
Abstract
Abstract
The purpose of this study was to evaluate the prognostic value of the Palliative Performance Scale (PPSv2) in the palliative care unit of our hospital, which sees more than 1500 referrals a year (both inpatient and outpatient).
We evaluated 356 admission episodes into our department, focusing mainly on patients with advanced cancer. The PPS has been shown to be useful in prognostication and this study confirms this in a fairly large study population in a tertiary care, teaching hospital. We further evaluated the impact of certain biologic variables in survival length, and eventually looked at variables significant for survival at 90 days, developing a prognostic model incorporating these variables.
We believe that the study results will aid health care professionals in assessing survival length of their patients more accurately, thus helping to guide decisions for treatment and care in a more judicious manner. It will also allow us to choose patients most likely to benefit from hospice resources.
Introduction
Prognostication is widely acknowledged to be an inexact science, a skill influenced by both subjective and objective measures. Subjective measures can include clinical prediction of survival (CPS) or interpretation of symptom intensity. Objective measures may include the use of biochemical variables, some of which have been shown to help predict mortality. 2
Different prognostic tools and indices have been developed and studied across various care settings, all with the aim to refine prognostic accuracy. An important harbinger of mortality is the presence of functional decline, and this has been borne out in studies that have shown the relationship between a poor performance status and mortality. Other independent predictors of survival include anorexia, dysphagia, and cognitive failure. 3 These variables are represented in the Palliative Performance Scale (PPSv2), a modification of the Karnofsky Performance Scale that encompasses five observer-rated domains. Developed in 1996, 4 it has been found to correlate well with length of survival in the tertiary care setting, as well as in the hospice setting.5,6 The PPS not only examines the degree of functional independence and disease burden, but it also has domains of self-care, oral intake, and level of consciousness, the temporal change of which may reflect physiological response to disease progression. Divided into percentile categories from 0% to 100%, it represents a spectrum of independence from full functionality at 100% to full dependence with minimal oral intake at 10%, and death at 0%. The PPS has proven correlation with survival, at grouped percentile categories, as well as at each tenth percentile category.7–9 The primary objective of our study was to evaluate prospectively, the prognostic value of the PPS in the prediction of survival in patients suffering from advanced cancer in a tertiary care hospital. The secondary objective of the study was to evaluate the impact of clinical variables commonly measured during admission on the length of survival.
Methods
Data collection
This was a prospective cohort study of patients suffering from advanced cancer admitted to the Palliative Care Unit of Tan Tock Seng Hospital in Singapore. Noncancer diagnoses were excluded. Patient admission episodes were consecutively entered into the study between July 2009 and November 2010 and were followed up to November 2011. The PPS score of each patient was decided in multidisciplinary palliative team discussions and was recorded on admission and on a weekly basis until the patient was discharged from the service or death occurred. Laboratory investigations were not undertaken specifically for this study. However, if they were performed as part of a patient's plan of care, the results were recorded by retrospective review of the medical charts of the patient upon discharge or death. Hence, not all variables selected for inclusion into the study were available for every patient admission episode. Variables entered into the study included age, gender, site of cancer, oncologic treatment within 3 months of admission, and PPS scores. Clinical variables included the lowest hemoglobin, albumin, and platelet values, as well as the highest value of white cells and calcium level during the admission episode. Information about oncologic treatment in the form of palliative chemotherapy or radiotherapy was obtained through retrospective examination of the patient's clinical notes. Length of survival was calculated based on the duration of time from admission to death. Information regarding date of death was obtained through manual examination of records at the hospital, inpatient hospice, or community hospice. The study protocol was reviewed and approved by the ethical review board of the hospital.
Clinical outcome
The primary end point was survival time for each episodic admission. The secondary end point was mortality within 90 days of follow-up. The last evaluation of patient survival status was performed in November 2011. Biologic variables routinely measured in such a care setting were also investigated as to whether they increased the predictive accuracy of the PPS. Models based on the PPS score were then developed using the biologic variables found to be statistically significant to estimate 90 day mortality.
Statistical methods
Stata v.10.1 (Statacorp, College station, TX) was used in the statistical analysis of the results. Hemoglobin, platelet, calcium, albumin, and white cell counts were treated as continuous variables and presented as mean (standard deviation [SD]). Categorical data in the form of PPS grouping, gender, and oncologic treatment within 3 months of admission were presented as an absolute number and percentages. A p value<0.05 was considered statistically significant.
Survival function of each PPS group was estimated using Kaplan-Meier analysis. Analysis of length of survival time based on PPS scores was performed by categorizing patients into three main groups based on degree of dependence in self-care. Patients grouped in PPS/A had scores between 70% and 100% (full ability for self-care), whereas patients in PPS/B had scores between 40% and 60% (occasional to mainly assisted self-care), and PPS/C was represented by patients scoring between 10% and 30% (total care). Survival time of each PPS group was estimated using the Kaplan-Meier survival analysis. Univariate analysis was carried out for variables entered into the study, to determine the demographic and biological variables that predicted survival time. Pearson's χ2 tests were used to explore the relationship between categorical variables and survival. The log-rank test was used to compare survival, based on Kaplan-Meier curves across two or more groups for categorical variables, whereas Cox proportional hazards regression model was used to evaluate continuous variables that predict length of survival. Multivariate Cox proportional hazards were then constructed by entering variables significant in univariate analysis. Hazard ratios with 95% confidence intervals (CIs) are reported. Correlation of survival time with each 10% increment level of PPS was examined using Kaplan-Meier survival analysis, and multivariate Cox proportional hazard analysis conducted to determine independent predictors of survival.
Between groups comparison of baseline data was performed using the independent-samples t test. Pearson χ2 tests were used to explore relationships between categorical variables and mortality. Variables that were significant univariately were added to the same multivariate logistic model to investigate the independent predictors of survival/mortality at 90 days. Odds ratio (OR) with 95% CIs are reported. The discriminatory property of the model at 90 days was evaluated using the area under curve (AUC) of the receiver operating characteristic (ROC) curve.
Results
Three hundred fifty-six consecutive patient admission episodes were entered into the study between July 2009 and November 2010, based on the data of 296 patients. Fifty-three patients had more than one admission to the unit. Table 1 shows the demographic, clinical, and functional characteristics of the study subjects involved.
Patient-centric data (n=296).
Admission episodic data (n=356).
CUP, carcinoma of unknown origin; GI, gastrointestinal; GU, genitourinary; MSK, musculoskeletal.
The mean age of the study subjects was 68.9 years (SD: 13.4), with a fairly equal representation of both male and female patients. Within the admission episodes, patients with admission PPS scores in the percentile range of 40% to 60% (PPS/B) represented the largest group with 199 episodes, whereas the next largest subset was PPS/C (PPS percentile range 10% to 30%), with 140 episodes. For the last recorded PPS value, distribution of PPS scores between groups “A,” “B,” and “C” remained the same, although there was a closer approximation between the number of patients in PPS/B and PPS/C. The mean PPS score at baseline was 39.1%, with a minimal drop in PPS score throughout the admission episode. There was a mean decrease of 4.4% in PPS score from admission to discharge or death in this study group.
Overall, the median survival time for patients in this study was 35 days (range: 14–81days). Kaplan-Meier survival analysis of patients within PPS/A, PPS/B, and PPS/C showed significant difference in the shape of the survival function among all groups. Median survival time was 59 days in PPS/A patients, 43 days in PPS/B patients, and 19 days in PPS/C patients (Fig. 1).

Survival length of three groups of patients stratified by baseline PPS scores. Survival differed significantly among patients in the three groups (p<0.001 by the log-rank test).
In univariate analysis, length of survival was affected by albumin, gender (Fig. 2), and baseline PPS scores. The presence of low albumin levels (hazard ratio [HR]: 0.96; 95% CI: 0.93-0.98), or being male (HR: 1.44; 95% CI: 1.10-1.87) affected length of survival. For every percentile increase in PPS documented from baseline, the HR was 0.97 (95% CI: 0.96-0.98), and for each tenth percentile increase in baseline PPS, the HR was 0.78 (95% CI: 0.72-0.84). The mean value of albumin in the study population was 23.7 g/L, with an HR of 0.96 (95% CI: 0.93-0.98) for every unit increase in albumin level, and an HR of 0.67 with every 10-unit increase (95% CI: 0.56-0.81). Using multivariate Cox proportional hazards analysis, a final model was constructed using significant univariate variables that had potential impact on survival time. The male gender (HR=1.51; 95% CI: 1.19-1.92) was more likely to experience a shorter survival time. However, having a higher albumin value by one unit (HR=0.97; 95% CI: 0.95-0.99) or by 10 units (HR=0.74; 95% CI: 0.60-0.90) was associated with a longer time to mortality. Admission PPS values within PPS/B was associated with a longer time to mortality compared with PPS/C (HR=0.61; 95% CI: 0.47-0.78), whereas those in PPS/A had a longer time to mortality compared with PPS/C (HR=0.46; 95% CI: 0.25-0.85) (Table 2). A significant survival difference was demonstrated between each tenth percentile level of the PPS, with a another separate multivariate model revealing a similar finding of a shorter survival time being associated with a lower PPS level, the male gender, and lower albumin levels (Table 3).

Survival length based on gender, using log-rank test.
Cox proportional hazards regression model adjusts for PPS baseline stratified by PPS/A, PPS/B, and PPS/C, and all other variables in the table.
Cox proportional hazards regression model adjusts for PPS tenth percentiles, and all other variables in the table.
Mean baseline PPS scores for admission episodes among those who died within 90 days (PPS score=37.5; SD=16.0) was lower than those who lived (PPS score=45.1; SD=13.1). Patient admission episodes where the gender was male, albumin values were lower (mean=22.9 g/L; SD=6.27), and white cell counts were higher (mean=13.6; SD=7.40) were more likely to succumb within 90 days (Table 4). Using multivariate logistic analysis, a model was constructed to evaluate the independent predictors of survival at 90 days. Baseline PPS scores together with gender and albumin levels were found to be independently predictive of survival at 90 days. In the 90-day prognostic prediction model, the OR was 0.98 for every unit increase in PPS score, 0.92 for every unit increase in albumin, with an OR of 1.83 for male versus female gender (Table 5). ROC analysis was used to determine the discriminatory value of the model, with the area under the curve at 0.70 (95% CI: 0.63-0.77) (Fig. 3). The prognostic model for 90-day mortality had a positive predictive value (PPV) of 79%.
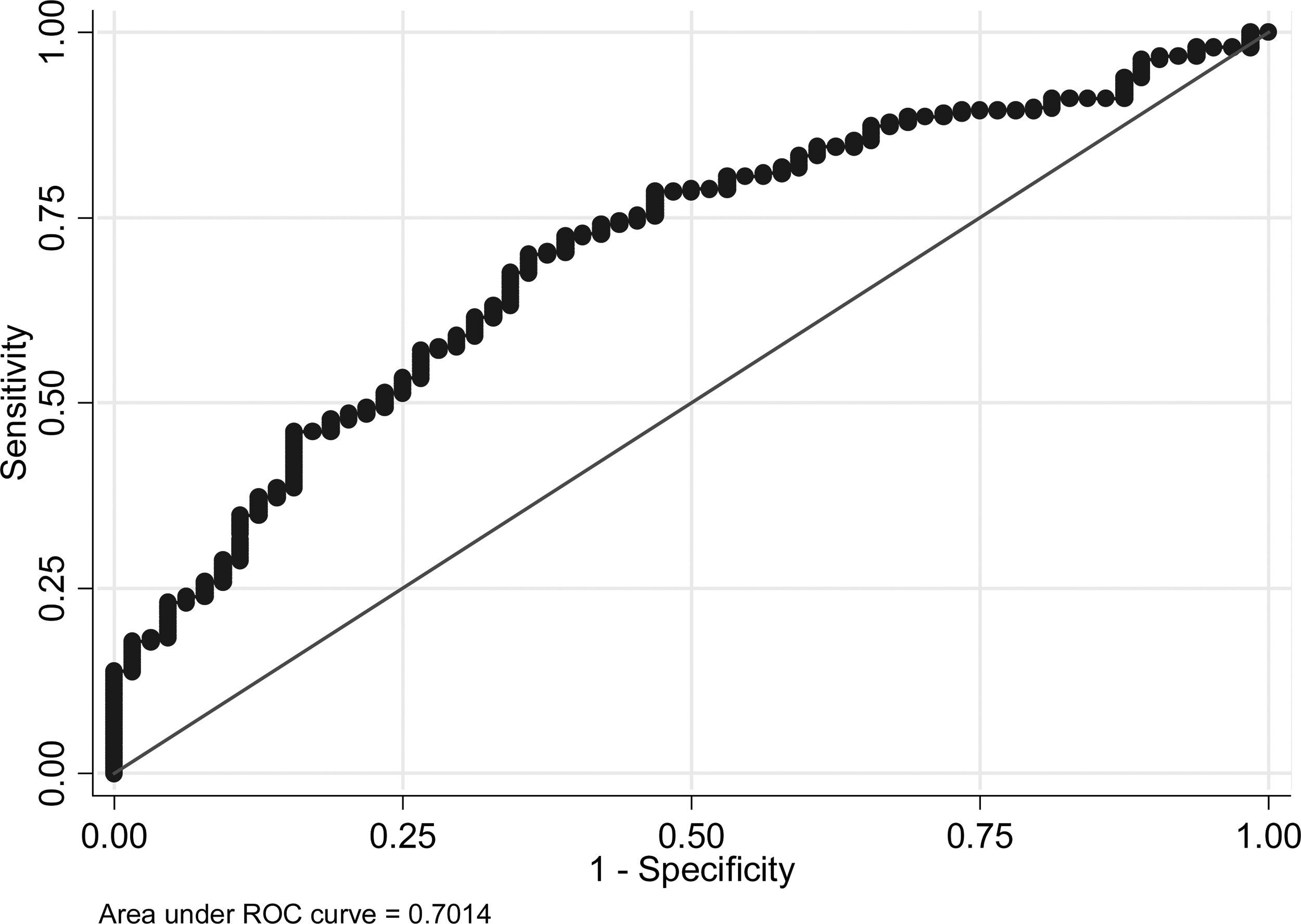
Receiver operating characteristic (ROC) curve for prediction of survival at 90 days using baseline PPS, albumin, white cell count, and gender.
Mean (standard deviation) for continuous variables, percentages for categorical variables. Admission episodic data.
χ2-test.
t test.
Mann-Whitney U test.
Logistic regression model adjusts for all variables in the table.
Discussion
Prognosis is an essential skill for clinicians, involving the evaluation of various objective and subjective measures of a patient's well-being, in order to derive an accurate measure of a patients' length of survival. Its inherent difficulty is at odds with the vital need to provide accurate information to patients and their caregivers, prognosis being an integral component of discussions relating to treatment and care at the end of life.
The PPS has been validated in heterogeneous patient populations across different sites of care for the prediction of survival. It has been used in inpatient hospice 4 and inpatient palliative care units, 10 as well as in the community and nursing home setting.6,11 As in previous reviews,7–9 our study shows a significant difference in survival length for patients across PPS percentile ranges. Patient survival was not only studied at each tenth percentile level of PPS but was further evaluated in three percentile range groups (A: 70%–100%, B: 40%–60%, and C: 10%–30%). This specific grouping of patients was chosen to reflect change in ability to manage one's self-care. The SUPPORT project showed evidence that patients in the last 6 months of life suffer functional decline, with many suffering four or more impairments in activities of daily living (ADL; according to the modified Katz Index) in the last days of their lives. 12 A study comparing the pattern of functional decline in the last year of life in patients with cancer as opposed to patients suffering from terminal end organ illnesses revealed that ADL impairments in cancer patients increased from a mean of 1 to 3 in the last 5 months of life, with an increased percentage unable to get up from a chair or bed. 13 Increasing difficulty with self-care may reflect greater physiological loss due to disease burden and therefore a poorer outcome. In this study, patients who required total care (PPS/C) at baseline assessment had a shorter median survival time of 19 days (range: 8–50 days), compared with their counterparts in PPS/B whose level of dependence in self-care ranged from “occasional” to “mainly” assistance. The median survival time was 43 days (range: 22–104 days) in PPS/B patients. Hence, focusing on deficits in self-care in relation to survival may yield greater accuracy in prognostication.
Our study focused on patients suffering from advanced cancer. Ninety-five percent of baseline PPS scores were in the range of PPS 10%–60% and median survival was 35 days. The PPS scores for our patient groups were decided by members of the palliative multidisciplinary team, which included physicians, nurses, and allied health staff members, who met weekly to discuss the progress of patients. In so doing, there was likely less subjectivity about an individual patient's level of deficit in each of the five domains in the PPS, resulting in the derivation of a more accurate value.
Albumin levels, as well as PPS scores documented at baseline, were found to be independently predictive of survival in multiple logistic regression analysis. Higher albumin levels in this study were associated with a better outcome. In a systematic review of 59 studies examining the relationship between serum albumin and cancer survival, lower serum albumin levels were associated with a poorer outcome. 14 Similarly, low serum albumin levels were predictive of a poor prognosis in multivariate analysis of prognostic factors in patients suffering from carcinoma of unknown origin. 15 In a study validating a predictive index for survival duration in terminally ill cancer patients, subjects with an albumin value higher than 25 g/L survived longer. 16 Our study concurs with these findings.
Gender was a predictive factor in length of survival in this study, with being female having a better outcome. In a retrospective review of the use of the PPS in end-of-life prognostication in patients within a hospice, female patients were also found to have lower hazards than their male counterparts for death. 7 Gender differences in mortality have been noted previously, with recent evidence that age-adjusted mortality rates for males were higher than for females in a large majority of cancers. 17 In a review of patients who underwent surgery for colorectal cancer, gender was also a significant predictor of 5-year survival, favoring females. 18 Reasons for gender difference in mortality are still not completely understood, although hormonal status in younger women has been put forward as a potential theory, potentially offering protection that leads to longer survival compared with their male counterparts. 19 Other reasons include differential comorbidity burden in males compared with females.
Addition of certain clinical variables may increase prognostic accuracy. With a PPV of 79%, and an AUC of 0.70, the 90-day prognostic model that incorporates baseline PPS value, albumin, white cell count, and gender may have value in identifying patients who should avail of hospice care resources. The AUC under the ROC curve for the PPS alone at 90 days in the study by Harrold and colleagues 11 was between 0.65 and 0.70, with predictive accuracy being greater for early deaths. Our study model may increase predictive accuracy of survival in patients within 90 days. A relatively simple model, it can be employed in the tertiary care setting and will be of value in decisions about pursuit of potentially burdensome treatment and utilization of community hospice resources.
Our study supports the use of the PPS in the estimation of survival time in patients suffering from advanced cancer. Objectivity regarding a patient's level of dependence in each domain of the PPS was reduced through regular meetings of the multidisciplinary team to discuss clinical progress. Given the ease with administration of the PPS and its utility, there is potential for its use in an outpatient and community palliative care setting in Singapore.
There are limitations to the study, one being the small number of patients in PPS/A. But this may be unsurprising given that our study subjects were suffering from advanced cancer. Most patients in our unit had PPS scores in PPS/B, which may not be representative of patients in other palliative care programs. However, the mean PPS baseline score of 39.1% suggests that patients with advanced cancer are likely to be functionally dependent, with more assistance required in activities of self-care. As laboratory investigation for patients at this stage of life was not always relevant to their goals and plan of care, not all variables included into the study were available for analysis. Comorbidity burden was not analyzed, and its addition may have helped explain gender difference in survival. Unfortunately, in this study the PPS was utilized only in patients suffering from advanced cancer, but it may have potential for use in patients suffering from noncancer advanced illness. Furthermore, this study was also not sufficiently powered to detect differences in survival between patients who received oncologic treatment and those who did not.
Overall, the PPS is promising in its use in patients with advanced cancer in the tertiary care setting, and potentially in the wider palliative care community. A prognostic model at 90 days encompassing the independent predictors of baseline PPS value, albumin, and gender will be further explored to determine its utility in estimating prognosis in our population of patients.
Author Disclosure Statement
No competing financial interests exist.