
Abstract
Abstract
Background:
Standardized approaches for assessing and classifying cancer pain are required to improve treatment of patients with complex pain profiles. The Edmonton Classification System for Cancer Pain (ECS-CP) offers a starting point for the evolution of a standardized international classification system for cancer pain and was introduced into multisite research initiatives of the European Palliative Care Research Collaborative (EPCRC).
Objectives:
The primary purpose of this study was to describe the prevalence of the five ECS-CP pain classification features: pain mechanism, incident pain, psychological distress, addictive behavior, and cognition—in a diverse international sample of patients with advanced cancer.
Methods:
A total of 1070 adult patients with advanced cancer were recruited from 17 sites in Norway, the United Kingdom, Austria, Germany, Switzerland, Italy, Canada, and Australia; 1051 of 1070 patients were evaluable. A clinician completed the ECS-CP for each enrolled patient. Additional information, including pain intensity, were also collected through patient self-reports, using touch-sensitive computers.
Results:
Of 1051 evaluable patients, 670 (64%) were assessed by a clinician as having cancer pain: nociceptive pain (n=534; 79.7%); neuropathic pain (n=113; 16.9%); incident pain (n=408; 60.9%); psychological distress (n=212; 31.6%); addictive behavior (n=30; 4.5%); normal cognition (n=616; 91.9%). The prevalence of ECS-CP features and pain intensity scores (11-item scale; 0=none, 10=worst; rated as now) varied substantially across sites and locations of care.
Conclusion:
The ECS-CP is a clinically relevant systematic framework, which is able to detect differences in salient pain classification features across diverse settings and countries. Further validation studies need to be conducted in varied advanced cancer and palliative care settings to advance the development of the ECS-CP toward an internationally recognized pain classification system.
Introduction
Over the past 23 years, a research program to develop a universally accepted pain classification tool has accrued a significant progression of work, resulting in the development of the Edmonton Classification System for Cancer Pain (ECS-CP). The ECS-CP includes five features: pain mechanism, incident pain, psychological distress, addictive behavior, and cognitive function. 5 Although pain intensity is not presently included as a core feature of the ECS-CP, moderate and severe pain intensity at initial assessment have been identified as significant predictors of increased time required to achieve stable pain control, and associated with higher opioid dose requirements and more adjuvant approaches.5,6
This program of work was merged with the aims of the European Palliative Care Research Collaborative (EPCRC), which similarly recognized the need to develop a unified pain classification system for patients with advanced cancer based on ongoing research and international consensus. 7 A pivotal issue was whether to proceed with the ECS-CP as a foundation or to develop a new consensus tool. There was agreement that the ECS-CP offered the best starting point for evolution of an international classification system for cancer pain 8 and this was introduced into multisite research initiatives of the EPCRC.
The primary purpose of this study was to describe the prevalence of ECS-CP pain classification features in a diverse international sample of advanced cancer patients. We hypothesized that frequencies of pain classification features would vary across sites and locations of care, with more acute palliative care settings having more complex pain features than less acute settings. A secondary objective was to demonstrate the variability in pain intensity at initial presentation in diverse palliative care settings.
Methods
Study design
We analyzed data from an international study in patients with advanced cancer who were recruited from palliative care inpatient and outpatient units, hospices, and general oncology and medical wards. A total of 17 centers within Norway, the United Kingdom, Austria, Germany, Switzerland, Italy, Canada, and Australia participated in this multicenter cross-sectional study, using a computer-based symptom assessment program. The study was conducted between October 2008, and December 2009. The findings from the initial analysis have been published elsewhere. 9 In this article, we report the findings of our analysis of pain classification features and pain intensity.
Sample
Inclusion criteria were patients with incurable metastatic cancer or locally advanced disease, 18 years old or above, who were able and willing to provide written informed consent. The exclusion criteria were inability to complete the assessment because of physical or obvious cognitive impairment or language problems.
Pain classification system
The ECS-CP consists of five pain features: mechanism of pain, incident pain, psychological distress, addictive behavior, and cognitive function. 5 It is a clinician-rated assessment, based on an integration of clinical findings including but not limited to the patient history, patient reports, physical examination, medical record, objective assessments, available diagnostic imaging and collateral history. The ECS-CP uses a categorical rating system, in which clinicians assess the presence or absence of a feature. Clinicians can select an “unknown” category, if there is insufficient information to categorize the feature at the time of the initial assessment. Subsequent assessments may be conducted if the patient's condition changes and/or as additional information is obtained. For the purposes of this study, a clinician conducted a single assessment using the ECS-CP, guided by written administration guidelines. 10
Data collection
Data collection was performed by touch-sensitive computers, consisting of two sets of questionnaires, completed by clinicians and patients, in random order. Details on the language compatibility lay-outs (English, German, Italian, Norwegian) and specifications have been presented previously.9,11
The clinician section included the ECS-CP, Karnofsky Performance Status (KPS), 12 and Mini-Mental State Examination (MMSE). 13 The patient section consisted of 71 initial questions focusing on symptoms and quality of life, which all patients completed. There were two different items for patient reports of pain “right now”: (1) pain rating (0–10) using the Edmonton Symptom Assessment System 14 and (2) a specific pain question ”Please rate your pain by marking the one number that best describes your pain right now” (0–10 response). For the purposes of this analysis, the latter question was used to measure pain intensity now.
Patients completed their questionnaires with the assistance of a research nurse or assistant. The clinicians who conducted the assessments were not blinded to the patient assessments. Questions that were not taken from existing questionnaires in the four languages were subject to forward–backward translations according to established procedures. 15
Data analysis
We analyzed the data based on the clinician's assessment of cancer pain using the ECS-CP. We used descriptive statistics (frequencies, means, medians, and standard deviations) to determine the prevalence of ECS-CP pain classification features and pain intensity in the total sample, and across sites and locations of care. Box plots were used to compare pain intensity rates across sites and locations of care. Box plots provide a visual representation of distributions by summarizing the median (bold line in box), quartiles (box), 95% interval (whiskers), and extreme values (highest and lowest). Pain intensity rates were further collapsed into three categories—mild (0–3), moderate (4–6), and severe (7–10)—based on previous studies5,17; and then compared across sites. We included a range from 0 to 3 for the mild category, because some patients whose pain is well managed might report a pain score of zero. 16
Ethical considerations
The study was performed according to the rules of the Helsinki Declaration. Prior to study initiation, appropriate ethical approval was obtained at each participating site within each county.
Results
Participant characteristics
A total of 1051 of 1070 cases were eligible for analysis. Nineteen cases were ineligible due to patient withdrawal of consent (n=4) and technical failure (n=15). Of the 1051 evaluable patients, 1034 had a completed ECS-CP, with 670 (670/1051; 64%) assessed by a clinician as having cancer pain. Table 1 provides a detailed summary of participant characteristics. Most patients with cancer pain were older than 60 years and cognitively intact, with variable performance status. A frequency distribution, comparing data collection centers by location of care, appears in Table 2.
SD, standard deviation; KPS, Karnofsky Performance Status; MMSE, Mini-Mental State Examination.
Of the remaining participants who were either not assessed as having cancer pain (n=364) or did not have a completed ECS-CP (n=17), most (n=226; 62%) rated their worst pain in 24 hours as zero. A small proportion of participants rated their pain as 1 or greater for current pain (n=67; 18%), worst pain in 24 hours (n=123; 34%), and average pain in 24 hours (n=113; 31%).
Prevalence of ECS-CP features
The ECS-CP features across all sites were: nociceptive pain (n=534; 79.7%); neuropathic pain (n=113; 16.9%); Incident pain (n=408; 60.9%); psychological distress (n=212; 31.6%); addictive behavior (n=30; 4.5%); normal cognition (n=616; 91.9%; Table 3). As shown in Table 3, there were substantive differences in ECS-CP features across the 17 sites. The most consistent scores (i.e., smallest range) across sites were for normal cognition (64%–100%). In contrast, the greatest range of scores across sites was for incident pain, with the lowest frequency of 9% at one site and the highest frequency of 81% at another site. The range of scores for neuropathic pain also varied substantially across sites, ranging from 0% to 64%. This variability in pain mechanism is further illustrated in Figure 1. As shown in this figure, the relative frequencies (%) among nociceptive (Nc), neuropathic (Ne), and unclassified pain (Nx) varied across locations of care, with the prevalence of neuropathic pain being lowest in home care (9%) and highest in hospice or nursing home (33.3%). The overall prevalence of neuropathic pain for hospital palliative care units was 19.6%.
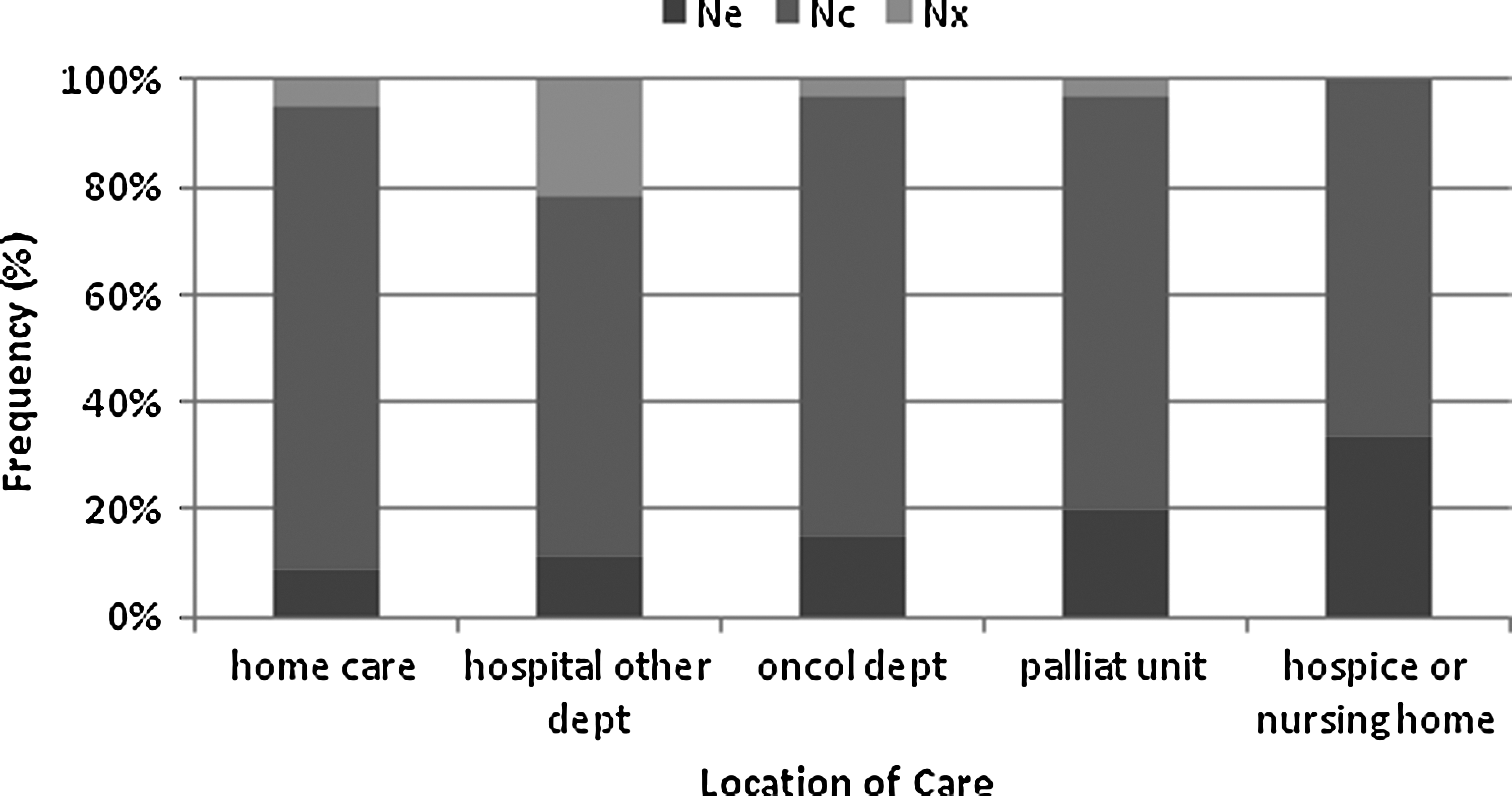
Frequency distribution (%) of pain mechanism by location of care (n=670). (Ne, neuropathic pain syndrome with or without any combination of nociceptive pain; NC, any nociceptive combination of visceral and/or bone or soft tissue pain; Nx, insufficient information to classify.)
Represents range in frequencies across the 17 sites.
Nc, any nociceptive combination of visceral and/or bone or soft tissue pain; Ne, neuropathic pain syndrome with or without any combination of nociceptive pain;
Ii, incident pain present; Pp, psychological distress present; Aa, addictive behavior present; Co, no impairment. Patient able to provide accurate present and past pain history unimpaired.
Pain intensity
Figures 2 and 3 illustrate the variability of pain intensity scores (rated as now) across sites and locations of care, respectively, using box plots. For Figure 2, median pain intensity scores ranged from 1 (Bergen, Norway; London, UK; Ullevål, Norway; Skien, Norway) to 5 (Edmonton Tertiary Palliative Care Unit, Canada). The 95% interval varied for each site, with the smallest interval for Curtin, Australia (0–3) and the largest interval for Milan, Italy (0–10). Figure 3 illustrates the variability in pain intensity across locations of care, with the hospital palliative unit having the highest median (median=3) and greatest variability (range, 0–10). Most patients (n=401; 69.9%) rated their current pain intensity between 0 and 3 (see Table 4). Depending on the site, the frequency of pain ratings between 0 and 3 ranged from 33% to 100%. A similar pattern of variability across sites was noted for moderate (4–6) and severe (7–10) pain ratings, with ranges of 0% to 67% (moderate) and 0% to 56% (severe).
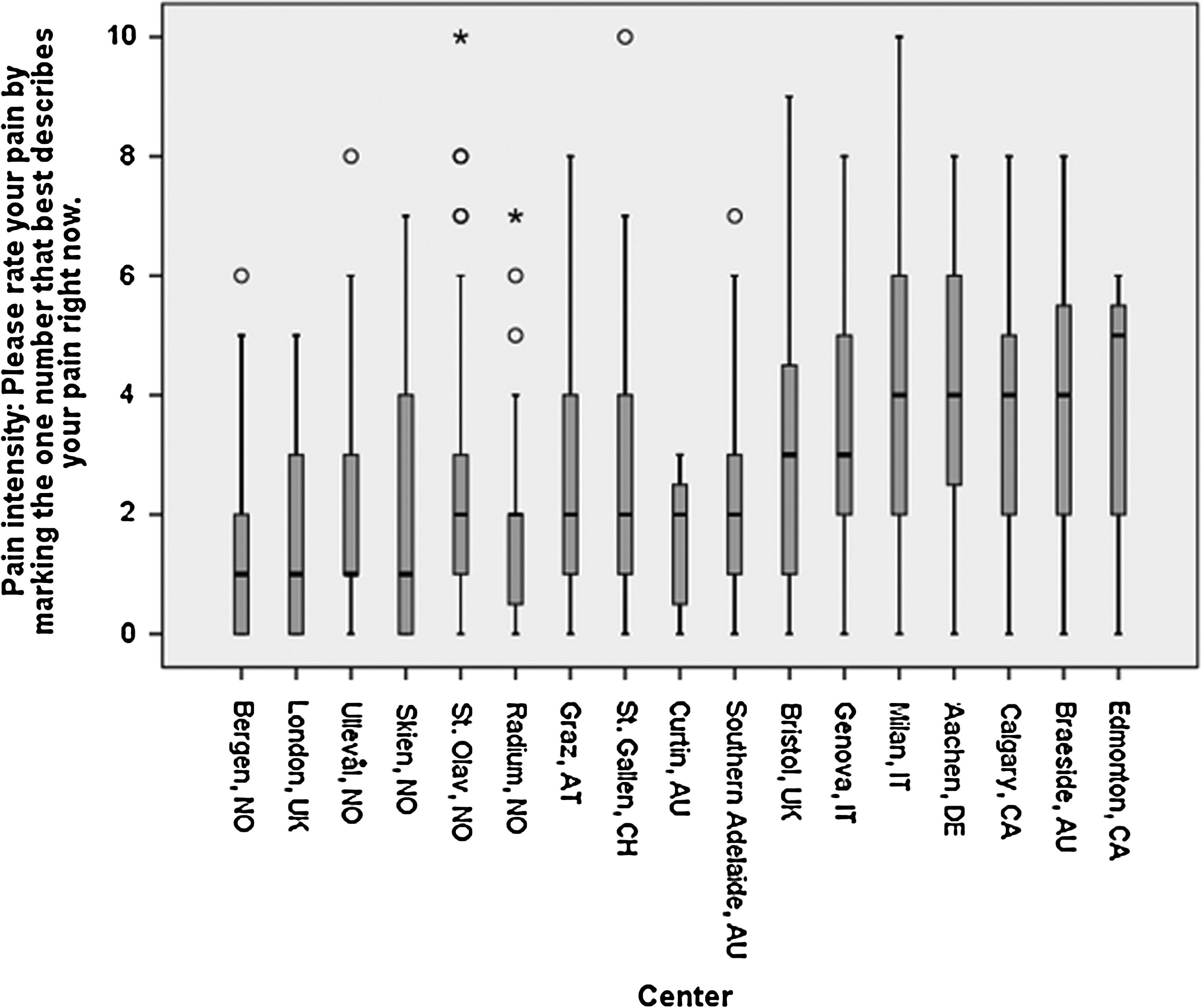
Box plots of pain intensity (rated right now) by collaborating site (n=570). (Note: Total does not add upto 670 due to missing data [n=96].)
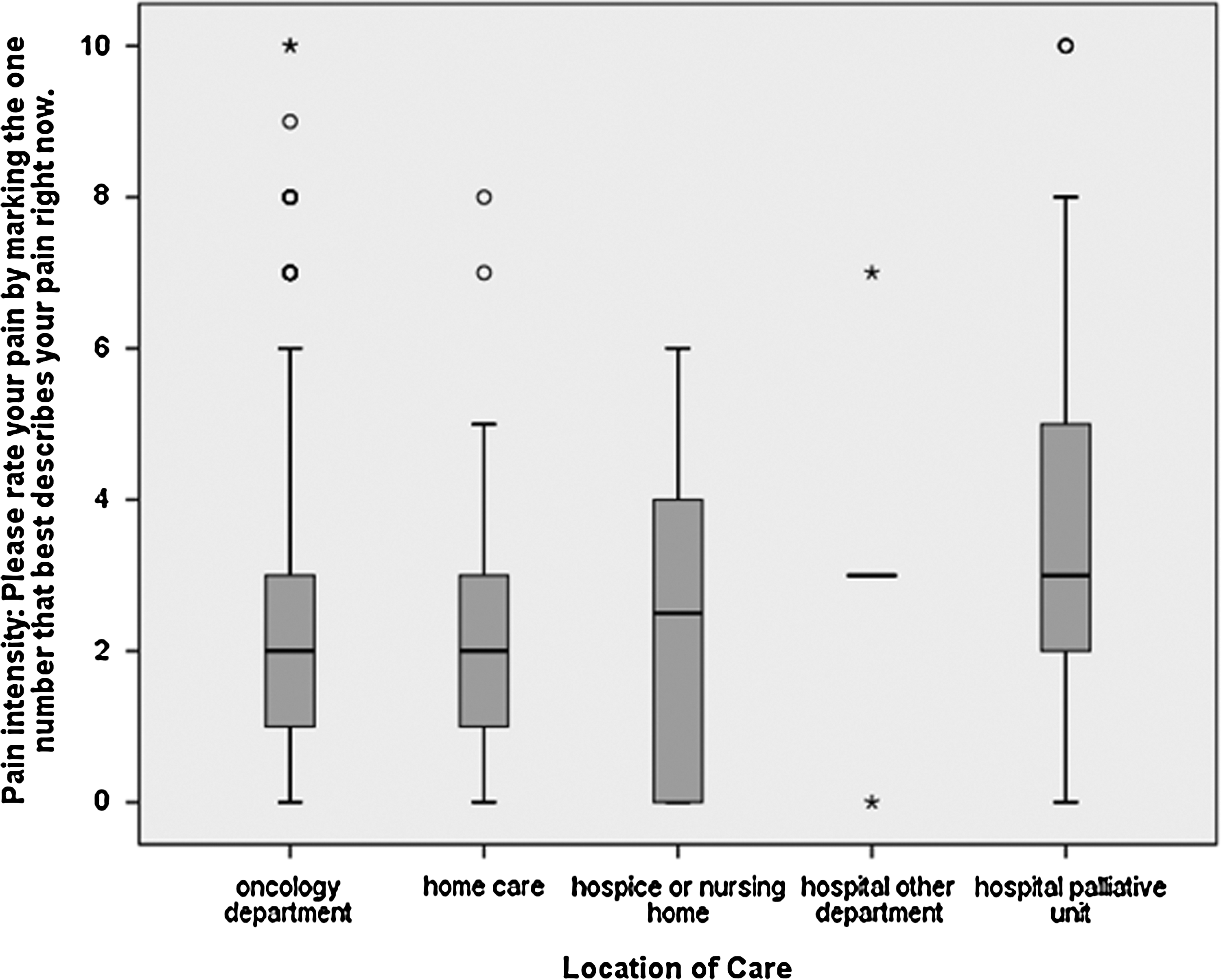
Box plots of pain intensity (rated right now) by location of care (n=574). (Note: Total does not add upto 670 due to missing data [n=96].)
Represents range in frequencies across the 17 sites.
Discussion
Two out of three patients in this study were clinically assessed as having cancer pain, with most pain patients (69.9%) reporting mild (0 to 3) pain intensity at the time of the assessment. The pain mechanism was predominantly nociceptive (79.7%). The overall prevalence of incident pain was relatively high (60.9%). About one in three patients (31.6%) were classified by clinicians as having psychological distress within the context of the pain experience. A smaller proportion of patients (4.5%) were classified as having addictive behavior, while most patients (91.9%) were classified as having normal cognition. Prevalence rates of pain classification features and pain intensity scores varied across collaborating sites and locations of care, with higher rates in more acute palliative care settings. Some participants who were not classified as having cancer pain still rated their pain as one or greater. It is possible that these ratings might have been due to noncancer pain.
Overall prevalence of neuropathic pain in this study was lower than reported rates of 28% 17 and 27% 5 in two previous ECS-CP studies; while prevalence of incident pain was considerably higher than in the other two studies (48% and 43%, respectively). Patients in this study had to be cognitively intact and relatively functional to take part in the computer assessments, which took an average of 30 minutes to complete, potentially excluding patients with more complex pain profiles or in acute pain crises. In contrast, the previous two ECS-CP studies used a consecutive sampling approach, in which all patients referred to a palliative care service, including cognitively impaired patients, were eligible. Clinicians completed the assessments, integrating patient-reported outcomes gathered as part of routine clinical practice. This design facilitated the inclusion of all patient referrals and minimized patient burden. The higher prevalence of incident pain in this current study might be related to a broader interpretation of this feature than in previous ECS-CP studies, highlighted by the wide range in frequencies across sites (i.e., 9%–81%).
The prevalence of psychological distress is in keeping with previously reported rates of 23% 17 and 44%. 5 The wide range in prevalence rates across sites (15%–75%) may be related in part to different levels of pain complexity. We cannot rule out the possibility that some of these differences may also be due to differing interpretations of the definition of psychological distress, for example, potentially including patients who were psychologically distressed but not necessarily within the context of the pain experience.
In contrast, the overall prevalence of addictive behavior was lower than expected in comparison with previous ECS-CP studies of 9% 17 and 11%. 5 There was a higher prevalence in some sites (range, 0%–50%), which may reflect patients with more complex pain profiles. It is not possible to discern the exact reasons for this wide variability.
The range of ECS-CP assessments across sites demonstrates the prevalence of pain classification features in a diverse international sample of advanced cancer patients. The variability was anticipated as a result of the types of patients admitted to specific sites, with patients with more complex pain profiles more likely to be admitted to acute palliative care settings. This is further supported by the variability in pain intensity ratings across the 17 sites, with the highest median pain intensity rating recorded on the Tertiary Palliative Care Unit (TPCU) in Edmonton; and across locations of care, with the highest median pain intensity rating and greatest variability for the hospital palliative unit setting. It is somewhat reassuring that 70% of those with cancer pain had reasonably well controlled pain (mild category) at initial assessment. These findings support the use of a pain classification system, not only for assessing and managing cancer pain, but also as a tool for benchmarking different sites and locations of care.
The ECS-CP can be used to create a cancer pain profile with standardized language and definitions allowing more appropriate pain management and better communication among interdisciplinary team members.4,18 In an internal audit of resource allocation in the Edmonton Zone Palliative Care Program (EZPCP), we demonstrated that the frequency of neuropathic pain, psychological distress and normal cognitive function was significantly higher in patients admitted to the TPCU when compared to other areas of the program, e.g. acute care and community, 19 justifying the increased resources available on the TPCU. However, some of this variation may have also been related to differences in interpretation of the ECS-CP, in spite of clinical bedside training, inservices and availability of the administration manual on the EZPCP website. 10
Differences in training and interpretation could certainly have affected the skill in using the ECS-CP in this study, where clinicians were expected to access the Administration Manual from the EZPCP website. At an International Knowledge Translation Symposium on the ECS-CP, the need to create a user-friendly manual was highlighted as a key next step to minimize the extensive reading needed for the comprehensive administration manual. 20 A “Quick User's Guide” to supplement the ECS-CP manual has now been made available. 21
The frequency of 92% normal cognition (range 64%–100%) and MMSE scores ranging from 10 to 30 further demonstrate the difficulty of achieving consistency in assessments. In this study where cognitive impairment was one of the exclusion criteria, these results raise interesting questions.
Implications for future research
The items included in the ECS-CP represent only initial efforts to define standard core variables. 1 Additional items, such as pain intensity, pain relief, age, cancer diagnosis, chronic pain history, and genetic variations, have been identified as worthy candidates for inclusion in a pain classification system.5,6,17,22–24 Recent work has suggested that some predictive models explain only 16%–26% of the variance of certain pain outcomes. 22 These findings were based on retrospective secondary data analyses and further research involving prospective study designs is warranted.
Recent advances in understanding of pain mechanisms, such as the revised neuropathic pain definition and grading system developed by the Neuropathic Pain Special Interest Group (NeuPSIG),25,26 could be incorporated in future studies. The positive relationship between cancer pain and systemic inflammation (C-reactive protein) in patients with cancer, 27 as well as basic research regarding bone and neuropathic pain, demonstrate the complexity of pathophysiology and potential oversimplification of current clinical classification. Nevertheless, present classification, as used in the ECS-CP, remains accepted convention to plan treatment. 28
Consistent training programs, use of inter-rater assessments and development of strategies to promote uptake of the ECS-CP need to be incorporated in future studies.20,24 The importance of psychological well-being, the relationship to coping with cancer pain, and the benefit of psychological interventions further highlight the importance of standardized screening for psychological distress, within the context of the pain experience, as part of cancer pain classification.29,30 Future study designs need to integrate clinician assessments with patient-reported outcomes that ideally are part of routine clinical practice, to minimize patient burden and obtain a representative sample of the palliative care population. A definition of an adequate pain response continues to present a challenge. A 2-point drop in a 10-point scale or 30% decrease in pain intensity is generally accepted and useful in clinical trials. 31 However, these definitions may not be appropriate to detect clinically relevant differences in advanced cancer and palliative care settings. 24 The use of personalized pain goals might have better prognostic importance as an outcome measure. 24 Another consideration is whether the pain intensity question should be framed as “over the last 24 hours” or “now.” 32
Limitations
This study was limited to a convenience sample of cognitively intact patients who could participate in an extended symptom assessment computer-based activity, which might have excluded patients with more complex pain profiles. Most patients reported mild pain and were recruited primarily from oncology departments and hospital palliative care units. Clinicians who conducted the assessments did not undergo any formal training program in using the ECS-CP. Some inconsistency in assessments is an inherent part of any assessment tool, particularly with multiple data collection sites in diverse health systems, using multiple languages. However, some of the differences across sites might have been due to differences in interpretation of the administration guidelines and definitions of classification features.
Conclusion
The ECS-CP is a clinically relevant systematic framework, which is able to detect differences in salient pain classification features across diverse settings and countries. The range of pain intensity scores likely reflects differences in patient complexity, referral criteria, and disease trajectory. However, further validation studies, including additional predictor variables, inter-rater assessments, improved definitions for some features, and refinement of outcome measures, need to be conducted in diverse settings to further develop the ECS-CP as an internationally recognized pain classification system.
Footnotes
Acknowledgments
The abbstract was presented at the European Association of Palliative Care (EAPC) Conference, Lisbon, Portugal, May 2011.
The European Palliative Care Research Collaborative is funded by the European Commission's Sixth Framework Programme (contract no LSHC-CT-2006-037777) with the overall aim to improve treatment of pain, depression and fatigue through translation research. Core scientific group/work package leaders: Stein Kaasa (project coordinator), Frank Skorpen, Marianne Jensen Hjermstad, and Jon Håvard Loge, Norwegian University of Science and Technology (NTNU); Geoffrey Hanks, University of Bristol; Augusto Caraceni and Franco De Conno, Fondazione IRCCS Istituto Nazionale dei Tumori, Milan; Irene Higginson, King's College London; Florian Strasser, Cantonal Hospital St. Gallen; Lukas Radbruch, RWTH Aachen University; Kenneth Fearon, University of Edinburgh; Hellmut Samonigg, Medical University of Graz; Ketil Bø, Trollhetta AS, Norway; Irene Rech-Weichselbraun, Bender MedSystems GmbH, Austria; Odd Erik Gundersen, Verdande Technology AS, Norway. Scientific advisory group: Neil Aaronson, The Netherlands Cancer Institute; Vickie Baracos and Robin Fainsinger, University of Alberta; Patrick C. Stone, St. George's University of London; Mari Lloyd-Williams, University of Liverpool. Project management: Stein Kaasa, Ola Dale, and Dagny F. Haugen, NTNU. The authors would also like to thank: Viki Muller (Research Administration) and John Hanson (Statistician).
Author Disclosure Statement
No confilicting financial interests exist.