
Abstract
Abstract
Background:
The ambulatory care setting is a new frontier for advance care planning (ACP). While electronic health records (EHR) have been expected to make ACP documentation more retrievable, the literature is silent on the locations of ACP documentation in EHRs and how readily they can be found.
Objective:
The study's objective is to identify the locations of ACP documentation in EpicCare EHR and to determine which patient and primary care provider (PCP) characteristics are associated with having a scanned ACP document. A scanned document (SD) is the only documentation containing signatures (unsigned documents are not legally valid).
Design:
The study design is a retrospective review of EpicCare EHR records. The search of terms included advance directives, living will, Physician Orders for Life-Sustaining Treatments (POLST), power of attorney, and do-not-resuscitate.
Setting/subjects:
Subjects were patients in a multispecialty practice in California age 65 or older who had at least one ACP documentation in the EHR.
Measurements:
Measurements were types and locations of documentation, and characteristics of patients and physicians.
Results:
About 50.9% of patients age 65 or older had at least one ACP documentation in the EHR (n=60,105). About 33.5% of patients with ACP documentation (n=30,566) had an SD. Patients' age, gender, race, illnesses, and when their physician started at the medical group were statistically significantly associated with the probability of having a scanned ACP document.
Conclusions:
Only 33.5% of patients with ACP documentation somewhere in the EHR had an SD. Standardizing the location of these documents should become a priority to improve care. Actions are needed to eliminate disparities.
Introduction
The ambulatory care setting is a new frontier for ACP. 6 Discussions with patients to elicit their preferences may be wasted if providers cannot readily access those preferences when necessary.7–9 Physicians in both the outpatient and inpatient settings have used a number of places in EpicCare electronic health records to document such discussions or decisions, including the problem list, progress notes, or as a scanned document under “encounter.” Such diversity in storage locations could make it difficult for physicians to retrieve this important information, especially under time constraints. While the inaccessibility of advance directives has been documented in the past, those studies usually used paper charts. 3 The literature is silent on the accessibility of ACP documentation using the EHR.
Within ACP documentation, advance health care directives (AHCD) and Physician Orders for Life-Sustaining Treatment (POLST) are the two main documents that physicians look to retrieve. AHCDs are legal documents (including living will, durable power of attorney) and are promoted for all adults. Living wills detail patients' wishes regarding life prolonging treatment. 5 Durable power of attorney designates a surrogate decision maker should the patient become incapacitated. In contrast, POLST is used to translate patient preferences into specific medical orders to be honored by all health care professionals. It is recommended for patients with a life expectancy of one to two years, and contains three sections: Cardiopulmonary Resuscitation, Medical Interventions, and Artificially Administered Nutrition. 10 POLST forms must be signed by the patient or surrogate (in most states) and the physician making the order.
The purpose of this study is to assess where and how ACP decisions or discussions are documented in EpicCare EHR within a large, multispecialty ambulatory group practice in northern California. Our research questions were (1) Where are ACP documentations located? (2) Are they easily accessible to physicians? and (3) What patient and primary care physician characteristics are associated with having a scanned ACP document? We use the term “location” to refer to where in EpicCare EHR the ACP documentation is found—in the problem list (PL) tab, progress notes, or as an SD found under the “encounter” tab. We considered a patient's documentation to be “accessible” if it was found on the PL, because it is one of the first places physicians look for ACP decisions and it is highly visible. We examined the patient and PCP characteristics associated with having an SD specifically because that is the only documentation containing signatures. Unsigned documents are not legally valid.
Methods
Sample
To be included in this study, patients had to meet all of the following criteria: (1) be an active patient, as defined by having had at least two in-person visits to primary care (internal or family medicine) between September 2008 and September 2011; (2) age 65 or older at the start of the study period (2008); and (3) have at least one ACP documentation in the EHR between January 1999 and September 2011. Patients met the criteria of having ACP documentation in the EHR if they had ACP on the PL, an SD containing an ACP decision, or a progress note containing an ACP term. (See Appendix 1 for search terms).
Data analysis
We used univariate and bivariate descriptive statistics to analyze the locations of the ACP documentations, as well as the characteristics of patients and PCPs in the study sample. We used a binary logistic generalized estimating equations model to examine the probability that a patient had a scanned ACP document. The dependent variable equals 1 if the patient had a scanned ACP document and 0 if they did not have a scanned ACP document. The model accounted for the clustering of patients within physicians. Explanatory variables for patients included age in 2008, gender, race, and health status as measured by a vector of diagnoses for major illnesses such as circulatory disease, chronic obstructive pulmonary disease, cancer, liver disease, kidney disease, and dementia. Physician variables included gender, specialty (internist versus family medicine), and an indicator variable for started working at the medical group after 2000, which was a proxy for experience as a practicing physician in the group. The year 2000 was chosen because the average tenure of physicians at the group is about 10 years. The above model was estimated for three separate groups of patients: all patients with ACP documentations, patients with POLST documentation, and patients with advance directive/living will (ADLW) documentation. Categorical variables were centered. 11 The organization's institutional review board approved the study.
Results
Locations of ACP documentation
We reviewed the charts of 60,105 active patients age 65 years or older over the three-year period. A total of 30,566 (50.9%) of these patients had ACP documentation in the EHR.
The locations of the documentation are summarized in Figure 1. About 33.5% of patients with ACP documentation had an SD. About 6.2% had an SD and documentation in the PN, 4.5% had an SD only, 1.2% had an SD and PL entry, and 21.6% had documentation in all three locations.

All patients with any ACP documentation: Location of documentation in the EHR (n=30,566 patients).
When we examined patients with POLST documentation, the vast majority (95.8% of the 7486) did not have an SD (see Figure 2). About 84.3% of these patients had the documentation located in the PN only. Notably, 11.5% of patients with a POLST documentation had POLST on the PL but no corresponding SD, and 2.9% had an SD but no indication on the PL.
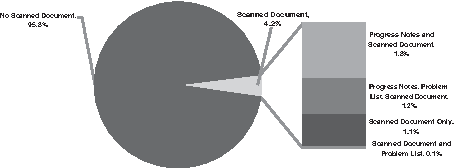
Locations of POLST Documentations (n=7,486 patients).
Figure 3 shows the EHR locations of the ADLW documents. About 34.8% of patients had an SD. About 4.7% of patients had an SD and PN documentation, 6.8% had an SD only, 1.9% had an SD and PL entry, and 21.3% had documentation in all three locations. About 32.9% of ADLW patients had an indication on the PL but no corresponding SD. About 11.5% of patients had an SD but nothing on the PL.

Locations of Advance Directive/Living Will Documentations (n=28,400).
To understand the difficulty a physician faces in finding ACP forms not identified on the PL, we examined the total number of documents patients had scanned into the system per year. While the mean was 4 (median=2), the maximum was 231 SDs per patient per year (of which the maximum of ACP documents was 6).
Patient characteristics
The demographic characteristics of patients in the sample are shown in Table 1. In 2008, the mean patient age was 75 years. About 60.6% of patients were female, 29.8% were nonwhite, and 9.2% died during the study period. With respect to patient diagnoses, 90.5% had a diagnosis of circulatory disease, 30.9% had a diagnosis of COPD, 27.2% of cancer, 26.4% of kidney disease, 10.3% of dementia, and 2.6% of liver disease.
p<0.05
p<0.01
Circulatory disease was identified by ICD-9 codes 390–459. Cancer includes all cancers other than nonmelanomatous skin cancer.
Based on EHR records and data from the Social Security Death Index.
Physician characteristics
Patients in the study sample had a total of 284 PCPs (see Table 1 for PCP characteristics). About 65.5% of PCPs were female, and 63.0% started working at the medical group after 2000. About 49.3% were internists, with the remaining practicing in family medicine.
Bivariate analyses
Results from the bivariate analyses are shown in Table 1. Disproportionately more female patients (35.1%, p<0.01); patients with a diagnosis of cancer (39.3%, p<0.01); and dementia (44.8%, p<0.01) had a scanned ACP document. Patients with scanned ACP documentation were significantly older (77 versus 75, p<0.01). Disproportionately fewer nonwhite patients (23.8%, p<0.01); patients with a diagnosis of liver disease (28.5%, p<0.01); and patients with PCPs who started at the medical group after 2000 (29.1%, p<0.01) had a scanned ACP document. For patients with POLST documentations (n=7486), patients with a scanned POLST document were also significantly older (80 versus 78, p<0.01). Patients with a diagnosis of cancer (5.4%, p<0.01) and those with PCPs in family medicine (7.3%, p<0.05) had a significantly higher likelihood of having a scanned POLST document. Nonwhite patients (2%, p<0.01) had a significantly lower likelihood of having a scanned POLST document. For patients with ADLWs (n=28,400), those with SDs were significantly older (77 versus 74, p<0.01). Female patients (36.2%, p<0.01); patients with cancer (40.7%, p<0.01); and dementia (48.5%, p<0.01) had a significantly higher likelihood of having an SD. Nonwhite patients (25.3%, p<0.01) and patients with PCPs who started at the medical group after 2000 (29.2%, p<0.01) had a significantly lower likelihood of having as SD.
Multivariable Binary Logistic Generalized Estimating Equations analysis
Table 2 presents the results of the binary logistic generalized estimating equations analyses for patients with any type of ACP documentation, patients with POLST documentation, and patients with ADLWs. The following patient characteristics were significantly associated with higher odds of having a scanned ACP document: being older (OR=1.0, p<0.01); being female (OR=1.1, p<0.01); diagnosis of dementia (OR=1.3, p<0.01); and having cancer (OR=1.2, p<0.01). Nonwhite patients (OR=0.7, p<0.01) and patients with a diagnosis of liver disease (OR=0.8, p<0.05) had lower odds of having an SD. Patients whose PCPs started at the medical group after 2000 were less likely to have a scanned ACP document (OR=0.7, p<0.01).
p<0.05
p<0.01
ACP, advance care planning; ADLW, advance directive/living will; GEE, generalized estimating equations; POLST, physician orders for life-sustaining treatment; SE, standard errors.
Odds Ratios, S.E. in brackets.
The second model examines, for patients with POLST documentation, the probability of having a scanned POLST document. In terms of patient characteristics, being older (OR=1.0, p<0.01) and having a diagnosis of cancer (OR=1.3, p<0.05) were associated with higher odds of having a scanned POLST document. Nonwhite patients (OR=0.8, p<0.05) and patients with PCPs in internal medicine (OR=0.5, p<0.05) were less likely to have a scanned POLST document.
The third model examines the probability of having a scanned ADLW document. Being female (OR=1.1, p<0.01); older (OR=1.0, p<0.01); and having a diagnosis of dementia (OR=1.4, p<0.01) or cancer (OR=1.2, p<0.01) were all associated with higher odds of having an SD. Being nonwhite (OR=0.7, p<0.01) and having a PCP who started at the medical group after 2000 (OR=0.60, p<0.01) were associated with lower odds of having an SD.
Discussion
We have uncovered three gaps in the current practice related to the placement of ACP documentations in EpicCare EHR. First, there is a lack of a standardized location for ACP decisions. Because documentation created in the outpatient setting can be viewed in the inpatient setting by hospitalists (hospital-based physicians) using EpicCare, having standardized locations will facilitate easy retrieval of such documentations in the inpatient setting. For ER or ICU doctors, decisions are made with limited time. An “accident of timing” could lead to ER or ICU doctors to not respect the patient's wishes, if the ACP decision was not easy to find at the point of care.
The second issue is the placement of information related to ACP discussions in the PN that are not properly signed. Even if a physician puts forth the effort to search for decisions in the PN, ACP documentations without proper signatures are not legally valid. Although the “.polst” dot phrase has the means for electronic signatures, in most cases signatures were not filled in. The placement of POLST information in the PN could be due to the lack of physician training about POLST, as POLST came into law relatively recently in California (2009). More education is needed to enable physicians to properly complete POLST so that it can accomplish its intended purpose.
Thirdly, we noted a discrepancy between the number of ACP decisions reflected on the PL and the number of SDs that should correspond to those decisions. At present, organizational policy for AHCD and POLST recommends that patients keep the original form and that physicians add a diagnosis code to the PL and send a copy of the form to the medical records department to scan and place it in the EHR. Scanning currently occurs in batch mode. We have been told that the lag time can be quite significant. A more streamlined process in which the document is placed in the EHR at the time of completion would be more efficient. Another possible explanation for the discrepancy might be the physician's lack of awareness that both patients and physicians should have legally valid copies of the documentation and of the organization's recommended workflow for AHCD and POLST. Currently, the workflow is not uniform among physicians.
Finally, the results point to variation by patient age, gender, and race in having a scanned ACP document. While older age and female gender were associated with higher odds of having an SD, being a minority was associated with lower odds. Specific attention is needed to reduce these disparities.
Limitations and future directions
This study has a number of limitations. First, it was conducted on a single medical group that uses one type of EHR (EpicCare). EpicCare users have different versions and customizations of the software. For example, one organization has a POLST header on the EpicCare snapshot screen highlighted in pink when a POLST has been completed. Another organization also has a POLST section on the EpicCare snapshot screen. Therefore, the results of this study cannot be generalized to other types of EHRs or to other EpicCare users.
Second, POLST is also intended for Emergency Medical Technicians and ER doctors who may not have access to the patient's EHR. It is also important that the patient has the document. Patients should display them in places easily seen, such as on the back of the front door. It is beyond the scope of this study, however, to examine whether patients with POLST documentations in the EHR actually display these forms visibly at home.
Third, we did not ascertain that all of the scanned documents were actually officially signed ACP documents. On a few occasions we have seen scanned documents to be queries regarding ACP, rather than the official ACP document. The findings from this study might have overestimated the number of documentations that are officially signed ACP documents. Future effort should examine whether the necessary signatures have been obtained for these documents.
Fourth, the proportion of patients with references to ACP in the PN is high and is subject to overestimation, because the nature of these discussions, such as whether the patient declined ACP or whether there was a decision, is unknown. For example, a phrase such as “Patient not interested in POLST” would be picked up by this search as a documentation. Future efforts should strive for more precision in the measurement.
Finally, it is possible that some documentation may have been overlooked based on our study search terms.
Implications for practice
If a firm produces 66.5% (all ACP documents) to 95.8% (POLST) of its products in a state that cannot be used by its intended customers, the firm would need to undergo major changes in its production system. In the age of the lean production approach, standardization is a fundamental prerequisite for efficient production and effective delivery of services. Standardizing the location of ACP documentation is paramount to ensuring that patients' wishes are honored.
The most recent EpicCare build (effective October 2010) has a new feature designed to easily locate ACP scanned documents. A button for “Advance Directive/Code Status” was added to the default screen; when physicians click on it they see all the ACP SDs. This is a major step towards facilitating easier recognition of ACP decisions. The large number of SDs, however, can still be a barrier to retrieval of the most salient documents by busy ER or ICU physicians. Rather than a simple repository of SDs, EHR systems need to present a single ACP document (or a small number of these documents) that is most up to date at the moment when critical decisions are made that either honor the patient's wishes, or not.
Footnotes
Acknowledgments
We are grateful to Lubna Qureshi and Nidhi Kohli for extracting EHR data, Lisa Diamond, Hal Luft, and Ashley Stone for helpful comments. Funding from the Metta Fund is much appreciated.
Author Disclosure Statement
No competing financial interests exist.