
Abstract
Abstract
Background:
Overcrowded emergency departments (EDs) and the staff within them are often not able to address the complex physical and psychosocial needs of people at the end of life. While some studies have suggested that the ED environment should be adapted and staff trained to address this issue, there are no previous studies which have investigated whether the provision of timely palliative care services could prevent people with palliative care needs from attending EDs.
Objective:
This study investigates whether early admission to community-based palliative care reduces ED admissions in the last 90 days of life for patients with cancer.
Methods:
The study was a retrospective, cross-sectional study using death registrations and hospital morbidity data for 746 Western Australian adults who died of cancer and where palliative care may have been a viable and appropriate option for care.
Results:
In their final 90 days before death, 31.3% of decedents who had early access to palliative care and 52.0% of those who did not have early access to palliative care visited an ED (OR=2.86; 95% CI, 1.91, 4.30). Early admission to community-based palliative care reduces the use of EDs by cancer patients in the 90 days before death.
Conclusions:
Proactive care in the form of timely community-based palliative care assists in preventing vulnerable people at the end of life from being exposed to the stressful ED environment and decreases the pressure on EDs.
Introduction
There is an increasing recognition that EDs cannot cater to the complex needs of people where death is clinically expected. To date, international studies have focused on ED visits by people with cancer in their last months of life,1,11 palliative care patients 5 and older adults with possible palliative care needs13,14 or who receive a palliative care consultation following presentation to an ED, 15 and the increasing need for education of ED physicians in palliative care.16,17
Studies that focus on patients requiring palliative care in the ED are also methodologically challenged. It is often difficult to identify and classify which patients are palliative, or to recruit patients with palliative needs into ED studies, 18 so prospective studies are virtually nonexistent, with many studies based principally upon the perceptions of health care providers.9,13 A number of recent publications acknowledge the ED as an inevitable and important setting for identifying and addressing unmet palliative care needs and have proposed a range of approaches.3,10,19,20 Nevertheless, a palliative care model for ED is in the early days of formulation 21 and studies on suitable assessments for identifying palliative care need are exceptions rather than common practice.22–24
People approaching the end of life have complex physical, psychosocial, and existential problems. While a proportion of their problems undoubtedly requires treatment in an ED, the focus of palliative care is on the quality of life of the patient as well as the family. EDs have been designed for medical emergencies, so for some people at the end of life palliative emergencies could be avoided by providing appropriate alternative care. 25 However, little is known about how other health care services might prevent people with chronic progressive diseases such as cancer at the end of life from having to use EDs. This information is vital to ensure the most appropriate care for vulnerable people at the end of life as well as to inform health care resource allocation. There is a paucity of published studies that use rigorous population-based research to investigate the nexus between the ED and palliative care,1,2 and we have not been able to identify any that specifically examine the effect of palliative care services on reducing the number of palliative patients with cancer who attend EDs at the end of life.
Our study attempts to address this gap by describing attendances at EDs during the last year of life for cancer patients where palliative care may have been a viable and appropriate option for care. In other words, the people had died of a condition considered ‘amenable to palliative care.’ 26 Previously, the same dataset has been used to demonstrate hospital and ED use in the last year of life. 27 In this paper we investigate whether receiving ‘early’ admission to a community-based palliative care service reduces ED presentations for people with cancer in the 90 days before death compared to receiving no admission or a ‘late’ admission to a community-based palliative care service. In Western Australia, where the study was set, patients may receive the palliative care service as part of the ongoing medical care received, which may include mainstream and curative medical treatments and services.
The approach suggested in this paper is premised on the claim that proactive care, in the form of primary care, preventative care, and/or supportive services delivered in the community, should prevent a proportion of ED presentations. 28 We propose that the probability of presentations to an ED is influenced by both the person's medical needs as well as use of proactive care. Based on this assertion, we suggest that a proportion of ED presentations are potentially avoidable, particularly in situations where proactive care is delivered such that exacerbations and complications of the underlying morbidity(ies) are monitored and controlled. For the purpose of testing our proposition we chose community-based palliative care as an example of a suitable form of supportive care to explore its relationship to ED use. By comparing the ED use of people at the end of life who had received community-based palliative care with those who had not received community-based palliative care, we could determine if palliative care use helps avoid ED use.
In operationalizing this method we used a cohort of people from a population who had cancer and would have potentially benefited from palliative care.26,29 The method also incorporated timing of admission to community-based palliative care in relation to the emergency event/s. We chose 90 days before death as the point at which we distinguished between ‘early’ and ‘late’ admission to a community-based palliative care service. The pattern of decline in the last three months of life for people dying of cancer 30 indicates that patients in the last three months (approximately 90 days) are at high risk of death and arguably in need of palliative care. However, it is important to note that the choice of 90 days is arbitrary for the purpose of the method and there is no fixed point in time when palliative care should commence. Palliative care is relevant before the last weeks or months of life and many argue should be offered alongside curative treatments to people with chronic progressive diseases.31,32
Methods
Study design
This was a retrospective cross-sectional study of attendances at EDs in Western Australia by a cohort identified systematically through death registrations.
Participants
The inclusion criteria for the cohort were people who died between August 2005 and June 2006, were 18 years of age, had an informal primary carer, did not reside in a residential aged care facility, and died of cancer identified from the underlying cause(s) of death on the death registrations. Although not all people who die of cancer may require palliative care, we suggest the majority may benefit from palliative care. Underlying causes of death were grouped according to International Classification of Disease version 10, Australian edition (ICD-10-AM) codes. 33
Data
ED, hospital morbidity, and community-based palliative care data were linked to death registrations by the Western Australian Data Linkage System. 27 For the purpose of this study we defined an ED admission as the day in which the person was admitted to an ED, regardless of whether there was more than one admission on that day.
Statistical analysis
Descriptive statistics were used to describe the cohort. Age at death was grouped into three groups, being <65 years, 65–75 years, and >75 years; admission to community-based palliative care was grouped as ‘early admission to PC’ (between 91 and 365 days before death) and ‘no or late admission to PC’ (no admission or within 90 days of death); gender; and usual place of residence (metropolitan or rural) based on postcode. Frequencies were provided for the total number of days in hospital 91–365 days before death, grouped as 0, 1–10, 11–20, 21–30, or 31+ days. ED admissions in the 91–365 days before death were grouped as 0, 1–2, or 3+ admissions. Logistic regression was used to estimate the likelihood of admission to an ED overall and admission to an ED in the time 0–90 days before death. All reference to ‘palliative care’ refers to community-based palliative care. Statistical analyses were carried out using the R statistical computing language. 34
Ethics approval was obtained from Curtin University Ethics Committee, Silver Chain (the community-based provider of palliative care), and the Confidentiality of Health Information Committee, Health Department of Western Australia.
Results
The cohort comprised 746 decedents, the majority of whom were male (61.8%). One-half of the cohort were aged ≥72 years (range 20–95; mean 69.7; SD 12.5) and three-quarters (74.9%) lived in the metropolitan area of Perth, the major city of Western Australia, in their last year of life. All decedents died from cancer.
Two-thirds (65.8%) of the cohort were admitted to an ED in their last year of life. Similar proportions of males and females (65.3% and 66.7% respectively) were admitted to an ED; and similar proportions were observed in the different age groups: 69%, 65%, and 64% for <65 years, 65–75 years, and 75+ years, respectively. Of those people who lived in the metropolitan area, 63.5% were admitted to an ED in their final year of life as opposed to 72.7% of patients from a rural area. A logistic regression examining people who were admitted to an ED in the final year of life as a response indicated that only location had a statistically significant impact on overall ED admissions, with metropolitan patients more likely to be admitted to an ED (OR=1.53; 95% CI 1.06, 2.21). The total number of admissions to an ED by this cohort was 1256. The number of admissions per patient to an ED ranged 0–16 (mean 1.68; SD 2.05), with one-half of the cohort (n=382, 51.2%) being admitted to an ED 1–3 times.
In the cohort there were 670 ‘early admissions to an ED’ (53.3%) and 586 ‘late admissions to an ED’ (46.7%). There were 392 people who were not admitted to an ED in the 90 days before death (52.6%), while 302 people had 1–2 admissions (40.5%) and 98 people had >2 admissions (7.0%). Table 1 provides the frequencies of potential predictor variables and the proportion of people who had ED admissions in the 90 days before death.
All numbers rounded up.
ED, emergency department; PC, palliative care; WA, Western Australia.
Three different models were fitted to describe the impact of potential predictor variables on whether the patient was admitted to an ED in the 90 days immediately prior to death. The first model examined the impact of gender, age group, usual place of residence, and admission to community-based palliative care. Only whether the individual had an early admission to palliative care (that is 91–365 days before death) had an impact on whether the patient was admitted to an ED in the 90 days before death. People who had no palliative care or were admitted to palliative care within 90 days of death were more likely to visit an ED in the 90 days before death (OR=2.38; 95% CI, 1.64–3.44).
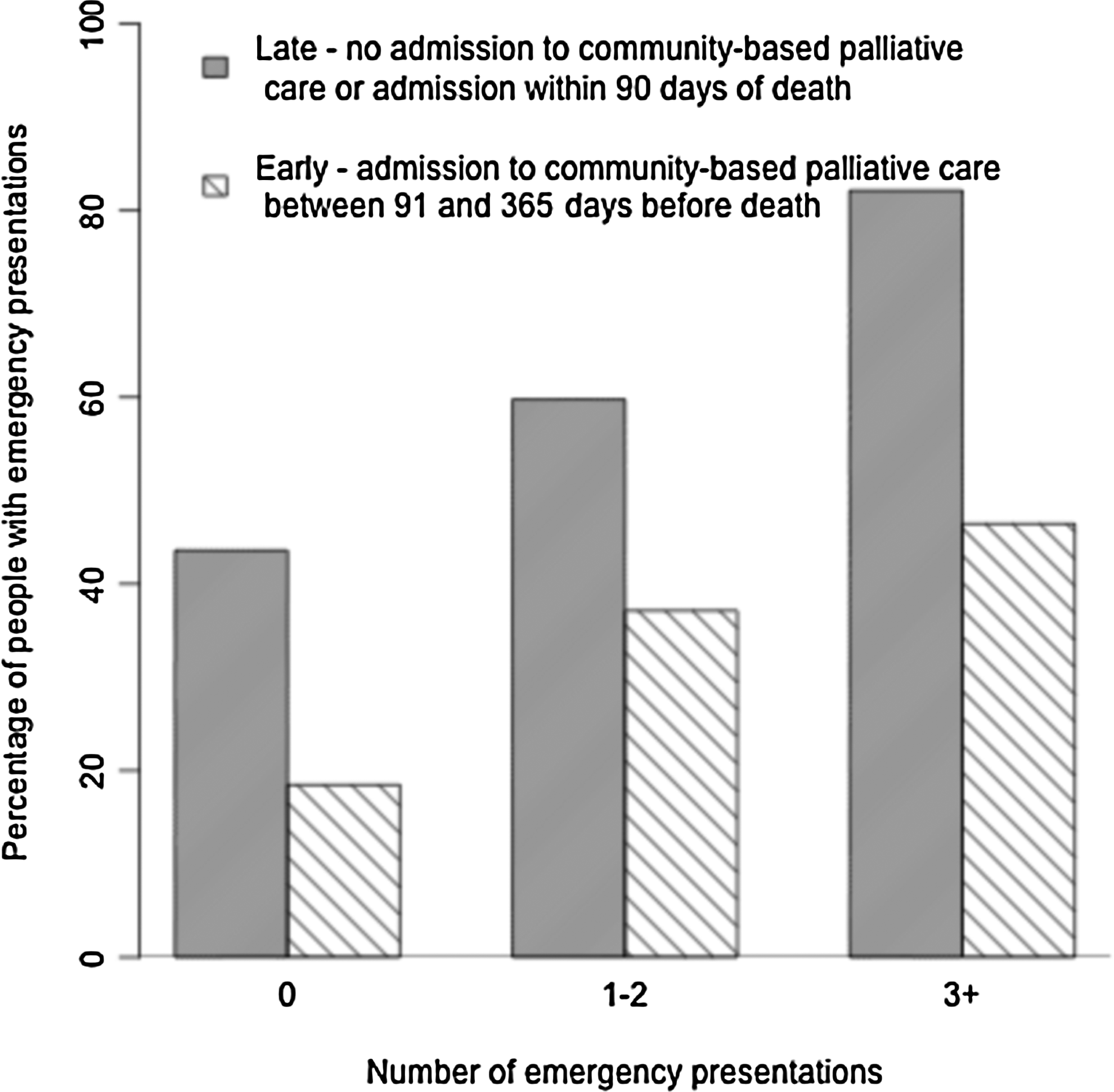
In addition to the variables considered in the first model, a second multivariate model (see Table 2) allowed adjustments to be made for both the number of ED admissions and the number of days in hospital 91–365 days before death. Both of these were found to be statistically significant predictors of an ED admission in the 90 days before death. ED admissions 91–365 days before death indicated a higher likelihood of being admitted to an ED in the last 90 days, while people who spent more time in hospital 91–365 days before death were less likely to be admitted to an ED in the last 90 days. Adjusting for these variables, again, decedents who did not have an early admission to palliative care remained significantly more likely to have an ED admission in the last 90 days. These findings are illustrated in Figure 1 and Table 2.
Effect of early admission to community-based PC versus late admission to community-based PC.
Adjusting for ED days in hospital and non-ED days in hospital 91–365 days before death.
Community-based palliative care.
CI, confidence interval; ED, emergency department; NS, non-significant; OR, odds ratio; PC, palliative care.
A third multivariate analysis, similar to the second model, adjusted for the number of days a patient could be admitted to an ED in the last 90 days before death. If a patient was in hospital during the last 90 days, one could assume he or she could not be admitted to an ED. Including this variable as a covariate in the analysis indicated that people who spent more time in hospital in the 90 days before death were still more likely to have an ED admission. The impact on the other variables was negligible. A cross-validation was completed. Instead of using 90 days as the cut-off for analyses, a sensitivity analysis was completed using both 60 and 120 days. In each case, early admission to a community-based palliative care service was statistically significant: 60-day early admission to palliative care (OR=2.78; 95% CI 1.89, 4.09) and 120-day early admission to palliative care (OR=2.33; 95% CI 1.51, 3.59). This cross-validation provides further evidence of the significance and consistency of the variables predicting ED admissions closer to death when the 90 day cut-off is varied.
Discussion
By employing a retrospective population-based approach, this study was able to describe the use of EDs by people in their last year of life who died of cancer and where palliative care would have been a viable and appropriate option. In addition, the cohort described did not live in a residential aged care facility and had a primary carer who enabled them to be cared for in the home. Consequently they were eligible for community-based palliative care should they choose to use the services. In Western Australia these services are freely available, providing a medical practitioner refers the patient to the service. Our premise, that the provision of alternative supportive care in the form of community-based palliative care would reduce attendance at an ED by this group, was supported. People who did not receive community-based palliative care, or who had a late admission (that is admitted in the 90 days before death), were more likely to be admitted to an ED in the last 90 days of life than people who had early admission to palliative care (that is 91–365 days before death).
The method employed in this study enabled us to focus on a cohort of people who had died of cancer, where death would have been clinically expected, and therefore where palliative care was likely a viable and appropriate option for care.27,35 Cancer takes a more predictable course than other end-stage diseases. Where cancer patients have been reported to be highly functional early in their final year of life but markedly more disabled in the three months prior to death, organ failure patients are reported to experience a fluctuating pattern of decline with substantially poorer function in the three months before death. 30 We argue that this level of predictability enables health care professionals to judge when palliative care may be appropriate. In addition, in Australia, as elsewhere, patients with cancer are more likely than noncancer patients to receive community-based palliative care services. 26
Some people approaching the end of life will clearly need the immediate and acute care provided in an ED and this can only be determined in a clinical context. It may be that in our study people attended the ED for problems other than those associated with their palliative condition. However, many ED admissions could be avoided if alternative support was available either through primary care providers or community-based palliative or supportive care services. Many admissions to an ED of people in their last months of life are potentially avoidable. A recent Canadian study found people dying of cancer used the ED for visits that were preventable including visits to address constipation, adjustment of urinary catheters, prescription refills, and for technical and mechanical reasons. 1 Another pilot project designed to identify ‘palliative care triggers’ in EDs found many chronically ill older people who were admitted to an ED had complex psychosocial problems and limited access to support systems and homecare services along with their medical problems. 13 Palliative care services are much better placed than EDs to provide the holistic, multidisciplinary, and time intensive care needed by people at the end of life.
The limitations of this study are those faced by studies that rely on administrative health data where the data is not collected specifically for research purposes. 36 This means that the data was not collected with the intention of answering the specific research questions. In addition the sample size was relatively small, which restricted the analysis of subgroups of the population in relation to particular ages or disease groups. Despite these drawbacks, the strength of our study is that for any one participant, we have been able to link their death registration with ED, hospital admission, and community-based palliative care data from all health services in Western Australia. This adds substantially to an underdeveloped research area where the findings to date are mixed, dependent on the classifications of the cohorts attending EDs and the methodologies used. 28 Many of the studies cited in this paper lack the statistical power afforded by the population-based analysis used in our study.
It is evident from the literature on end-of-life and EDs that few if any studies have been able to adequately identify use, need, and outcomes for individuals and health services. While this study does not purport to address all of these concerns, it goes some way to starting the investigation by describing ED use for a group likely to benefit from palliative care and by demonstrating that early admission to palliative care reduces the use of EDs in the 90 days before death.
Footnotes
Author Disclosure Statement
No conflicting financial interests exist.