
Abstract
Abstract
Background:
Current evidence indicates that patients with hematological malignancies are less likely to receive input from specialist palliative care services compared to those with solid tumors.
Aim:
We aimed to analyze data for referrals to our palliative care service, in order to assess trends in the number and proportion of referrals received from hematology, and changes in the characteristics of these referrals.
Design:
Prospective information was collected for all referrals to the Department of Pain and Palliative Care (DPPC) over a four-year period. This included inpatient/outpatient status, diagnosis, symptoms, and goals of the referring clinician; and information linked to hospital inpatient data to obtain date and location of death.
Settings/Participants:
All hematology referrals were from January 2007 to December 2010.
Results:
Hematology referrals constituted 11.6% of all referrals received during the study period. Outpatient referrals increased significantly with each year, as did the proportion of patients referred for symptom control. The median time from referral to death was 34 days, with poorest survival seen in acute leukemia and inpatients. Overall, 54% of inpatient hematology deaths had consultation from the DPPC, with these patients less likely to die in the intensive care unit.
Conclusions:
Over recent years, collaboration between hematology and palliative care has resulted in increased referral numbers, with potentially positive results for patients.
Introduction
The Peter MacCallum Cancer Centre is a publicly funded dedicated comprehensive cancer centre accepting referrals from across Australia. The Department of Pain and Palliative Care (DPPC) is a well-established inpatient and outpatient consultative service. Our clinical impression is of increasing numbers of hematology referrals and greater palliative care involvement in hematology deaths. We aimed to analyze recent trends in the number and proportion of hematology referrals made to DPPC, as well as to assess for changes to the characteristics of the referrals and the nature of palliative care involvement.
Methods
Data collection
DPPC doctors and nurse consultants routinely collect prospective data from all referrals using a standardized form. Data items include demographic details, referral date and location, referring unit, diagnosis, care goals, Edmonton Symptom Assessment Scale (ESAS), 10 Palliative Prognostic Score (PaP), 11 and Edmonton Classification System for Cancer Pain (ECS-CP). 12 A data manager enters information into a Microsoft Access™ database.
Data were extracted for all referrals received from the hematology unit, with analysis performed for patients whose principal diagnosis was a hematological malignancy referred from January 1, 2007 to December 31, 2010. Information on all inpatient hematology deaths (including those not referred to DPPC) was obtained from the hospital patient administration system and was anonymously linked to the referral dataset.
Statistics
Summary statistics were produced using standard methods. Trends in proportions over time were analyzed using the Cuzick χ2 test for trend to compare number exposed by calendar year. For survival analyses, multivariate Cox regression was used to examine survival from time of referral to death, with exposure variables of age; diagnosis group (acute leukemia, lymphoma, multiple myeloma, and other); and inpatient/outpatient status. For comparison to other publications, median time to death was reported for those known to have died. The effect of palliative care involvement on the outcome of death in the intensive care unit (ICU) was analyzed using the Fisher's exact test. P values are unadjusted for multiple comparisons and are considered significant at <0.05. Statistics were computed using Stata statistical software version 12.0 (StataCorp., College Station, TX).
Results
Hematological malignancies constituted 11.6% of all 2377 referrals DPPC received during the study period, while the commonest solid tumor referrals were gastroenterological (17.9%) and lung cancer (17.4%). DPPC received 279 referrals from the hematology unit, of which 276 related to hematological malignancies. Demographic characteristics by calendar year of referral are presented in Table 1. Outpatient referrals constituted an increasing proportion of referrals by year. Similarly, hematology referrals increased as a percentage of all referrals from 9.7% to 13.7% (see Figure 1).
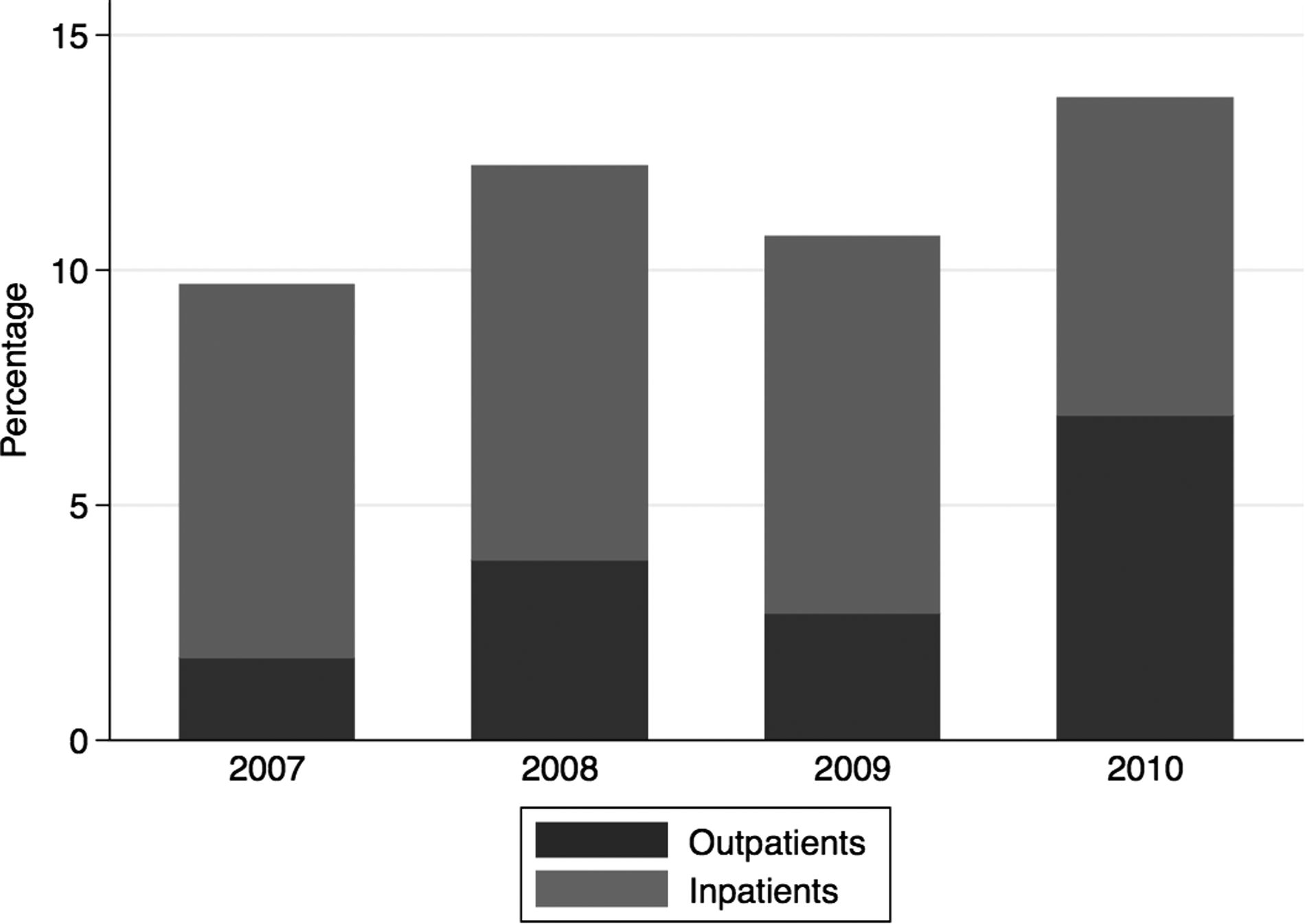
Percentage of total palliative care referrals received from hematology, by year and inpatient/outpatient source.
p values for χ2 test for trend by year.
Lymphoma including Hodgkin's disease.
n refers to number of patients for whom field was complete.
CLL, chronic lymphocytic leukemia; IQR, interquartile range; SD, standard deviation.
Diagnoses were acute leukemia (49), chronic lymphocytic leukemias (22), lymphoma (94), multiple myeloma (65), myeloproliferative disorders (33), and miscellaneous (13). Over the study period a significantly greater proportion of patients were referred for multiple myeloma, while lymphoma remained the commonest referral diagnosis throughout. The principal goals of the referring clinician were most frequently advice on symptom control or palliative management (with the latter suggesting decreased focus on disease-directed therapy). Of those for whom an ESAS score was recorded (149), 80.5% reported any pain, with a median pain score of 5 (interquartile range [IQR] 2–8). Similarly, for those with available data, the commonest symptoms reported were tiredness and loss of appetite (see Table 1).
Around one quarter (25.7%) of patients referred to palliative care died within 28 days of referral. Of those known to have died, median duration from referral to death was 34 days (IQR 9–144). Time to death was longer for outpatients (61 [IQR 18–164] days) than for inpatients (31 [IQR 8–144] days). Multivariate analysis revealed that age and diagnosis significantly influenced survival from point of referral, with increasing age predicting poorer survival (hazard ratio [HR] per decade 1.20 [1.09–1.33], p<0.001) and a trend toward poorer prognosis for inpatients (HR 1.40 [0.98–1.99], p=0.064). By comparison to the reference diagnosis of lymphoma, acute leukemia conferred the poorest prognosis (HR 1.73 [1.15–2.62], p=0.009); survival for other diagnoses was similar (HR 1.03 [0.69–1.53] p=0.89); and multiple myeloma was associated with improved survival (HR 0.58 [0.35–0.94], p=0.028) (see Figure 2).
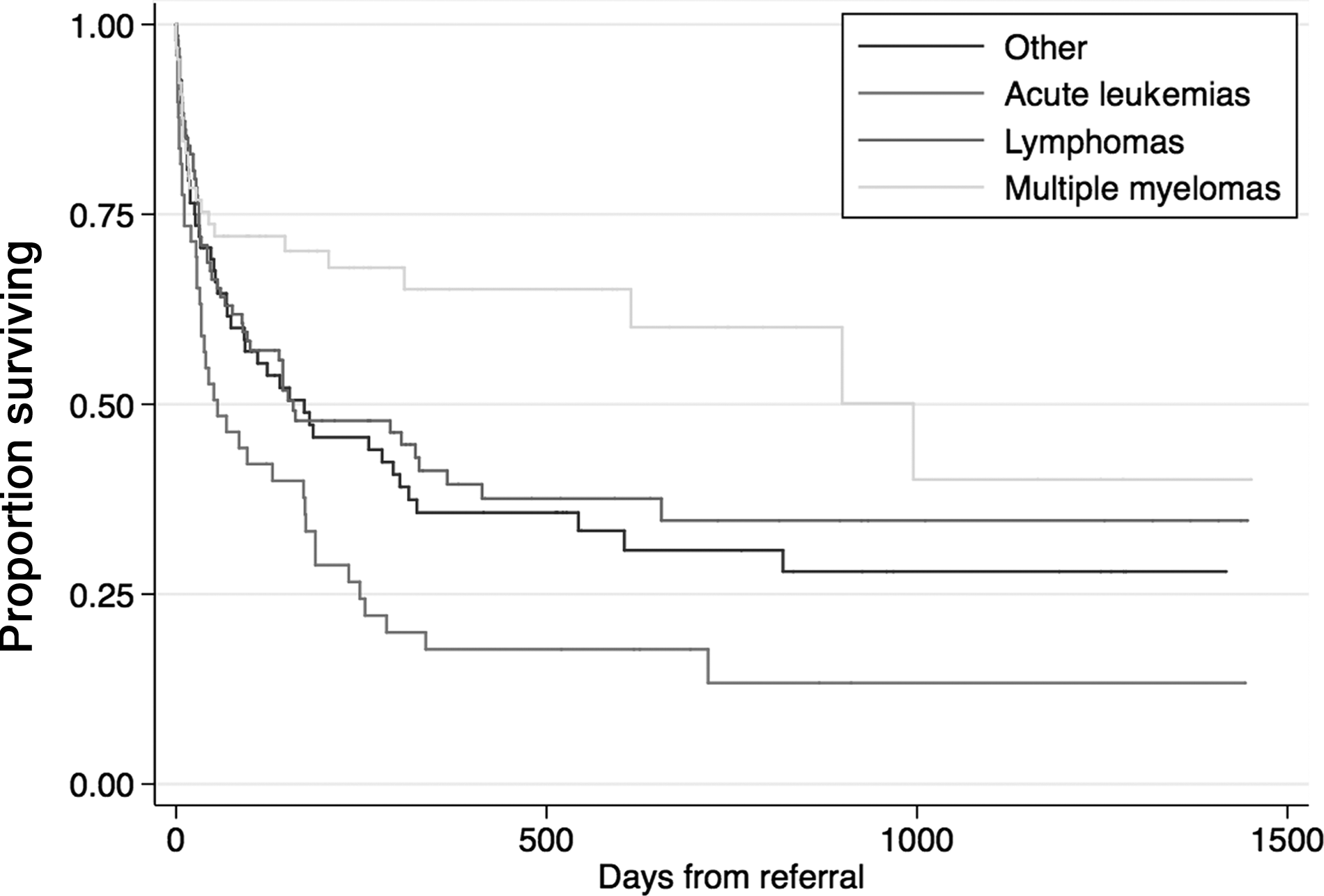
Patient survival from date of referral by diagnosis and referral source.
After linkage to death data, the proportion of hematology inpatient deaths referred to DPPC was 54.0% overall and increased by calendar year (see Table 2). Patients dying in hospital who had been referred to palliative care were significantly less likely to have died in ICU (7/68, 10.3%) than those who had not been previously referred (29/58, 50.0%, p<0.001, Fisher's exact test).
Discussion
In this prospective observational cohort study we confirmed our suspicion that the proportion of hematology referrals received by DPPC increased over recent years, with hematology now constituting the third commonest referral source. As a standardized data collection tool had been established, with collected data discussed at weekly unit meetings to verify accuracy, we believe this study gives an accurate picture of trends in hematology referrals at our tertiary centre.
Preliminary national audit data from January to June 2011 show the proportion of hematology referrals to DPPC increasing further to 16.8% at our centre. This is considerably higher than the Australian estimate of 5.3% for the same period, 13 with acute leukemia and non-Hodgkin's lymphoma referred less often than colorectal tumors, despite similar symptom burdens. 14 Internationally, patients with hematological malignancy have lower referral rates than other malignancies, although the proportion varies. 15 Our data do not enable us to estimate the proportion of all patients with hematological malignancy receiving DPPC input. However the increase in hematology referrals along with the increasing proportion of hematology deaths referred to DPPC suggest increasing involvement of our service.
The increase in hematology referrals was principally due to the increase in outpatient referrals, which rose from less than 20% in 2007 to more than 50% in 2010. This suggests earlier contact with DPPC and is supported by our observation of slightly longer survival from point of referral among outpatients and the increasing frequency of referrals for symptom control. Early involvement of palliative care is beneficial, as hematology patients have similar symptom burdens to those with solid tumors, with greater rates of delirium and drowsiness.16,17 Early palliative care involvement is important in facilitating trusting therapeutic relationships and establishing appropriate goals of care. 18 Therefore, our service has worked with hematology to increase DPPC presence in outpatient clinics and awareness of its service. This reflects a commitment by both services to work towards a shared-care model, in which patients may continue their disease-directed therapy concurrent with palliative care consultation.
Our finding of 54% of all hematology deaths having been previously referred to DPPC is considerably higher than other published data, with rates ranging from 14% in the United States to 25% in the United Kingdom.19,20 Moreover, the increasing proportion of hematology deaths with prior DPPC input observed suggests that the increase in referrals was not due to an increase in hematology workload relative to other streams.
Our median survival of 34 days is longer than that of other centres (14 days, MD Anderson Cancer Centre), with our survival approaching estimates for solid tumors (47 days). 21 Hematological disorders are highly heterogeneous, with particularly marked prognostic differences for myeloma and acute leukemia. Our estimates of survival grouped all hematological malignancies, including genetic subtypes, into four categories, inevitably creating diagnostic groups that include biologically different diseases. 22 This creates particular challenges for prognostication, symptom control, and formulation of appropriate referral pathways.
Difficulties in referring patients with hematological malignancies to palliative care include lack of access, lack of experience of palliative care units, the challenge of continuing disease-directed therapy while incorporating a palliative approach, and difficulties in determining and communicating prognosis. However, surveys of clinicians have identified a willingness to refer such patients and engage more actively with palliative care. 23 In order to improve collaboration with hematology, palliative care services must also be proactive and flexible. 24
The impact of palliative care services among patients was reflected in the fivefold lower proportion of inpatient deaths occurring in ICU that had been previously referred to palliative care. Although causation cannot be inferred, implementation of palliative care services has led elsewhere to a reduction in the proportion of inpatient deaths occurring in ICU. 25 While other studies report greater overall proportions of patients dying in ICU, the magnitude of difference due to palliative care involvement is similar. 16
The limitations of our study include that our results, obtained at a comprehensive cancer centre, may not be externally generalizable. Our finding of increasing DPPC involvement with hematology patients cannot be confirmed without assessing the total hematology clinical workload. Death data are probably incomplete, as some patients died at home or in an external hospice. Although increased time from referral to death was demonstrated, we cannot confirm that this necessarily improves outcomes.
In conclusion, we present evidence that patients with hematological malignancies are increasingly referred to palliative care services at our centre. Patients referred were a diverse group, with a high symptom burden and disparate prognoses and care needs. Close ties between our service and hematology appear to have resulted in earlier referral, with more time to address complex issues. The association between palliative care involvement and death outside ICU is also consistent with a positive influence on management.
Footnotes
Author Disclosure Statement
The authors declare no conflict of interest.