
Abstract
Abstract
Delirium is highly prevalent in those with serious or advanced medical illnesses. It is associated with many adverse consequences, including significant patient, family, and health care provider distress. This article suggests a novel approach to delirium assessment and management and provides useful, practical guidance for clinicians based on a complete review of the existing literature and the expert clinical opinion of the authors and their colleagues, derived from over a decade of collective bedside experience. Comprehensive assessment includes careful description of observed symptoms, signs, and behaviors; and an understanding of the patient's situation, including primary diagnosis, associated comorbidities, functional status, and prognosis. The importance of incorporating goals of care for the patient and family is discussed. The concepts of potential reversibility versus irreversible delirium and delirium subtype are proffered, with a description of how diagnostic and management strategies follow from these concepts. Pharmacological interventions that provide rapid, effective, and safe relief are presented. Employing both pharmacological and nonpharmacological interventions, including patient and family education, improves symptoms and relieves patient and family distress, whether the delirium is reversible or irreversible, hyperactive or hypoactive. All interventions can be provided in any setting of care, including patients' homes.
Introduction
In brief review, delirium is an acute change in mental status that may fluctuate and has underlying physiological causes.8,9 It is frequently also called an acute confusional state, intensive care unit (ICU) psychosis, encephalopathy, acute brain failure, and syndrome of cerebral insufficiency. Using one term, delerium, minimizes confusion and ensures effective management.8–10
Delirium subtypes have been defined based on the presence (hyperactive) or absence (hypoactive) of psychomotor agitation, perceptual disturbances, and/or changes in level of consciousness. 11 Often both subtypes are present concurrently (mixed).12–20
Delirium is highly prevalent (56%–88%) in the elderly and those with serious or advanced medical illnesses.16,17,21–30 It is associated with many adverse consequences. Delirium often leads to unnecessary medical interventions, increased hospital admissions, prolonged hospitalizations,21,22,31,32 increased need for higher levels of care,24,27 functional decline, 33 increased mortality,9,16,28,29,32–39 decreased life expectancy,34,40,41 and increased health care utilization and costs.22,42,43 It can impair the recognition and control of other physical and psychological symptoms, such as pain and depression.44–46 Delirium frequently produces a significant amount of distress for patients, families, and caregivers.47–51
Most physiological disturbances can cause delirium.29,52–60 Even in the context of serious or advanced illness, these causes can frequently be determined and reversed.29,40,59,61 Some that are particularly frequent in this population, such as constipation and urinary retention, are easily addressed. The most common causes of delirium found in patients with serious and/or advanced illness are fluid and electrolyte imbalances; medications (benzodiazepines,52,53 opioids,29,53–55 steroids,53,54,56 and anticholinergics57,58); infections; hepatic or renal failure; hypoxia; and hematological disturbances.29,59
Once the diagnosis of delirium is made, the assessment of any associated symptoms, likely underlying cause(s), the patient's functional status and prognosis, and patient and family goals of care will help to determine whether the delirium is potentially reversible or irreversible.1,62,63 Pharmacological management differs based on potential reversibility; however, nonpharmacological interventions and family/caregiver education and support should be included in every delirium management plan.
Assessment
Evidence has shown that routine screening identifies patients at risk for delirium, who can then be assessed more thoroughly to establish a definitive diagnosis.1–4,42,60,64–66 Once delirium is suspected, a careful assessment by clinicians is necessary to identify patients with delirium, including:
• A careful description of the observed symptoms, signs, and behaviors (see Table 1), and changes over time • An understanding of the patient's situation, including primary diagnosis, associated comorbidities, functional status, and prognosis • The goals of care for the patient and family • The degree of associated family, caregiver, health care professional distress
A skilled diagnostician who can differentiate delirium from other related diagnoses is required to establish a definitive diagnosis of delirium 9 and categorize it as (1) hyperactive, hypoactive, or mixed; and as (2) potentially reversible or irreversible delirium.45,46 When one or more of these components is unclear, a physician specialist, with relevant expertise and experience, should be consulted to clarify the assessment.
Potential reversibility
To establish the potential reversibility of a delirium, it is important to know the patient's principal underlying diagnosis and comorbidities, prognosis, functional status, and goals of care.75,78–81 With appropriate diagnostic investigation and management, as consistent with patient and family goals of care, delirium may be reversible, even in the presence of serious or advanced illness.29,40,59,61 However at times, delirium can be classified as irreversible, and different management strategies ensue.
Irreversible delirium
Delirium becomes irreversible when
1) a time-limited diagnostic and adequate therapeutic trial to reverse the delirium ○ is inconsistent with patient and family goals of care, or ○ fails to discover underlying etiologies of the delirium, or ○ fails to reverse the delirium, even with the help of expert consultants, or 2) the underlying physiological processes are irreversible, e.g., end-stage organ failure; imminent death (prognosis of hours to days).
As noted by Freemon in 1981, most if not all patients who are exhibiting objective signs of the dying process67–69 (see Table 2) experience either a hyperactive (difficult road) or a hypoactive (usual road) delirium (see Figure 1).67,68 As dying is an irreversible process, the associated delirium is also irreversible and should be managed accordingly. The management for irreversible delirium focuses on symptom relief and supporting the family, caregivers, and health care professionals, all of whom are distressed. Consultation with an expert in delirium assessment and management before deeming a delirium irreversible should be considered.

Common paths to death: hyper- or hypoactive delirium. 137
Goals of care guide workup and management
Patients and families have a wide range of goals for their medical care and their lives.70–72 With serious, advanced, and/or life-threatening illness, some still hope for cure, many hope for prolongation of life, and almost all hope for concurrent relief of the multiple issues, physical and nonphysical, that cause them suffering. 73 At times they may have goals of care that appear to be overlapping and, at other times, conflicting. Patient and family goals are the core of patient-centered, whole person/family care.
Goals of care frequently change over time as an illness evolves and new information becomes available. Many patients approaching the end of their lives do not want aggressive or potentially life-prolonging medical therapies. They often prefer to focus on care that gives them the best possible quality of life and a good death, as they define these.
Patients or their surrogate decision makers (when the patient lacks decisional capacity) have the right to accept or refuse any medical treatment at any time. 70 A diagnosis of delirium often motivates patients living with advanced illnesses, their families, and their surrogate decision makers to reassess their goals of care. If a delirium is potentially reversible, patient and family goals of care, guided by thorough informed-consent regarding all options, should guide the diagnostic workup and management of the underlying causes.
Some patients and families will want time-limited therapeutic trials. They believe that simple tests, such as blood draws and urinalysis, are acceptable, especially if the results suggest an easy therapeutic intervention that could potentially reverse a delirium, reduce distress, and improve the patient's quality of life. They choose to attempt to reverse the underlying cause of a delirium and manage any associated distressing symptoms.
Others will decline a therapeutic trial, as is their right, and choose to forgo a diagnostic workup or any treatment of the underlying cause of the delirium, thus rendering it effectively irreversible. They may prefer to focus on managing distressing symptoms, relieving any ensuing suffering, and not attempting to reverse the underlying cause of the delirium, even when the workup or treatment are noninvasive and relatively easy to do (e.g., urinalysis and antibiotic treatment for a urinary tract infection). Adequate education about the situation and discussions about goals of care and informed consent are needed to ensure such decisions are not motivated by caregiver fatigue or other addressable concerns.
Management
Treating underlying cause
If the patient's underlying diagnoses, functional status, prognosis, and goals for care are consistent with a potentially reversible delirium, a time-limited and goal-focused diagnostic workup and therapeutic trial to reverse the underlying cause(s) is appropriate, as clearly stated by delirium treatment guidelines.1–4,10 Before ordering tests that are potentially invasive or burdensome to the patient, their potential benefits, risks, and burdens should be carefully considered. Only tests that will lead to specific management strategies should be ordered.
Safety
The safety for the patient, family, and caregivers should be insured, and any environmental issues addressed.9,10 The risks for suicidality, violence, falls, wandering, or inadvertent self-harm. The following steps can help to minimize these risks:
• removing or limiting access to dangerous items • increasing surveillance and supervision • padding bed rails • lowering beds as much as possible • placing mats on floor • reducing the number of invasive lines, including IV lines and Foley catheters • reducing movement-restricting devices • ensuring patient has access to reading glasses, hearing aides
Constant companions can also ameliorate many of these risks. 9
Management of symptoms
Whether attempting to reverse the delirium or not, the symptoms associated with a delirium should always be managed using nonpharmacological interventions,37,45,74–84 and when appropriate, with pharmacological interventions.1–4 All of the pharmacological and nonpharmacological strategies to manage delirium can be safely administered in any setting of care, including patients' homes.
Pharmacological interventions
Currently, there are
• no medications with U.S. Food and Drug Administration (FDA) approved indications for the management of delirium • no published double-blind, randomized, placebo-controlled trials to guide the pharmacological management of delirium • no consensus between oncologists, geriatricians, psychiatrists, and palliative medicine specialists about how to pharmacologically treat delirium
85
The following three management strategies comprise an evidenced-based, expert-consensus approach to the practical management of the symptoms associated with delirium, based on potential reversibility and delirium subtype (see Figure 2):
• potentially reversible, hyperactive delirium • irreversible, hyperactive delirium • hypoactive delirium, whether potentially reversible or irreversible
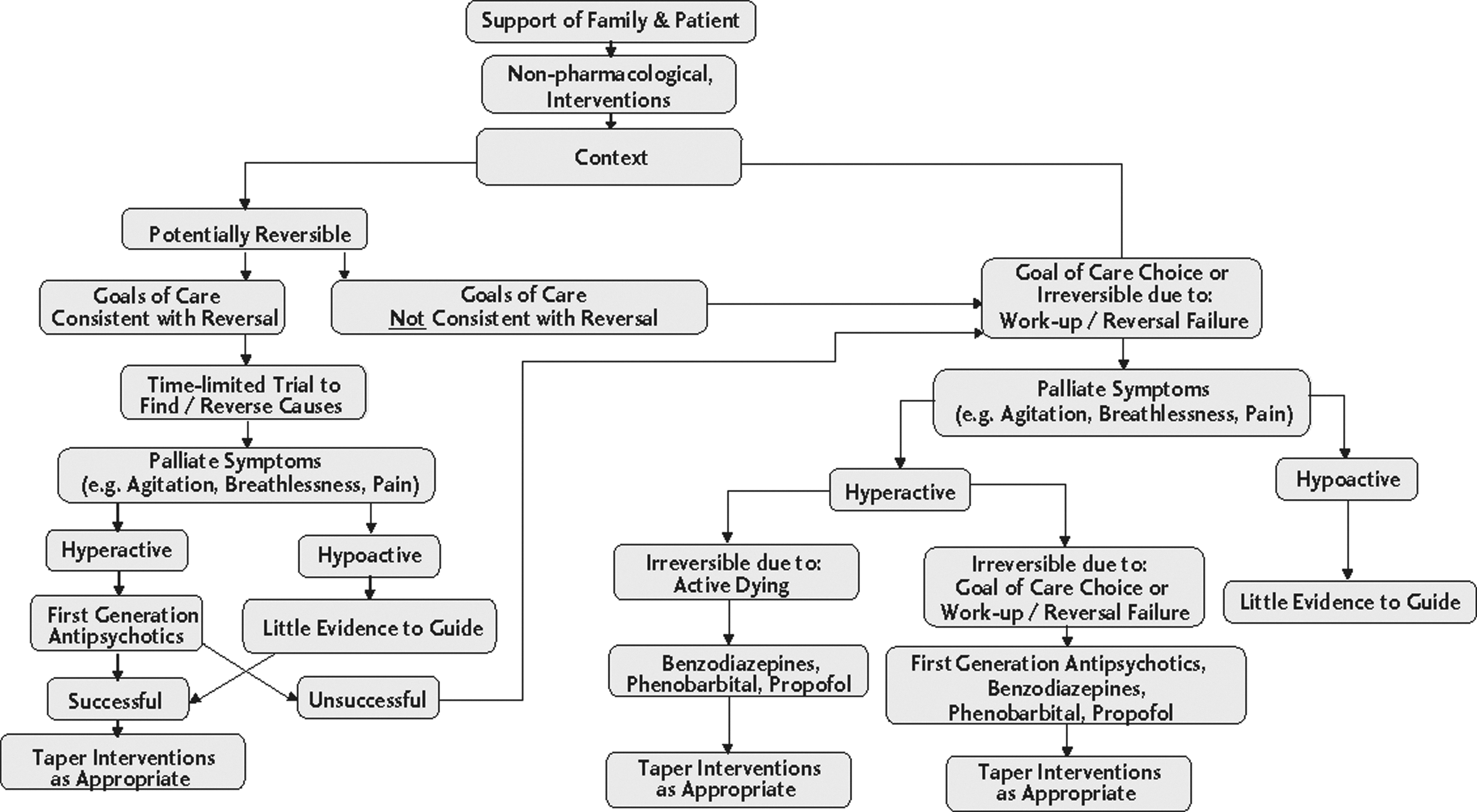
Delirium management decision tree.
Pharmacological principles
The medications used to control agitation or other symptoms associated with delirium follow first-order kinetics. Their biological effects are directly proportional to their plasma concentrations. These medications can be rapidly and safely using a technique based on each medication's pharmacokinetics, in the same manner that opioids are titrated rapidly and safely to control pain. 70
Titration technique
If the first dose of an appropriate medication does not control target symptoms by the time its plasma concentration is maximum (tCmax), that administration of the medication will not become effective with more time. Rapid and safe titration to control symptoms, can be achieved by dosing medications every tCmax until the symptom is controlled (don't dose sooner, don't wait longer). 70 Before each additional dose, ensure the patient does not have any undesired side effects. Titrate only to desired effect. If side effects emerge the dose can be reduce to the last most effective dose without side effects or a change in medications can be considered. Continuing to increase dosages without careful consideration of benefits and side effects may worsen the delirium.
Once the symptom (e.g., agitation) is controlled, the total dose used in the last 24 hours should be provided as a routine dose administered once every half-life (t½). To control any further breakthrough agitation or other symptoms, extra doses of the same medication once every tCmax as needed (PRN), at the same PRN dose that was previously effective, should be continued.
For example, to control agitation rapidly, antipsychotics can be safely dosed intravenously (IV) once every 15 minutes, subcutaneously (SC) once every 30 minutes, or orally (PO) once every 60 minutes until the agitation is controlled or the maximum recommended dose of the medication in a 24 hour period has been reached. 70 This is similar to the protocols used to rapidly control agitation with antipsychotics in emergency situations.86–90
Potentially reversible, hyperactive delirium
First-generation antipsychotics
For the first-line treatment of a potentially reversible, hyperactive delirium, evidence supports, and published guidelines recommend, the use of first-generation antipsychotics, e.g., haloperidol and chlorpromazine. (These guidelines do not distinguish potentially reversible from irreversible delirium, nor do they address the principal underlying diagnosis and comorbidities, prognosis, functional status, goals of care, or irreversible delirium.)9,10,91,92 Antipsychotics reduce agitation and address other symptoms associated with hyperactive deliria. Their sedative effects vary by medication. They are not amnestics, muscle relaxants, or antiepileptics, and do not have these therapeutic effects (see Table 3). Using the titration technique discussed above 70 the minimum antipsychotic dose needed to relieve distressing symptoms rapidly and safely can be established. The dose of an antipsychotic typically needed to control the symptoms of a hyperactive delirium is well below recommended maximum daily dosages.9–11,93,94 See Tables 4 and 5 for dosing guidelines and sample orders. If the symptoms are not controlled within a few hours, a physician specialist with expertise in delirium management can be consulted, when available.
Sedation is a side effect of opioids (not a therapeutic effect) and is not reliable from patient to patient or opioid to opioid.
✓=has property; ×=does not have property; -=has opposite property.
Management may be better with phenobarbital or propofol if symptoms are not controlled at the recommended maximum dose.
Infusion is reserved for severely agitated patients with dosage requirements exceeding injection volumes that can comfortably be given by routine intermittent IM or SC injection.
Time to onset.
Increases with prolonged administration due to tissue distribution.
IV, intravenously; PO, orally; PR, rectally; SC, subcutaneously; IM, intramuscularly.
Dosing schedule varies by routes of administration.
SC/IM dosing may be irritating to the skin.
IM, intramuscular; PO, orally; PR, rectally; SC, subcutaneously; EPS, extrapyramidal symptoms; PRN, as needed.
Second-generation antipsychotics
No evidence currently exists for improved efficacy with atypical (second or third generation) antipsychotics.52,95–97 These medications are often more expensive and have fewer routes of administration. 93 Existing treatment guidelines suggest starting with first-generation antipsychotics. 10
Antipsychotic side effects
When selecting any medication, the potential benefits, risks, and burdens of each medication should always be considered, as well as patient and family goals of care. Table 6 categorizes the common side effects for five antipsychotic medications used to control symptoms of delirium.9–11,93,94,98 As lower antipsychotic doses typically control the symptoms associated with deliria in seriously ill patients, evidence suggests that the risk of side effects appears to be less in this population.7,52,99 When higher doses are required to control symptoms, families are often willing to accept increased risks to control the severe distress experienced by the patient and themselves.
EPS, Extrapyramidal side effects; IV, intravenous; PO, orally; QTc, Corrected electrocardiogram QT interval; M1, muscarinic acetylcholine receptor; H1, histamine receptor; α1, α-1 adrenergic receptor; D2, dopamine receptor.
✓=relative strength of effect; ×=does not have effect.
The FDA has issued a black-box warning about the increased risk of death when first- or second-generation antipsychotics are used to treat
Benzodiazepines
With few exceptions (e.g., the management of alcohol withdrawal; acute agitation crisis), published guidelines recommend that benzodiazepines NOT be used as first-line treatment to manage potentially reversible deliria.9,10,91,92 As these are also sedatives and amnestics (see Table 3), they can make the delirium worse, increase the risk of falls, create memory problems, and lead to withdrawal syndromes.9,52,93
Opioids
Likewise, opioids have no role in the treatment of agitation or delirium. These are analgesics with no anti-agitation actions (see Table 3). Sedation is a side effect of opioids (not a therapeutic effect), and is not reliable from patient to patient or opioid to opioid. Care should be taken to differentiate pain-related behaviors from delirium-induced behaviors. New or increased doses of opioids may actually worsen delirium and the associated agitation, especially if no change in pain symptoms has occurred. Pain, in and of itself, does not cause delirium; though, uncontrolled pain may worsen the symptoms of delirium and complicate the clinical picture. When tapering opioids, the doses should be reduced carefully to avoid withdrawal syndromes.
Irreversible, hyperactive delirium
When irreversible, hyperactive delirium is diagnosed, antipsychotics could be used first-line; however, a shift to management with benzodiazepines may be more appropriate to control the symptoms associated with the delirium, especially when there are associated signs of the dying process (see Table 2).29,60,68,90,109–117 The concurrent use of antipsychotic medications targeted at perceptual disturbances or delusions may also be warranted.11,118
Delirium in dying patients
When patients are dying and experiencing an irreversible hyperactive delirium, there is significant risk of muscle tension; myoclonus; seizures; and distress for patient, family, and caregiver.67,68 When asked, most patients with serious or advancing illnesses confirm that they would rather not ‘experience’ the symptoms of a hyperactive delirium associated with dying or have any ‘memory’ of the event. Likewise, witnessing agitation, confusion, moaning, and groaning can cause significant distress in families, caregivers, and health care professionals.47–51 In dying patients with hyperactive delirium, when the goals are to decrease agitation, relieve muscle tension, ensure amnesia, and minimize the risk of seizures, benzodiazepines appear to be ideal medications to manage and prevent these symptoms.29,60,68,90,109–117,119
Benzodiazepines
These function as sedatives, anxiolytics, skeletal muscle relaxants, amnestics, and potent antiepileptics (Table 3). Using the titration technique 70 discussed above, the minimum benzodiazepine dose needed to rapidly and safely relieve symptoms can be established. (Sample orders are presented in Table 5). The dose of a benzodiazepine typically needed to control the symptoms of delirium is far below their median lethal dosages (LD50; see Table 4).93,110 If a paradoxical reaction occurs and the patient becomes more agitated, safe and rapid titration to higher doses will usually overcome the paradoxical reaction and palliate the symptoms. Target doses are still the minimum needed to effectively relieve distressing symptoms without any unwanted side effects.
The most common side effects of benzodiazepines are sedation, lethargy, ataxia, falls, weakness, nausea, impaired concentration and motor coordination, and anterograde amnesia. With prolonged use, there is also a risk of withdrawal seizures and physical and/or psychological dependence. In patients with irreversible, hyperactive delirium, the benefits of these medications are more likely to outweigh the risks. 93
To be clear, this is not palliative sedation. Sedation is not the primary goal, though it may be an outcome. The intent is to relieve agitation and other symptoms of delirium using the smallest dose of the best agent with the appropriate indications and desired effects. 119
While another common concern is iatrogenic hastening of death, there is no evidence that the appropriate use of benzodiazepines in patients with advanced illness hastens death. In fact, evidence suggests that appropriate use of benzodiazepines or antipsychotics may increase both quantity and quality of life.116,117,120–126
If benzodiazepines are ineffective, phenobarbital or propofol127,128 may be needed to control the symptoms associated with an irreversible hyperactive delirium. Their pharmacological parameters and suggested dosing are presented in Tables 4 and 5.127–129
Management of an acute agitation crisis
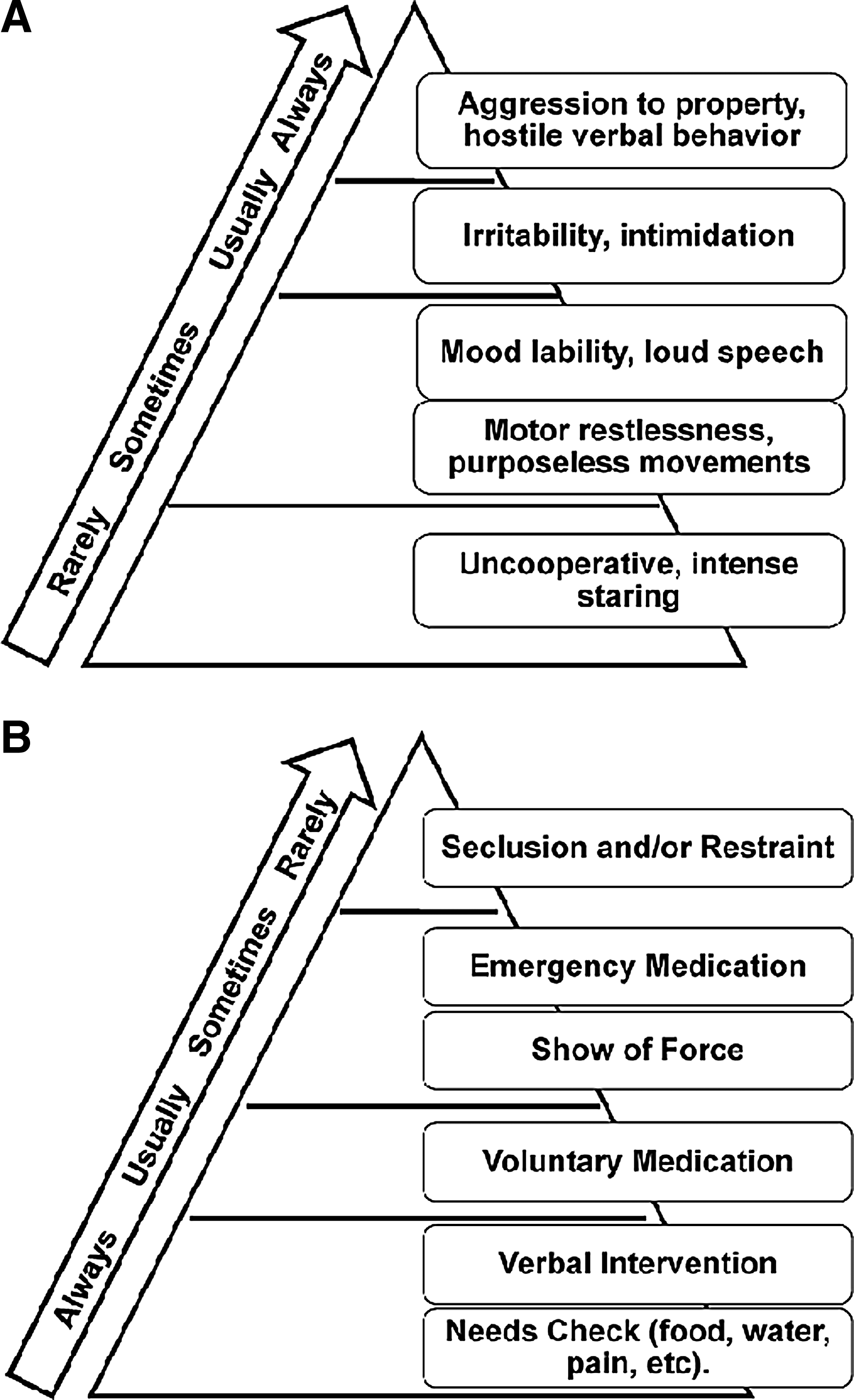
When imminent risk of harm exists for the patient or others due to agitation, the patient should be aggressively medicated to reduce the risk of harm to him or herself or others, then a plan for the best course of action can be formulated, especially when goals of care and/or potential reversibility are unknown. Figure 3 depicts the hierarchy of behaviors that constitute an emergency and the appropriate interventions to control them. 88 Table 5 contains medication recommendations and sample orders to use during an acute agitation crisis.88–90
Hypoactive delirium
Treatment of both potentially reversible and irreversible
No evidence exists to guide the use of benzodiazepines to manage an irreversible hypoactive delirium, though theoretically their broad spectrum of therapeutic actions (see Table 3) may be beneficial in the context of an irreversible hypoactive delirium.
Nonpharmacological approaches
All patients can benefit from nonpharmacological interventions, including several evidence-based environmental interventions, that will minimize the risk and severity of symptoms associated with delirium.1,37,45,74–78 These interventions can minimize disordered thinking, disorientation, sleep disturbances, immobility, risk of falls/injury, sensory deprivation, dehydration, and can address other environmental factors. Following are example of environmental interventions:
• Engage patients in mentally stimulating activities to help them with disordered thinking • Provide orienting and familiar materials to help patients know the time and date, where they are, and which staff are working with them • Ensure all individuals identify themselves each time they encounter the patient, even if the encounters are minutes apart • Minimize the number of people interacting with the patient and the quantity of stimulation the patient receives, e.g., television or loud music • Use family or volunteers as constant companions to help reassure and reorient a delirious patient. Encourage staff to sit with the patient while they do their documentation • Provide adequate soft lighting so patients can see without being overstimulated by bright lights. • Manage fall risks. • Provide warm milk, massage, warm blankets, and use relaxation tapes to optimize sleep hygiene and minimize sleep disturbances. • Ensure patients use their glasses, hearing aids, etc., to optimize orientation, decrease confusion, and promote better communication. • Ensure patients have good nutrition and an effective bowel and bladder management strategy. • Monitor fluid intake. Rehydrate with oral fluids containing salt, e.g., soups, sport drinks, red vegetable juices. When necessary, infuse fluids subcutaneously rather than intravenously.79–81
• Use physical restraints only as a last resort to temporarily ensure the safety of both staff and a severely agitated and not redirectable patient,37,82 and only until less restrictive interventions are possible. • Provide education and support to help family members cope with what they are witnessing.
83
Family and Caregiver Education and Support
Having a loved one experience delirium is extremely disturbing. It has been shown to produce a high level of distress in family and professional caregivers.49,51 In addition to general distress, caregivers of delirious patients have 12 times the risk for being diagnosed with a generalized anxiety disorder. 133 Supporting caregivers through education about delirium has been shown to help reduce these negative impacts. 83 Verbal and written education provides caregivers with a better understanding of delirium, feelings of empowerment, and an enhanced ability to make decisions on behalf of the delirious patient. 83
Family and caregiver education should be incorporated into the care plans of every delirious patient. Caregivers can be instrumental in helping to prevent, identify, and treat delirium. 134 If taught the signs and symptoms of delirium, caregivers may alert the medical team to the need for immediate follow-up. 83 Caregivers may also provide nonpharmacologic interventions for the prevention and treatment of delirium. 134 These caregiving acts will benefit the patient and provide the caregiver with an improved sense of control in the face of a potentially terrifying situation.
Conclusions
This article presents a cutting edge approach to delirium assessment and management. It provides useful, practical guidance for clinicians based on a complete review of the existing literature and expert clinical opinion.
Delirium is associated with many negative consequences, including significant distress for patients, families, and caregivers. Its assessment and management stand to be clarified and markedly improved.
With a careful history, physical examination, and investigation as appropriate, the causes of delirium are often discoverable and reversible, even in patients with serious and advanced illnesses. Diagnostic and management strategies differ based on potential reversibility and delirium subtype. The concepts of reversible versus irreversible delirium guide appropriate workup and management through determining and articulating (1) that a patient has a medical diagnosis of delirium; (2) the potential cause(s); (3) the primary diagnosis, associated comorbidities, functional status, and prognosis; and (4) the goals of care.
Once delirium is diagnosed and pharmacological interventions are deemed appropriate, medications are dosed with careful attention to their pharmacokinetics and safety parameters, using a ‘titration’ technique, to safely and rapidly relieve distressing symptoms. In all cases, nonpharmacological interventions are used to treat and prevent the symptoms associated with delirium. Education and support is provided to the patient, family, caregivers, and health care professionals to minimize their distress.
With these combined approaches, clinicians can rapidly control the agitation and other symptoms associated with delirium and relieve patient and family distress, whether the delirium is reversible or irreversible, hyperactive or hypoactive, even in seemingly refractory, seriously ill, or actively dying patients. Most people want to be cared for and die at home;135,136 fortunately, all of these interventions can be used in any setting of care, including patients' homes.
Footnotes
Acknowledgments
The authors wish to acknowledge the support from the faculty, staff, and patients and families at San Diego Hospice and The Institute for Palliative Medicine. This work was supported by the John A. Hartford Center of Excellence in Geriatric Psychiatry at the University of California, San Diego; The National Institute of Mental Health K23MH091176; a National Palliative Care Research Center Career Development Grant ; and by donations from the generous benefactors of the education and research programs at San Diego Hospice and The Institute for Palliative Medicine.