
Abstract
Abstract
Background:
There are very few reports about end-stage renal disease (ESRD) patients with breast pains in the medical literature, posing a difficulty to understand their pathophysiology.
Case Presentation:
A 47-year-old African American female patient with ESRD on hemodialysis presented to the pain clinic with new-onset black maculopapular skin lesions on her breasts. These lesions started out as dark spots and then became necrosed, exposing the underlying tissue. The painful and tender lesions were located in a circumferential pattern around the bases of both breasts. She had stopped using breast supporting undergarments secondary to allodynia-hyperalgesia eliciting from necrotizing skin tissues. Her recent skin biopsy was inconclusive about ruling in or out the possibility of calciphylaxis. However, her past mammograms had showed calcium deposits in her breasts. Her other past medical history was significant for chronic hypotension with recently diagnosed legal blindness bilaterally. Her home medications included midodrine. The systolic blood pressures in either arm were consistently recorded in high 60s to low 70s during the interdialytic periods. She had multiple emergency room admissions secondary to persistent chronic hypotension; however the underlying pathophysiology for intractable but asymptomatic hypotension remained obscure. Over the course of the next 11 months her nonhealing breast lesions progressed and became infected. She developed septic shock due to infected lesions. Per her do-not-resuscitate requests, she died peacefully while under inhospital hospice care.
Conclusion:
Morbidity-mortality with calciphylaxis and chronic hypotension related tissue changes is high, and the breast lesions in ESRD patients require aggressive treatment for underlying inadequate oxygen delivery to these peripheral tissues.
Introduction
Case Presentation
A 47-year-old African American female patient with ESRD on hemodialysis presented to the pain clinic for follow-up of cervical spondylosis and lumbar radiculopathy. At the follow-up presentation she also complained of new-onset black maculopapular skin lesions on her breasts. According to the patient, these lesions started out as dark spots and then became necrosed, exposing the underlying tissue. The lesions were located in a circumferential pattern around the bases of both breasts. These lesions were painful and tender, with pain scores of 10/10. She had stopped using breast supporting undergarments secondary to allodynia-hyperalgesia eliciting from necrotizing skin tissues. A punch excision skin biopsy had been done at her dermatologist's clinic; it had revealed the histopathological features most consistent with chronic dermatitis. The skin biopsy did not exclude the clinical presentation of lichen simplex chronicus; it was also inconclusive about ruling in or out the possibility of calciphylaxis. However, her past mammograms had shown calcium deposits in her breasts. Her other past medical history was significant for chronic hypotension with recently diagnosed legal blindness bilaterally. Her home medications included midodrine. The systolic blood pressures in either arm were consistently recorded in high 60s to low 70s during the interdialytic periods. She had multiple emergency room admissions secondary to persistent chronic hypotension; however the underlying pathophysiology for intractable but asymptomatic hypotension remained obscure. She was maintained on amitriptyline 50 mg with gabapentin 100 mg before sleep and hydrocodone 10 mg with acetaminophen 500 mg every six hours as needed for pain. Over the course of the next 11 months her nonhealing breast lesions progressed and became infected. Septic shock ensued and she was admitted to the intensive care unit. Her management included vasopressors and broad spectrum antibiotics. However, she, in consent with her family, refused all further curative care and was transferred to hospice care. She died peacefully while under inhospital hospice care.
Discussion
Though the pathophysiology of our patient's breast lesions was enigmatic, it was our understanding that these lesions can be best explained by the skin tissue changes secondary to calciphylaxis with chronic hypotension. Calciphylaxis is a rare condition that affects CKD patients with an incidence of about 5% and mortality of around 80% even with treatment.2,3 It can occur as early as 6 months or even after 15 years of hemodialysis in CKD patients.4,5 It has a female preponderance. 6 The various factors that interplay to promote a favorable microenvironment in the tissues for calcium deposition are corticosteroid administration in CKD patients on dialysis, 7 albumin infusion, immunosuppressants, trauma, infection (especially human immunodeficiency virus), 8 low protein S functional level, 9 metallic salts, intramuscular nondextran complex, calcium heparinate, and intramuscular tobramycin injections.4,5,7–9 Risk factors for calciphylaxis are obesity, diabetes mellitus, white ethnicity, time of renal replacement therapy, and coumarin anticoagulants.10–12 Factors associated with calciphylaxis are vitamin D analogs, calcium containing phosphate binders, iron supplementation therapy, and glucocorticosteroids.10–12 Besides calciphylaxis, other differential diagnoses for breast necrosis are acute bacterial breast infections, breast cancer, warfarin induced skin necrosis, cutaneous vacuities, and hypercoagulable states like protein C and protein S deficiency. 13
Calciphylaxis clinically presents as a painful nonhealing skin ulcer, which progresses rapidly to sepsis leading to a significant morbidity and mortality. Calciphylaxis occurs predominantly in areas with a large amount of fat, like abdomen, buttocks, and thighs. It has an insidious onset as livedo-reticularis-like skin lesions, which over a period of days to weeks transform into painful, subcutaneous, purpuric plaques and nodules and subsequently become necrotic ulcers covered by eschars. 10 Onset of calciphylaxis is usually related to a history of recent trauma, the initiation of coumarin treatment, or hypotensive episodes.10,12 There is high mortality associated with calciphylaxis because of secondary sepsis of the cutaneous gangrenous ulcers. 14 The best imaging to study soft tissue calcification is xerography, a high-definition x-ray photography that tends to improve structural visibility. 15 Xerography (x-ray technique used in mammography) is the imaging modality of choice that reveals small-vessel calcification; and low transcutaneous oxygen saturation can confirm underlying tissue ischemia.16,17 The majority of calciphylaxis patients show a positive bone scan, which can be used to assess response to treatment. 13 Skin biopsy itself can lead to development of nonhealing ulcers, therefore it should be done only in equivocal cases. 13 Histologically, it shows medial calcification and intimal hypertrophy and microthrombi leading to complete occlusion of vascular lumen of the small and medium sized vessels within the dermis and subcutaneous tissue. 18
The main therapy for calciphylaxis is to prevent infections with intensive wound care and systemic antibiotics; to ensure adequate analgesia with opioid analgesics; and to slow the disease progression by modifying elevated calcium-phosphate product and/or parathyroid hormone (PTH) level using low-calcium dialysate for intensified dialysis and noncalcium-based phosphate binders, and discontinuing vitamin D analogs. Medical therapy includes cinacalcet, a calcimimetic approved for the treatment of patients with secondary hyperparathyroidism and CKD.14,19–21 Urgent parathyroidectomy might be necessary if there is elevated parathyroid hormone level.22,23 Sodium thiosulfate reduces metastatic tissue calcification, acts as an antioxidant, and induces endothelial nitric oxide synthesis, which improves blood flow and tissue oxygenation leading to ulcer healing.24,25 Bisphosphonates, both oral and intravenous, can cause rapid reduction in pain and decreased signs of inflammation.26–28 Hyperbaric oxygen therapy has been reported to promote wound healing by improving oxygen delivery to damaged tissues. 29
In regards to coexistent chronic hypotension that worsens the prognosis of calciphylaxis, 30 there are various mechanisms for pathogenesis of chronic hypotension in the interdialytic periods of ESRD patients: cardiac dysfunction, 31 enhanced production of vasodilators like adrenomedullin or nitric oxide induced by long-term hemodialysis,32–34 and autonomic nervous system dysfunction and decreased reactivity of blood vessels to noradrenaline and angiotensin II. 35 The vascular system of chronic hypotensive patients on dialysis has a postsynaptic resistance to stimuli from the sympathetic nervous system due to down-regulation of alpha-2-adrenergic receptors.35,36
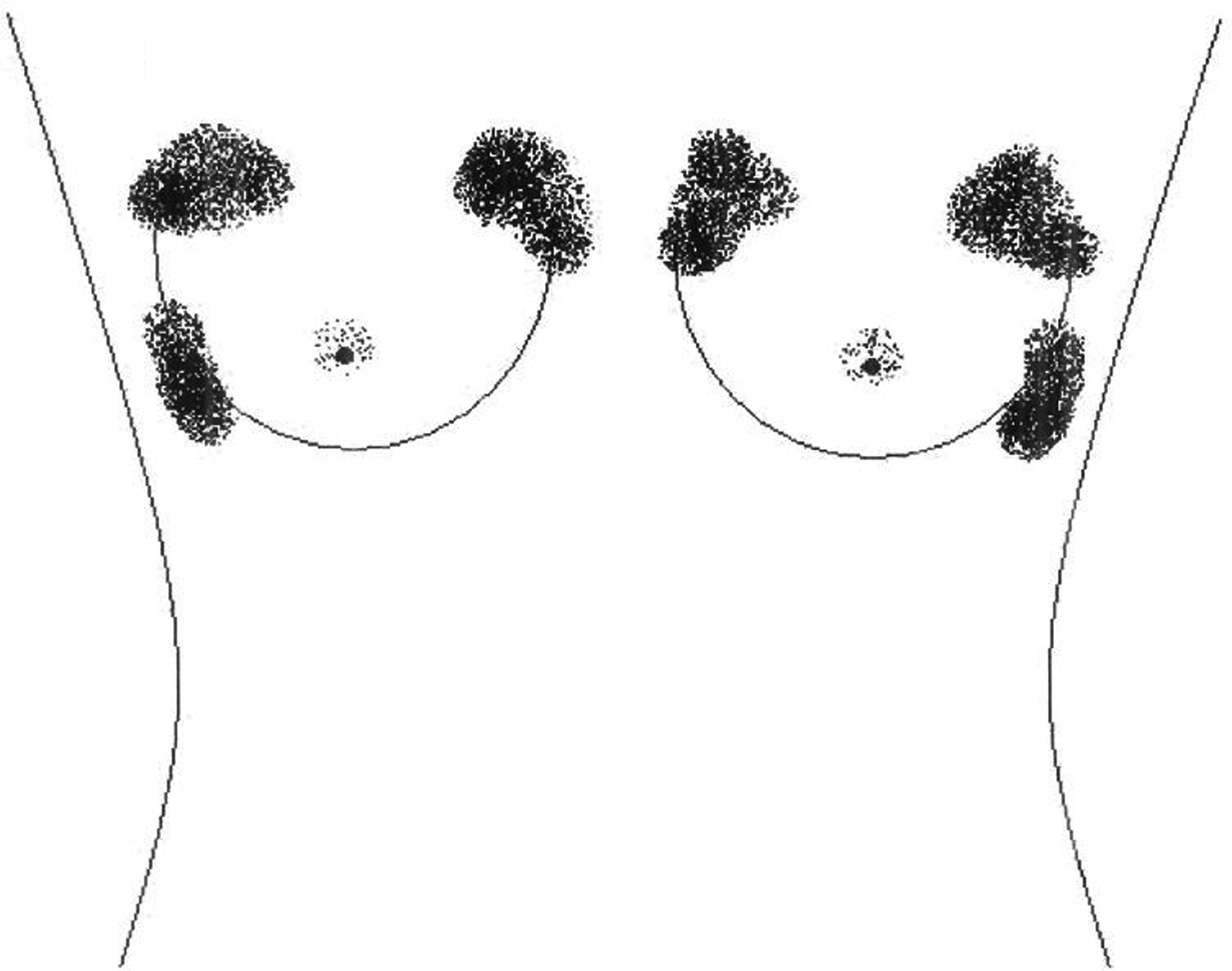
In our ESRD patient, the histopathology of a limited skin segment biopsy revealed no obvious calciphylaxis; however the mammograms had shown calcifications in her breast tissue suggesting calciphylaxis in our ESRD patient. Though our patient was asymptomatic and living with extremely low systolic blood pressures (high 60s to low 70s) in interdialytic periods, the nonhealing breast ulcers and legal blindness suggested chronic hypotension induced end-organ damage. Her breast skin tissue changes in our patient were secondary to combined effects of xerography-suggestive calciphylaxis with chronic hypotension induced regional tissue hypoperfusion-hypoxia. As these changes were primarily localized circumferentially in the nondependent areas of the breasts, the wound healing might have been worsened by the nondependent breast skin exposed to constant wear-shear tension and weight of the unsupported breasts (see Figure 1). Though she was not able to tolerate breast support undergarments due to pain, it might have been worth investigating whether customized undergarments that support breasts without coming in contact with hyperalgesic areas would have promoted wound healing. The circumferential pattern of breast lesions provides weight to the explanation that constantly unsupported breasts in our pain patient might have exposed potential watershed areas in her breast skin to wear-shear injury; calciphylaxis with chronic hypotension would have further deteriorated the pathological conditions in these areas by interfering with adequate oxygen delivery.
In summary, morbidity and mortality with calciphylaxis and chronic hypotension related tissue changes is high and the breast lesions in ESRD patients require aggressive treatment for underlying inadequate oxygen delivery to these peripheral tissues. Monitoring with transcutaneous oxygen saturation of breasts' nondependent areas (watershed regions) and nonpharmacological management with customized breast support undergarments may be worth considering in these intractable pain patients who all eventually require palliative and hospice care.
Author Disclosure Statement
No competing financial interests exist.