
Abstract
Abstract
Background:
Palliative care clinicians confront suffering as they care for people living with life-limiting conditions. When the degree of suffering becomes unjustified, moral distress can ensue. Promising work from neuroscience and social psychology has yet to be applied to clinical practice.
Objective:
Our objective was to expand a social psychology model focusing on empathy and compassion in response to suffering to include an ethical dimension and to examine how the interrelationships of its proposed components can assist clinicians in understanding their responses to morally distressing situations.
Analysis:
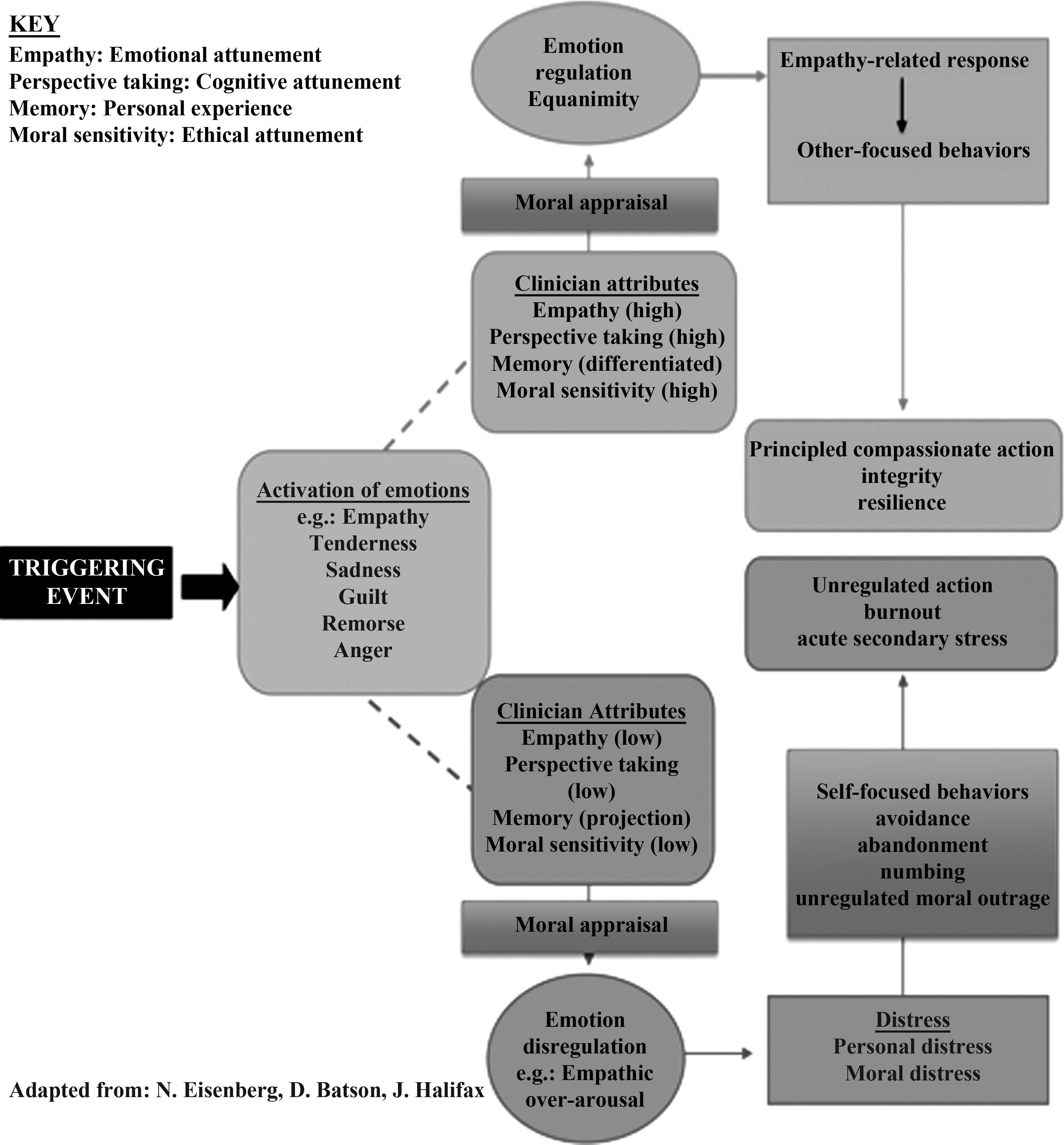
In the clinical context, responses to distressing events are thought to include four dimensions: empathy (emotional attunement), perspective taking (cognitive attunement), memory (personal experience), and moral sensitivity (ethical attunement). These dynamically intertwined dimensions create the preconditions for how clinicians respond to a triggering event instigated by an ethical conflict or dilemma. We postulate that if the four dimensions are highly aligned, the intensity and valence of emotional arousal will influence ethical appraisal and discernment by engaging a robust view of the ethical issues, conflicts, and possible solutions and cultivating compassionate action and resilience. In contrast, if they are not, ethical appraisal and discernment will be deficient, creating emotional disregulation and potentially leading to personal and moral distress, self-focused behaviors, unregulated moral outrage, burnout, and secondary stress.
Conclusion:
The adaptation and expansion of a conceptual framework offers a promising approach to designing interventions that help clinicians mitigate the detrimental consequences of unregulated moral distress and to build the resilience necessary to sustain themselves in clinical service.
Introduction
Moral distress is defined as “the pain or anguish affecting the mind, body or relationships in response to a situation in which the person is aware of a moral problem, acknowledges moral responsibility, and makes a moral judgment about the correct action; yet, as a result of real or perceived constraints, participates in perceived moral wrongdoing.” 7
Through research and anecdotal reports, moral distress is a reality of clinical practice. The complexity of clinical care, combined with clinicians who are often stressed, create an environment where moral distress flourishes and therefore is unlikely to be eradicated. We must consider how to work with the suffering of caregivers in ways that support patients, families, clinicians, and institutions to provide care with the highest level of integrity, dignity, and respect.
Methods for dealing with moral distress have focused primarily on developing skills in moral reasoning, communication, and conflict resolution; interdisciplinary collaboration; system reforms; mediation; ethics consultation; grief counseling; and employee assistance programs.8,9 A promising body of work that has not been applied to instances of moral distress involves neuroscience and social psychology research on empathy, compassion, and empathic distress. This article expands a model developed in social psychology to include an ethical dimension and suggests how the interrelationships of proposed components can assist clinicians to understand their responses to morally distressing situations.
Empathy, Sympathy, and Compassion
The act of caring for seriously ill or dying people demands empathy, sympathy, and compassion, three closely related responses. Empathy “denotes an affective response to the directly perceived, imagined, or inferred feeling state of another being.” 10 It occurs when one perceives or imagines another's affect, triggering a response that fully or partially mirrors the other's affect. Empathy also involves self-awareness and the ability to distinguish self from other, distinguishing empathy from mere emotional contagion.11–13 In contrast, sympathy 10 refers to a genuine concern for another's welfare or situation conveyed by a recognition or understanding of the circumstances or feelings (“I'm sorry for your loss”). It is oriented toward the other rather than the self, may be impersonal or personal and involve feelings of pity, sorrow, or anguish. 14 Although empathy and compassion are closely related, compassion is the other-oriented “emotion one experiences when feeling concern for another's suffering and desiring to enhance that person's welfare.” 15 Compassion optimally involves a quality of presence that conveys stability and resilience, with a balanced concern and heartfelt connection, but is not depleting or overwhelming to either person. 16 It reflects the individual's character through a virtuous concern for the welfare of others and conveys an “inherent regard and respect” for another. 17 These three responses, although admittedly conceptually related, are integral for understanding the experience of moral distress, as moral distress may undermine empathy, cause personal distress, and lead to moral outrage, burnout, or acute secondary stress. 18
The interface between moral distress, empathy, compassion, and personal distress
An expanding body of research is evolving within neuroscience and social psychology focusing on empathy and compassion in response to suffering. 19 A fruitful area of exploration involves how clinicians respond to the distress and suffering of others, a crucial aspect of palliative care. Taken further, these research findings can help clinicians to recognize and respond to their own sources of distress and the influence of them on the way they respond to the suffering of others.
Batson20,21 suggests that two different emotions motivate people to help others: empathic concern and personal distress. Empathic concern, an other-focused emotion, occurs when witnessing another's suffering. Typically it involves feelings such as empathy, compassion, and tenderness. Personal distress can also motivate a person to help in relieving another's suffering. However, it is focused on the self and is prompted by the need to relieve one's own uncomfortable feelings. 22 This can lead to behaviors motivated by a desire to protect oneself from negative emotional arousal that occurs with self-focus when observing another who is suffering.22,23
Eisenberg24,25 elaborated further on Batson's concepts. She proposed that the preconditions for “empathic arousal” that can precipitate either positive or aversive responses include empathy (emotional attunement), perspective taking (cognitive attunement), and memory (related to personal experience). Seeing another in pain, for example, gives rise to emotional arousal, reflected in activation within emotion-related brain areas, such as the anterior insula, anterior cingulate, and amygdala.22,26 When arousal in response to another's suffering is not regulated, it can give rise to personal distress, 24 thereby undermining the possibility for expressing compassion, 25 leading to either avoidance or self-focused behaviors.
Self-focused behaviors are those that involve relieving one's own uncomfortable feelings in response to the suffering of another. Eisenberg notes that compassion and personal distress appear to be related to individual differences in self-regulatory capacities. 25 Brain systems involved in emotion regulation are typically activated when compassion for social or physical pain is elicited, 27 and when this emotional arousal is not regulated, it can lead to “empathic over-arousal.”24,28 Responses such as generalized discomfort, concern about one's own welfare, anxiety, agitation, autonomic arousal, intense sadness, and (sometimes) anger signal empathic over-arousal. 29
A Framework for Understanding Moral Distress
Batson's 20 model and Eisenberg's elaboration24,25 provide a useful framework for identifying new ways of responding to the situations that cause moral distress among clinicians. We extend their prior work to include the ethical dimensions of responses to distressing events that involve conflicting moral values, commitments, or perspectives. In addition to emotional attunement (empathy), cognitive attunement (perspective taking), and personal experience or memory, responses to morally distressing events also include moral sensitivity, discussed below. We propose that these interrelated and dynamically intertwined factors create the preconditions for how one responds to a triggering event instigated by a perceived ethical conflict or dilemma. The critical interplay of the practice environment in contributing to or modulating the impact of individual responses to moral distress is beyond the scope of this paper.
Moral sensitivity
Responding to clinically challenging cases requires ethical awareness, sensitivity, and attunement as antecedents for discernment and action. 30 Moral sensitivity is the “ability to recognize the presence of moral issues in real-world situations.” 31 Specifically, it involves the ability to (1) discern the morally salient dimensions of the situation; 32 (2) perceive and interpret the perspectives, feelings, and responses of others; and (3) discern how one's actions may affect self and others. 34 It requires sufficient tolerance of ambiguity to simultaneously evaluate the possible impact of various actions from multiple perspectives. This interpretive awareness may reveal the need to take moral action and activate the cognitive processes for moral reasoning. Illuminating the moral contours of specific situations—the attitudes, values, and moral commitments of all those involved—invites more nuanced moral analysis, a cognitive process that can impact the range of factors and choices considered, and the actions selected and implemented.
Clinicians in whom moral sensitivity is not well developed may fail to recognize an occasion for moral action, or tolerate morally objectionable acts. 34 Ambiguity gives rise to apathy or confusion. Overlooking the negative impact of certain behaviors on patients, families, and others may lead to inappropriate acts that undermine integrity.
We postulate that moral sensitivity (ethical attunement) coexists with empathy (emotional attunement), perspective taking (cognitive attunement), and memory (personal experience) to create the conditions on which arousal and regulation depend. Conceptually, moral sensitivity is related to conscience, that aspect of oneself that evaluates one's own actions. Once activated via the autonomic nervous system and conscious or unconscious memory, conscience assesses a situation and engenders emotions in response. 35 When moral values, internalized norms, or commitments are aligned, wholeness is preserved and feelings such as contentment, honor, or self-respect arise; ethical values are embodied in each interaction and lead to integrity, preserving moral action. In contrast, when a situation presents conflicting moral demands with no clear path to resolution, moral values are compromised and feelings of remorse, guilt, self-disgust, humiliation, or regret may occur, instigating self-focused actions aimed at relieving personal and/or moral distress.
Eisenberg 29 postulates that individuals who are exposed repeatedly to negative emotional arousal are vulnerable to experiencing personal distress. This suggests that clinicians who experience secondary or vicarious trauma as a result of their constant exposures to suffering and tragedy are at higher risk for personal distress; 36 and arguably, moral distress is intensified when they are repeatedly exposed to morally distressing situations. Similarly, if their personal distress arises from an ethical dilemma and is unrelieved, moral outrage can ensue.37–39 We postulate that the culmination of unrelieved moral or personal distress can be unregulated action, burnout, or acute secondary stress.
Emotional arousal and regulation
Arousal involving ethical quandaries may arise because of a perception of value conflicts, confusion about the proper course of action, uncertainty about which course of action to pursue, or a real or perceived inability to do the “right” thing. This may be coupled with witnessing the suffering of another, attempting to relieve another's suffering, or arousal of empathic concern. 4 Conceivably, when clinicians become aroused by a distressing event, various positive emotions can be aroused, such as empathy or positive regard, or negative emotions such as sadness, guilt, remorse, frustration, or anger. For example, witnessing the unrelieved pain and suffering of a dying patient may instigate empathy, advocacy, and action to secure the therapies needed for relief in order to uphold the principle of “do no harm.” Likewise, emotional triggers associated with perceived inappropriate or burdensome use of technology can lead to requests for ethics consultation in response to an initial arousal precipitated by value conflicts. 40 Once aroused, the response and degree of emotional regulation will likely be informed by the degree of emotional, cognitive, and ethical attunement and personal experience or memory. Of particular importance in the context of ethical dilemmas is the cumulative “crescendo” effect of unresolved experiences of moral distress 34 and the possibility that these memories may exacerbate the distress.
We propose that when feelings in response to the distress (both related to the ethical conflict and one's ability to take the correct ethical action) are modulated through mindful awareness, the emotional connection to the patient and their predicament contribute to one's ethical attunement to the situation and can instigate the moral motivation to uphold the violated ethical value, principle, or standard and align integrity. According to Batson's model, if arousal is regulated and self and other are distinguished, then the aroused state can give rise to compassion, with the manifestation of other-focused behaviors such as altruism and principled compassionate action that preserves integrity and supports resilience. Eisenberg 25 proposes that individuals who can regulate their emotions and behavior are more likely to express compassion than are less regulated individuals. Without emotion regulation and processes by which self and other are differentiated, moving from empathy to compassion is unlikely. 25
When the aroused state is not regulated through mindful appraisal that gives rise to a response of compassion (sympathy is the term used by Eisenberg), because the experience of another's suffering becomes unbearable and unregulated, personal distress or in the case of ethical concerns, moral distress, can occur. 41 If clinicians are unable to regulate their emotions or responses as a result of negative empathic arousal that exceeds their capacity to maintain neutrality and composure, it can lead to an experience of aversion and to three predictable responses: (1) avoidance and/or abandonment of the patient and family physically, emotionally, or spiritually (flight); or (2) angry or contentious responses that lead to self-focused behaviors aimed at mitigating the caregiver's own suffering 42 (fight); or (3) “freeze” or numbing, 43 a generalized shutting down emotionally and being immobilized to respond or take appropriate action to address the situation. 38 We postulate that these responses to other sources of distress also occur in response to moral distress.
Ethical appraisal, discernment, and action
Concurrently, the perceived violation of an ethical value, principle, or standard that accompanies an ethical dilemma may ignite moral emotions or feelings of discomfort, anxiety, confusion, dissonance, uncertainty, or anger and other automatic and deliberative processes that underlie ethical behavior. This could instigate a cognitive process of ethical appraisal, discernment, and reasoning, as one determines the ethically justified response. Discernment is primed by moral sensitivity to the ethically salient dimensions of self, others, and the situation, and to the ethical reasons that support various courses of action. 34 Once recognized as a situation where action is needed, cognitive processes aimed at understanding the conflicting perspectives, exploring the nature of the value conflicts, identifying the range of ethically permissible actions, and determining the best course of action (all things considered) are activated. This iterative process involves an appraisal of how one's actions affect self and others and how the actions taken or not taken promote or undermine integrity and/or result in participation in wrongdoing. 44 The preconditions, described above, support or undermine a person's capacity to respond in an emotionally balanced, ethically grounded, and compassionate manner 33 (see Figure 1).
Consequences of clinician distress
When clinicians experience personal or moral distress that cannot be modulated, the consequences may include moral harm or outrage, burnout, or acute secondary stress. Moral outrage has been described as anger provoked by a perceived violation of an ethical standard such as fairness, respect, or beneficence. 41 Pike 45 describes moral outrage as “characterized by energy-draining frustration, anger, disgust, and powerlessness.” Burnout, in contrast, is “a state of physical, emotional, mental exhaustion caused by long-term involvement in emotionally demanding situations.” 46 Burnout tends to emerge gradually as a result of emotional exhaustion and job stress producing symptoms ranging from mild short-term disturbances, to gradually more-recalcitrant disturbances that can become chronic. In contrast, secondary stress occurs in response to the pressures that are placed on clinicians who care for others in need. 18 Acute secondary stress (sometimes referred to as vicarious trauma) occurs in response to repeated exposure or re-exposure to suffering and trauma that creates helplessness, confusion, or frustration in response to one's inability to relieve the suffering or relate to it in ways that are not draining or exhausting and thereby compromise the person's well-being. 18
In contrast, if mental and emotional stability are maintained and distress modulated, the appraisal and discernment process can yield principled compassionate action: an adherence to the highest ethical standards while grounded in a robust process of compassion. In this sense compassion is a rigorous, balanced stance of a “strong back” of equanimity that allows one to be clear, courageous, and principled in the midst of the most challenging circumstances with the soft front of open-heartedness, kindness, and empathy leading to compassion. 16 Principled compassion is founded on an unwavering commitment to integrity. It does not imply apathy, disregard, or indifference to egregious situations. A hallmark of principled compassionate action includes leveraging one's moral outrage by executing unpopular decisions and when appropriate, conscientiously objecting to ethically compromising situations, despite resistance, in a fair, modulated manner. 47
Ideally, the outcome of being able to modulate moral distress is a state of equilibrium, integrity, and resilience. Resilience, the ability to return to a restorative limit of function in the midst of challenging circumstances, relies upon focused awareness and modulation of somatic, emotional, spiritual, and moral stimuli within a zone of stability and well-being. Resilience suggests that although the frequency of ethically problematic events may not change, the intensity of morally distressing situations may not result in detrimental consequences.
Discussion
For the purposes of illustration, we postulate (see Figure 1) that if empathy, perspective taking, memory, and moral sensitivity are highly aligned, the intensity and valence of the emotional arousal will influence the ethical appraisal and discernment of the situation by engaging a robust view of the ethical issues, conflicts, and possible solutions. The confluence of these factors helps to focus attention on the ethically salient features of the situation; supports the synthesis of multiple perspectives; and facilitates the conceptual analysis of the competing claims and obligations that, when combined with emotional regulation and equanimity, is more likely to produce empathy-related responses (compassion) and other-focused behaviors leading to principled compassionate action, integrity, and ultimately greater resilience. In contrast, if empathy, perspective taking, memory, and moral sensitivity are not aligned, we postulate that ethical appraisal and discernment are deficient (because moral sensitivity is not well honed); creating emotional disregulation (particularly empathic over-arousal); and potentially leading to personal and moral distress and ultimately self-focused behaviors, including avoidance, abandonment, and/or numbing; or resulting in unregulated moral outrage, burnout, or acute secondary stress. Ultimately, this state of disregulation potentially undermines the ethical reasoning process. Without modulated moral sensitivity, salient features of the situation may be overlooked, overemphasized, or disregarded; ethical actions are then more likely to be guided by unconscious projections, unreflected assumptions, and faulty reasoning leading to actions that lack sufficient ethical justification or are unethical. Whether the relationships reflected in the proposed framework are valid will require systematic empirical evaluation and study. Although presented here as a linear sequential path, we postulate that the elements are interrelated and occur in a dynamic, iterative spiral.
Conclusion
Moral distress is an unavoidable reality of palliative care practice. Clinicians who experience it repeatedly need new ways to understand their experiences and to find alternatives for addressing it. The adaptation and expansion of a framework grounded in neuroscience and social psychology offers a promising approach to designing interventions that mitigate the detrimental consequences of unregulated moral distress and that build resilience. Research is needed to test the framework's efficacy and to document the impact on individual clinicians and ultimately the care that is provided to patients and families.
Footnotes
Acknowledgments
The authors acknowledge their colleagues of the Being With Dying professional training for their invaluable contribution to the development of this model and the various researchers, cited in this paper, whose work has inspired us. Gratitude to Chery Kay Zogg and Kelly Wilson-Fowler for assistance with manuscript preparation.
Author Disclosure Statement
No competing financial interests exist.