–9); 29 (67%) of the presentations were directly related to COPD. Four patients (13%) accounted for 62% of presentations to the ER. There were 16 hospital admissions in 9 patients (range 1–7). Fourteen admissions (87.5%) were directly related to COPD. Two patients accounted for 62.5 % of the hospital admissions.
Patient and caregiver satisfaction
Eleven patients and five caregivers completed ratings of overall satisfaction with their care from 1 (very unsatisfied) to 5 (completely satisfied) at baseline and study completion (Table 4). Responses to open-ended questions outlined in Text Box are reflective of the opinions of the majority of patients and caregivers, and indicate that the involvement of the palliative care team was welcomed and valued by both.
Mean of responses (minimum 1, maximum 5).
Discussion
COPD IMPACT was our first attempt to provide a coordinated, customized palliative care intervention to patients with nonmalignant disease. Our feasibility results point to realities of evaluating related outcomes for patients with advanced COPD. Though nearly all of the eligible patients approached agreed to participate, only one third were enrolled within one year of study start-up. This reflected two realities: (1) patients with advanced disease often struggle to attend ambulatory clinics and (2) we had underestimated the personnel/resources required to meet our original projection of enrollment. Our feasibility outcomes will inform sample size calculations and realistic time frames, ensuring that future studies in this patient population are adequately powered to detect meaningful changes in outcomes that are of importance to both patients and their caregivers.
More than 80% of enrolled patients readily accepted home-based education and treatments and follow-up by the palliative care team. However, there were significant issues with respect to incomplete data collection, also found in a recent randomized control study involving 464 patients with COPD in Glasgow. 30 This further underscores the difficulties inherent in carrying out prospective studies in patients who are living with multiple burdens of advanced disease. Moreover, seeking improvement to traditional quantitative measures of symptom burden may miss subtle changes in outlook, hope, or confidence in dealing with a chronic illness, outcomes that lend themselves more to a qualitative approach. 31
The severity of illness of our patient cohort is reflected in the observation that within a year of study completion 53% of our patient participants had died (consistent with findings in an earlier Canadian multicentre study).20, 21 Although half of the deaths occurred in an acute care setting, none of the patients were intubated or were admitted to an ICU. All patients established comfort-focused care plans.
None of the deaths occurred at home despite the majority of patients having previously established comfort-based goals of care and the availability of local home-based expertise in palliative care. In contrast to caregivers of terminal cancer patients, family caregivers of COPD patients at the end of life are often physically and emotionally exhausted from years of stress and fatigue associated with care giving on the COPD rollercoaster.18,32 Even with the best available supports, dying at home from end-stage COPD may not be realistic or even the best option for many.
For those who survived, it became increasingly clear that housebound dyspneic patients had significant primary care/community-based needs, which could not be met when they lacked access to a primary care physician who would see them at home. Moreover, patients often relied on the emergency room to deal with any escalating symptoms or decreased capacity to cope.
There are a number of limitations to this study. First, standardization of the advanced care team intervention was an issue. As with all other patients enrolled in our home program, some patients were seen multiple times at home over the course of the intervention, while others who were stable required mainly phone support and coordination of services.We established a minimum set of core interventions while acknowledging that it isn't possible or desirable to standardize all aspects of palliative care involvement for an individual patient.
Second, selection bias may account for the forgoing of intubation and mechanical ventilation and admission to the ICU in all patients who died during and after the study intervention. However, patients and families made informed choices after our eighth EOL module and through further advance care planning discussions in the home as part of our palliative team involvement. Third, we did not include a control group, as a comparative analysis was not our intent. However the stability in HRQoL, caregiver burden, and symptom intensity over the course of the intervention may speak to its efficacy. Given the progressive course of advanced COPD, a similar population receiving usual care might experience deterioration in these outcomes over a four-month period, especially since more than half of the enrolled population died within one year of study completion. Finally, recruitment of inpatients may provide a richer source of potentially eligible study participants, making it more feasible to enroll the goal number of patients and caregivers with a one-year time frame.
There are a number of strengths to this study. Innovative approaches to palliation has been a research focus for our team for a number of years.5,33 We conducted the study in accordance with calls to incorporate quality indicators within a multidisciplinary approach. 34 In doing so, our palliative care program moved from its traditional focus on malignant disease, gaining valuable experience in providing care to a population faced with unique challenges and appreciation for the systematic changes required to better serve patients with chronic respiratory disease. Our study builds upon others on chronic illness26,35,36 by implementing a comprehensive home-based palliative care intervention specifically customized to address the needs of those living with advanced COPD. A novel aspect was the integration of chronic disease management strategies with education on disease prognosis/end-of life decision making along with concurrent proactive provision of comprehensive home-based multidisciplinary palliative care in a homogeneous population of patients with advanced COPD.
Insights gained through the conduct of this study have informed a new clinical service in which we identify inpatients with advanced COPD and high needs. We provide shorter, focused, and relevant education sessions according to need, supplemented by advance care planning sessions in the home. We use a mixed-methods evaluation approach and have seen a dramatic drop in ER visits and hospitalizations for our first 100 patients when comparing the years before and after enrollment. 37 Not all interventions based on self-management education have yielded positive outcomes.30,38 In addition, it isn't yet clear why such interventions fail when they do, or whether social determinants of health are more important than diagnostic considerations in some clinical settings.
Quantitative data collection remains challenging. In contrast, patients and families are quite willing to participate in qualitative interviews and record videos that provide insights into changes in HRQoL, symptom burden, satisfaction with care, and many other important patient-oriented outcomes.18,37 Those who live with advanced COPD where literacy rates are an issue consistently struggle to or don't want to complete written questionnaires. We need to learn how to most effectively assess these patient-centered issues and provide meaningful interventions without taxing an especially vulnerable population whose coping strategies are already stretched to the limit. 18
Conclusion
Providing home-based palliative care services for patients with advanced COPD is feasible, but completing repeated questionnaires is an impractical expectation for many patients and families. A careful assessment of barriers and limitations of current palliative care service models can provide important insights and opportunities for local program innovation and evaluation aimed at improving care for those living with advanced COPD.
Footnotes
Acknowledgments
We thank the patients and caregivers who were the reason we developed and implemented IMPACT, and our COPD educators and colleagues in spiritual care and palliative care who supported our participants over the course of the study intervention. The COPD IMPACT study was supported by an operating grant from the Canadian Institutes of Health Research (IHP-94532), and by the Canadian Researchers at End of Life New Emerging Team (CareNET). Dr. Sinuff was supported by a CIHR Clinician Scientist award.
Author Disclosure Statement
No competing financial interests exist.