
Abstract
Abstract
Background:
Patients with nonmalignant respiratory diseases have limited access to palliative care services and health professionals do not adequately address discussions about end-of-life care preferences.
Objective:
The aim of this systematic literature review was to highlight key components and challenges for patients and health professionals discussing end-of-life care in nonmalignant respiratory disease.
Design:
A mixed methods systematic review was conducted. Included studies were assessed for quality and data were synthesized thematically, while original data were presented in tabular form.
Data Sources:
PubMed, CINAHL, BNI, ASSIA, PsycINFO, Science Direct, and Web of Science were searched (1999–2010) for studies on end-of-life discussions. Additional studies were identified by hand searching key journals and reference lists of included articles.
Results:
Fourteen studies were identified. Three themes involving components and challenges in end-of-life discussions were identified: the discussion, the health professional/patient relationship, and patient perceptions.
Conclusions:
End-of-life discussions should be initiated by health professionals, who must be aware of patient expectations regarding palliative care and end-of-life care planning. Efforts must be made to develop relationships with patients with terminal illness and allow sufficient time to discuss the end of life during clinical encounters. Future research should address palliative care uptake in nonmalignant disease and implications for health education should be addressed.
Introduction
As patients with nonmalignant respiratory disease have less access to palliative care services than patients with other respiratory diseases (e.g., lung cancer), Partridge 6 proposed formal policies to assist them to receive a satisfactory level of palliative care services. However, the personal nature, individual preferences for end-of-life discussions, and the unpredictable disease trajectory in nonmalignant respiratory disease make this difficult.7–10
In a study about when and how to initiate end-of-life discussions with patients with a terminal illness, carers and health professionals agreed that end-of-life discussions should take place when the patient is ready, but also indicated that many patients waited for health professionals to raise the topic. 11 However, enabling continuity of care can be challenging and physicians may not be allocated sufficient time for meaningful conversations with patients. In nonmalignant respiratory disease, the unpredictable disease trajectory may also make timing such discussions difficult. 10 Communication difficulties arising from poor health and breathlessness associated with respiratory disease are likely to add further barriers to discussion. 12 Given the lack of palliative care services available 6 and the greater prevalence of anxiety and depression associated with nonmalignant respiratory disease, 13 end-of-life discussions are crucial in this context.
This systematic review of the recent literature aims to highlight key components and challenges for patients and health professionals discussing end-of-life care in nonmalignant respiratory disease.
Methods
Design
Prior to the systematic review, a protocol outlining inclusion/exclusion criteria and the methods of analysis was developed according to the review method proposed by Petticrew and colleagues.
14
The review method—question development, literature search, study screening, data collection and analysis, quality appraisal and synthesis—allows for statistical or narrative synthesis of included studies. As the review guidelines are general, other sources (e.g., for quality appraisal and synthesis)1,16 were incorporated into the method when necessary. The review was conducted in accordance with PRISMA guidelines.
15
The components of the review question using the PICO framework are:
14
• Population: Health professionals who care for patients with life limiting, progressive nonmalignant respiratory disease. Studies on carers were included if carers reported on the deceased patient's experiences.
16
Studies that addressed nonmalignant respiratory disease and other life limiting conditions were included. • Phenomena of interest: End-of-life discussions between patients with a life limiting progressive nonmalignant respiratory disease or their carers and health professionals. • Context: Any setting where end-of-life discussions occur.
Search strategy
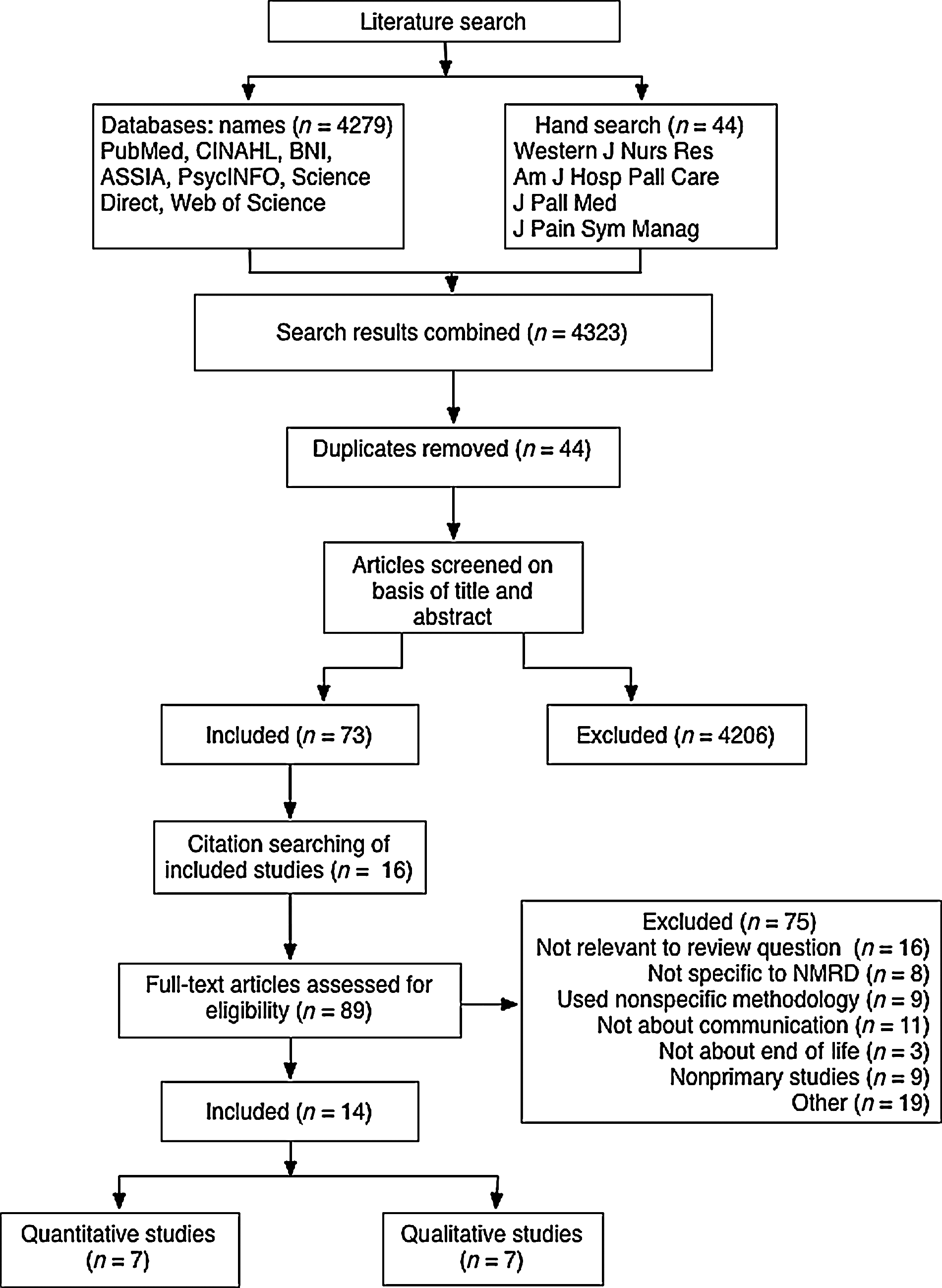
A broad preliminary search was conducted in PubMed and CINAHL to identify relevant keywords to develop the search strategy. PubMed, CINAHL, BNI, ASSIA, PsycINFO, ScienceDirect, and Web of Science were searched (11/2009–2/2010) for peer-reviewed literature published 1999 to 2010. The Journal of Palliative Medicine and the Journal of Pain and Symptom Management were hand searched, as they yielded the most relevant results in the database search. Reference lists of included articles were searched. This process conformed strictly to PRISMA guidelines
15
(see Figure 1). Search terms or equivalent medical subject headings are detailed in Table 1. Screening of the studies was conducted by the first author. Studies were included if they met the PICO criteria and
• reported primary research conducted using a specified qualitative or quantitative methodology, • were conducted in any country, were published between 1999 and 2010 in a peer-reviewed journal in English, • involved participants aged 18 years or over.
Search and review process
19, 20, 36, 42 denote that search term items listed (e.g., 1 to 18) were combined using the boolean term OR between them, meaning that the database searched “terminal care” OR “terminally ill” OR “chronic disease” OR etc., which provided results of any database item containing any of these terms. 43 indicates that the results of searches conducted in 19, 20, 36 and 42 were combined using the boolean term AND in the database which provided results of database items containing items from each search group e.g., a database item that included “palliative care,” “communication,” “patient satisfaction,” “nurses.”
MeSH, medical subject headings.
Reviews were excluded to ensure that evidence was not duplicated. The authors reviewed the studies for inclusion, and any discrepancies were discussed until a consensus was reached.
Search outcome
A total of 4279 titles from databases and 44 titles from hand searching journals were identified. After 44 duplicates were removed, the selection criteria were applied in an unblinded standardized manner to 4279 abstracts to narrow down the results to 73 papers. Fourteen papers were added from citation searching, resulting in 89 papers that were read in full. The 14 articles selected for inclusion were seven quantitative studies and seven qualitative studies. Figure 1 demonstrates the search process, including reasons for exclusion.
Appraisal of papers
Qualitative and quantitative papers were evaluated by the assessment criteria developed by Kmet and colleagues to provide information on the relative methodological quality of studies in the review. 17 To validate the critical appraisal, the second author assessed 5 of the 14 studies. The authors of the assessment criteria suggest a cut-off between 0.55 and 0.75; we set a cut-off of 0.60 to allow for relevant papers of satisfactory quality to be included. 17 The scores for the qualitative studies ranged from 0.65 to 0.9/1 (mean=0.79), while those for quantitative studies ranged from 0.68 to 0.95/1 (mean=0.83), with an overall mean of 0.81 for both groups (see Tables 2 and 3).
The summary score for quantitative studies is calculated by determining the total sum of scores, then subtracting it from the total possible sum (28 – number of NA x 2), and then dividing the total sum by the total possible sum. Items are scored for the degree that they meet the criteria for each question detailed by the authors of the quality appraisal guidance: 2=yes, 1=partial, 0=no. NA=not applicable.
The summary score for qualitative studies is calculated by dividing the sum of scores by the total possible sum (20). Items are scored for the degree that they meet the criteria for each question detailed by the authors of the quality appraisal guidance: 2=yes, 1=partial, 0=no.
Synthesis
Data were extracted into a summary table (see Table 4) by two authors to enable comparison across studies.14,18,19 Qualitative and quantitative findings were subjected to thematic analysis, providing a structure for organization of the findings. 20 While the controversy regarding synthesizing qualitative and quantitative evidence in systematic reviews is well documented,21,22 thematic analysis is commonly used to identify the key themes in a set of studies. This method is enhanced by using tabular summaries to add a greater degree of synthesis.19,21
AIDS, acquired immune deficiency syndrome; CHF, chronic heart failure; CIV, conversational interviews; CNA, case note analysis; COPD, chronic obstructive pulmonary disease; EOL, end of life; GP, general practitioner; HF, heart failure; RCT, randomized control trial; SSIV, semistructured interviews; X, cross-sectional survey.
Recurrent themes were identified and topics were summarized under thematic headings. 20 Original evidence was preserved in the summary table. Equal weight was given to qualitative and quantitative data in the synthesis.
Results of each paper were coded: codes were grouped into categories and entered in a table. Categories were grouped into common themes using a mind map (a diagram where ideas are pictorially represented and linked to a central idea).20,23 The authors discussed and reached a consensus on themes.
Results
The review process revealed several consistent themes throughout the included literature. The findings were organized within three themes—the discussion, the health professional/patient relationship, and patient perceptions.
The end-of-life discussion
Style and content are key components of end-of-life discussions with patients with nonmalignant disease. This theme includes how and when the discussion is initiated, barriers to discussion, patient concerns about the end of life, and patient information needs.
Discussing prognosis is a component of such discussions that helps determine when to move away from aggressive life-sustaining treatments. 24 Patients' end-of-life concerns include facing the end of life and awareness of impending death; 25 changes in daily living with a terminal illness; 26 and the lack of treatment options, 27 which often led patients to consider end-of-life issues. 27 Curtis and colleagues 28 found three discussion areas in need of improvement: prognosis, death, and spiritual issues. While patients may want prognostic information soon after diagnosis, they may not want to raise the issue themselves, 29 placing an emphasis on the willingness of the health professional to initiate the discussion. 30 Lofmark and Nilstun 31 found seriously ill patients valued frank discussions about forgoing life support, even within short clinical encounters.
Elkington and colleagues 26 found 72.5% of GPs thought discussions of prognosis were necessary or essential in severe chronic obstructive pulmonary disease (COPD), while 82% felt GPs had an important role in such discussions. Patients were not generally harmed by talking about their prognosis, 31 yet one study found only 32% of patients with COPD discussed the end of life with their physician, with more facilitators for communication resulting in more end-of-life discussions. 9
General practitioners (GPs) may not discuss end-of-life because they feel unprepared and find starting such discussions difficult. 26 Only 41% of GPs in the same study reported often or always discussing prognosis with patients with severe COPD, 26 while some did not discuss prognostic information because of insufficient information in the primary care notes. 26
Barriers to discussion most frequently endorsed by patients were uncertainty about what type of care patients wanted and which doctor would be providing care. 9 Unsurprisingly, the greater number of barriers reported, the less likely it was for discussions to occur. 9
Style of communication was found to be an important factor; for example, listening to patients and encouraging questions was important for successful communication. 30 A lack of awareness of end-of-life options may be connected with the patient using denial as a coping mechanism therefore sensitivity to such coping mechanisms was important in preparing for and conducting discussions. 30
Health professional/patient relationship
The importance of the health professional/patient relationship has been emphasised in observations of end-of-life communication. This relationship appears to involve a power component, with patients expecting providers to be competent, provide consistent caring, and be all-knowing.25,29 Patients may wish to avoid confrontation with nurses over decision making, due to the uncertainty of their situation and fear of repercussions that may arise from challenging an expert. 29
The balance between honesty and hope when communicating with patients was a common theme: two studies found this was important for good end-of-life communication.30,32 Patients wanted to be informed of what may happen; 29 however in one study of GPs, half were undecided as to whether most patients with COPD wanted prognostic information. 26 Patient hope was decreased when discouraging medical facts were discussed and information was presented bluntly or the health professional was perceived as cold. 32
Variations in the relationship style between health professionals and patients may be related to the model of care. Grbich and colleagues 33 claimed a lack of evidence for use of a holistic palliative care model, while Clover 29 did not find evidence of patient-centered care and found that at times nurses missed opportunities to discuss the end of life. The authors 25 reported that at times patient choice regarding care was impeded by the actions and communication style of the health professionals. Patients often adopt the style of communication of the health professional; therefore it is essential that an open, patient-centered approach is used. 29
Patient perceptions
Discrepancies between the reports of the different participants in end-of-life discussions between health professionals and patients were found. One study found that when patients inaccurately predicted their life expectancy, they also misperceived any occurrence of communication. 34 The same study found patient and health professional agreement was low on whether prognosis had been discussed: health professionals felt they had provided prognostic information more often than patients reported. 34
Financial status and race of the patient may play a role in agreement between health professionals and patients about the occurrence of end-of-life discussions. While no patient profile can predict individual end-of-life communication needs, 35 noncaucasian patients with lower economic status were more likely to agree that end-of-life discussions about prognosis occurred. 36 As patients in these groups have a propensity to favor life-sustaining treatments, 36 health professionals may put more effort into communicating end-of-life options with them. The patient's apprehension may impact on his or her desired level of information, some may rate illness-related issues, such as social effects, as more important than disease-related issues such as prognosis and treatment. 35 The clear impact on patient mental health was demonstrated by improvements in functional status, anxiety, depression, and preparation for end-of-life in a randomized controlled trial with an active end-of-life discussion intervention. 37
Discussion
The studies in this review were highly varied in methodological approaches, indicating a wide range of research in this area. The review adds to current knowledge by revealing several key components of end-of-life communication in nonmalignant respiratory disease and the numerous challenges faced by health professionals and patients, summarized in Table 5.
The most prevalent component was the style of the communication including the desire for two-way communication, the existence of power issues, and the importance of honest yet hopeful communication. In 1995, authors of a systematic review found a correlation between successful health professional/patient relationships and improved patient health outcomes. 38 The importance of the style health professionals use to communicate with patients has been recognized in several types of patient/health professional interactions. Buller and Buller 39 found patients reported less satisfaction when physicians used a controlling style of communication. In another study, when health professionals exhibited patient-centered behaviors, patients were more satisfied with the interaction, felt understood, and felt their concerns were resolved.40,41 Snoek and Skinner 42 found patients with diabetes reported higher satisfaction with health care visits when they felt communication was bidirectional between physicians and patients, with awareness and recognition of facilitators and barriers to end-of-life communication being important. Other key components were (1) the health professional's recognition of the patient's desire for information about prognosis and subsequent care options, (2) initiation of the end-of-life topic by the physician or health professional, (3) an appropriate environment for the discussion, and (4) provision of prognostic information. Findings by Jones and colleagues 43 show that information about the future course of their illness was reported as a major issue for patients with COPD, with patients having varied opinions on how much prognostic information they desired. This is a major issue for end-of-life communication, as prognostic information is difficult to provide in COPD due to the unpredictable disease trajectory. 10 These factors must all be considered within the context of changing patient information needs during chronic illness.
These findings imply health professionals should not assume they know what patients want in terms of end-of-life communication, as preferences vary between patients. Instead, individual needs can be discerned by having preliminary planning discussions with patients. Preliminary discussions should be initiated by the health professional to determine whom the patient wants present for the discussion, when it will take place, and the appropriate environment. While the health professional/patient relationship may be key to a successful discussion, also important are style of communication and the health professional's ability to communicate honestly while conveying hope. This means that in addition to the health professional's willingness to present choices and have two-way conversations with patients, he or she must give information in a way that does not take away hope for the future. Being honest, hopeful, supportive, and encouraging at the same time is a difficulty for many health professionals. 44
Discussions may need to occur more than once to ensure both parties are clear on the prognosis, the agreed plans, and to ensure questions get answered while changing information needs and care preferences are addressed. This is particularly important when patients have repeat admissions to the hospital due to exacerbations, as their experiences may change their needs or preferences. Rizzo and colleagues 45 have recently found that the Stages of Change Transtheoretical Model is useful as a flexible way to handle end-of-life conversations, facilitating more meaningful communication. The review findings are congruent with Momen and colleagues' findings that patient preferences for end-of-life communication are highly individual, and health professionals need to facilitate such discussions based on patient wishes in COPD. 46
This review included papers that looked at nonmalignant respiratory disease exclusively or alongside other conditions such as heart disease and cancer. Interestingly, the papers that looked at nonmalignant respiratory disease exclusively were all questionnaire studies with patients, physicians, or both. Much could be gained by conducting in-depth interviews with health professionals and patients with nonmalignant respiratory disease about their experiences or approaches to end-of-life discussions.
A limitation of this review is the range of countries from which data were obtained. The included studies were produced by countries with a wide range of health care systems, from nationalized to private, however only studies published in English were included and those all originated in Western countries. As a result, cultural variables were not explored in this review and were rarely addressed in the included studies. A second limitation of this review is that the scoring system used for the quality appraisal did not provide specific guidelines for what constituted a poor or excellent review. Therefore, the quality of included papers relative to other papers in the review is known, but not quality compared to literature in general.
Conclusions
This review has identified several key components of end-of-life communication in nonmalignant disease (detailed in Table 5); however, these are not always evident in the patient experience. Assignment for each patient of a key health professional responsible for discussing the end of life and ensuring wishes are communicated between settings may improve the patient experience and likelihood of end-of-life discussions.
End-of-life communication is challenging but essential to enable scarce palliative care resources for patients with nonmalignant disease to be utilized appropriately: health professionals must make this a priority. This also has implications for health professional education: to ensure professionals are trained and confident enough to have such discussions. Practitioners are increasingly providing palliative care without specialist training, and while palliative care rotations are becoming more common in medical training, improvement is required. 47 Future research should address more widespread implementation of training programs in disease-specific palliative care communication and delivery and should measure the resulting effect on uptake of palliative care in nonmalignant disease.
Future research could also address how more palliative care resources may be allocated to patients with nonmalignant disease by determining effective ways to use existing cancer palliative care services for other patient populations.
Footnotes
Author Disclosure Statement
The authors declare no conflict of interest.