
Abstract
Abstract
Background:
Delirium is one of the most distressing and difficult to manage problems in advanced illness. Family caregivers have a unique view of the progression of delirium.
Objective:
This study examined precursors to delirium from the perspective of family caregivers.
Design:
This study utilized a two-stage concept mapping design that began with semistructured interviews with caregivers of patients suffering with delirium. The interview data was sorted and rated by clinicians prior to quantitative data analysis via multidimensional scaling (MDS) and cluster analysis.
Subjects/settings:
The subjects were 20 family caregivers of patients with a diagnosis of delirium in a hospice inpatient unit.
Results:
The main outcome of the study was a multidimensional model of precursors of delirium that included 99 specific items. The model included ten clusters within three general domains: Cognition, Distress, and Rest/Sleep. An exploratory analysis suggested that Rest and Sleep issues were evident to caregivers much earlier than other kinds of problems (mean=17.56 weeks prior to hospice admission, 95% CI=9.2–25.0 weeks).
Conclusions:
This study provides detailed insights from family caregivers about the progression of delirium. The caregiver observations were clustered by multivariate analysis to provide a map of symptom domains. The principal finding of this study is that sleep disturbance was identified by almost all family caregivers much earlier than other more commonly recognized symptoms associated with delirium. The study highlights the importance of sleep fragmentation in the temporal progression of delirium and points toward opportunities for improved measurement, prevention, and treatment.
Introduction
The cruel paradox of delirium is that, despite being ubiquitous within the medical setting, it remains poorly recognized and, while considered treatable, it is often untreated.10–12 The current medical interpretation of delirium may be limited by the emphasis on identification of objective factors of causality. Although delirium in certain cases is clearly linked to a specific cause such as medication, many delirious patients have no clear toxic or metabolic abnormality. 13 A more complete interpretation may require acknowledgement of less definable causes or contributing factors. Delirium is often diagnosed in its fulminate state and there is a paucity of data that describes or detects the progression of delirium. There is a need for studies that clarify the pathogenesis of delirium in order to provide earlier detection, prevent further worsening in reversible cases, and provide a strategy that reduces the risk of developing delirium. 14
Caregivers can be considered key observers to the phenomenology of delirium and often recall subtle signs and symptoms that herald the delirious episode.10,15–17 The caregiver perspective also highlights the fact that delirium has impact beyond the patient, as caregivers are often witness to the loss of personhood which characterizes delirium. Caregivers score even higher than their delirious loved ones on measures of distress and are challenged in coping with the consequences of delirium, such as agitation and sleeplessness. 1
The objective of this study was to describe caregiver observations regarding the onset, characteristics, and progression of the predelirium state in hospice patients diagnosed with delirium.
Methods
Study design
This study was reviewed and approved by the Social and Behavioral Sciences Institutional Review Board (IRB) of the University at Buffalo. Caregivers of patients admitted to a hospice inpatient unit with a diagnosis of delirium were interviewed regarding symptom development and time course in the progression of delirium. Descriptive data provided by caregivers were analyzed to identify common symptoms and to characterize the temporal course of the development of delirium in the study patients.
The study utilized a two-stage mixed methods design known as concept mapping to identify and categorize caregiver observations and descriptions of precursors to delirium. 18 Concept mapping applies multivariate statistical analysis to qualitative, descriptive data, resulting in a graphical representation of the ideas or concepts obtained from interviews or brainstorming sessions. It is particularly well suited to analysis of responses to open-ended questions. 19 In the first stage, participant statements are converted by two or more researchers to a list of single-concept phrases, or “items.” In the second stage, items are sorted by multiple participants or “experts” into categories based on similarity. Multidimensional scaling (MDS) reduces the multiple-expert representations of the items to a single two-dimensional map, where distance in the map represents similarity between items. Hierarchical cluster analysis of the MDS map coordinates results in identification of clusters of related items, which may then be grouped into a small number of categories, or “domains.”
Participants
Stage I included 20 sets of patients and family caregivers. Most of the patients (70%) had a primary diagnosis of cancer. The mean age was 77.6 years (SD=12.6), with a range of 50 to 93 years. Caregivers included 10 spouses and 10 children, of whom 11 were female and 9 male. Caregivers of patients were included in Stage I of the study based on admission to a hospice inpatient unit for delirium according to DSM IV criteria. Patient exclusion criteria were history of psychosis, thought disorder, dementia, encephalopathy, brain metastases, or signs of significant renal or hepatic impairment.
Stage II of the study involved 10 experienced palliative care providers with expertise in delirium assessment and management. The clinician group reported an average of 20.40 years (SD=12.16) of health care experience with an average of 5.95 years in full-time palliative care (SD=4.45). Six of the clinicians were MDs, two were PAs, and two were NPs. Each completed the assigned task of sorting the item cards into piles based on similarity, with the only restrictions being that all cards could not be in separate piles, nor could there be one large pile of all of the cards. The 10-card sorts were used as input for the multivariate analysis.
Procedures
The health care proxy and/or primary caregiver (PCG) provided informed consent. In Stage I of the study, caregivers met with a research team member who conducted a semistructured interview as part of the routine inpatient unit family meeting. Caregivers were asked to describe their observations regarding the onset, characteristics, and progression of the patient's condition prior to the diagnosis of delirium. The interview included questions regarding signs, symptoms, or behaviors preceding the delirium episode. They were also asked to specify the timing of the events, where able. The discussions were audio recorded and transcribed verbatim, and individual observations or items were extracted from the transcriptions.
Each interview was reviewed and coded by two research team members conjointly with the goal of identifying specific unitary items or events described by caregivers. The items were reviewed by two members of the team, who eliminated duplicates, edited very similar items to a common unique descriptor, and deleted a small number of idiosyncratic items. “Decks” of randomized cards containing one item per card were created for use in Stage II.
In Stage II, 10 palliative care clinicians were instructed to independently and freely sort the cards based on similarity between items. The only restrictions on sorting were that there needed to be more than one pile of cards, and at least one pile had to have more than one card. Statistical analysis via multidimensional scaling produced an aggregate two-dimensional map of similarity between items, followed by hierarchical cluster analysis to identify clusters of related items in the map. Clusters were named, and further grouped into three domains, based on location within the cluster mapping. The mean and 95% confidence interval (CI) were computed and compared for time of onset of symptoms within each domain. A study flow chart is presented in Figure 1.

Flow diagram of study from enrollment to completion. MDS, multidimensional scaling.
Statistical analysis
Statistical analysis followed standard concept mapping procedures as described by Kane and Trochim 18 using The Concept System Version 4.0 (Concept Systems, Inc., Ithaca, NY). The statistical analysis began with MDS of the aggregated item sorts, followed by hierarchical cluster analysis of the MDS coordinates for each item. MDS produces a goodness of fit index called the stress value, where a value of 0 represents perfect correspondence between the sorted items and the MDS coordinates, and a value of 1 represents the worst possible fit of the item sorts with the MDS coordinates. MDS produces a two-dimensional plot of all of the items in relation to each other, with similarity quantified as the distance between items. The x–y values for each item were used in hierarchical cluster analysis to identify the best representation of the concepts within the map. An iterative approach was used to find the solution that produced the most interpretable clusters and generally minimized the bridging values of the items within clusters. Bridging values range from 0 to 1 and indicate the degree to which an item was consistently sorted within the cluster under consideration versus other clusters. Low bridging values, as in the Sleep Disturbance cluster, indicate that nearly all sorters placed these items in the same category; higher bridging values suggest a more heterogeneous or complex set of items.
Results
Analysis of the interview transcripts resulted in identification of 421 items describing predelirious symptoms and events. The number of items was reduced to 99 after combining redundant items, and eliminating a few idiosyncratic entries. The MDS analysis produced an acceptable stress value of 0.246 after seven iterations. The cluster analysis produced two solutions that most clearly represented the relationships between the items extracted from the caregiver interviews. This included a 10-cluster solution illustrating specific categories of symptoms, along with a more general three-domain map showing larger domains that conceptually bound the smaller clusters. In Table 1, the 3 domain and 10 cluster models of delirium progression from the caregiver perspective are shown, along with example items of each cluster, the percentage of the 20 cases where items in that cluster were reported by caregivers, and the mean bridging value for the cluster.
The Rest and Sleep domain included four clusters: Agitation/Restlessness, Nighttime Anxiety, Sleep Disturbance, and Daytime Sleep Pattern. The Nighttime Anxiety cluster included 14 items describing problems antithetical to restful sleep, such as “Panic at night,” “Fear of sleep because of dreams,” and “Calling caregiver at night.” The Sleep Disturbance cluster contained such problems as “Difficulty falling asleep,” “Less restorative sleep,” and “Frequent awakenings;” while the Daytime Sleep Pattern cluster contained 10 caregiver observations including “Sleepiness during the day.” The 10 items in the Agitation/Restlessness cluster included similar problems that might occur at any time, such as “Agitation;” “Fidgety, always moving;” and “Moving hands, grabbing.”
The Cognition domain included three clusters related to neuropsychiatric phenomena: Gradual Cognitive Decline, Confusion, and Perceptual Disturbance. Gradual Cognitive Decline was distinguished by items reflecting noticeable loss of capacity, such as “Mental fogginess,” “Difficulty concentrating and paying attention,” and “Diminished alertness;” while the Confusion cluster included 12 items reflecting more significant impairment, such as “Not recognizing familiar faces (e.g., family);” “Loss of self-monitoring of speech (e.g., uninhibited, unfiltered, uncensored speech);” and confusion about time and location. There were nine items in the Perceptual Disturbance cluster, including “Visual hallucinations,” “Conversations with people who are not there,” “Auditory hallucinations,” and other items characteristic of a delirious state.
The Distress domain of the map included three clusters containing many common phenomena observed in palliative care. For example, the Psychological Distress cluster included 12 specific issues, such as “Curiosity/worry about the dying process, including pain, feelings, spiritual status, timeline, foreknowledge;” “Depressed mood;” and “Frustration re: loss of independence and autonomy.” The Physical Distress cluster included “Pain,” “Weakness,” and “Unable to eat,” among a total of nine symptoms common to advanced illness. There were four items in the Family Caregiver Distress cluster, including “Caregiver anxiety, stress, exhaustion” and “Caregiver does their best to understand/manage symptoms with limited knowledge.”
The PCG interview included attention to the time course of symptom emergence. Caregivers were asked to recall how long ago the specific issue named was observed. For approximately half of the original items (201 of the full set of 421; 47.7%), a specific timeframe was recalled, which was expressed in weeks. Two members of the research team coded the 201 items for which onset time was identified on the three major clusters. The overall level of agreement in the coding was high, with disagreement on only nine items and a coefficient kappa of 0.91. An exploratory analysis was conducted to examine whether the time estimates were differentially associated with the three domains. There appears to be a clear pattern as depicted in Figure 2. A total of 67 Rest and Sleep issues were observed an average of 17.55 weeks prior to admission for delirium (95% CI=9.2–25.9), followed by 32 Distress items at 11.36 weeks (95% CI=2.3–20.4) and 101 Cognition items with a mean reported onset 6.36 weeks (95% CI=3.3–9.5) prior to admission. A one-way analysis of variance was conducted with weeks as the dependent variable and domain category as the independent variable. Contrasts between Cognition and the other two domains were also computed. The overall model produced an F of 4.12 (p=0.018) with a significant difference in the Rest and Sleep versus Cognition contrast (Dunnett's T3, p=0.040). The mean difference between these clusters was quite large, at 11.2 weeks.
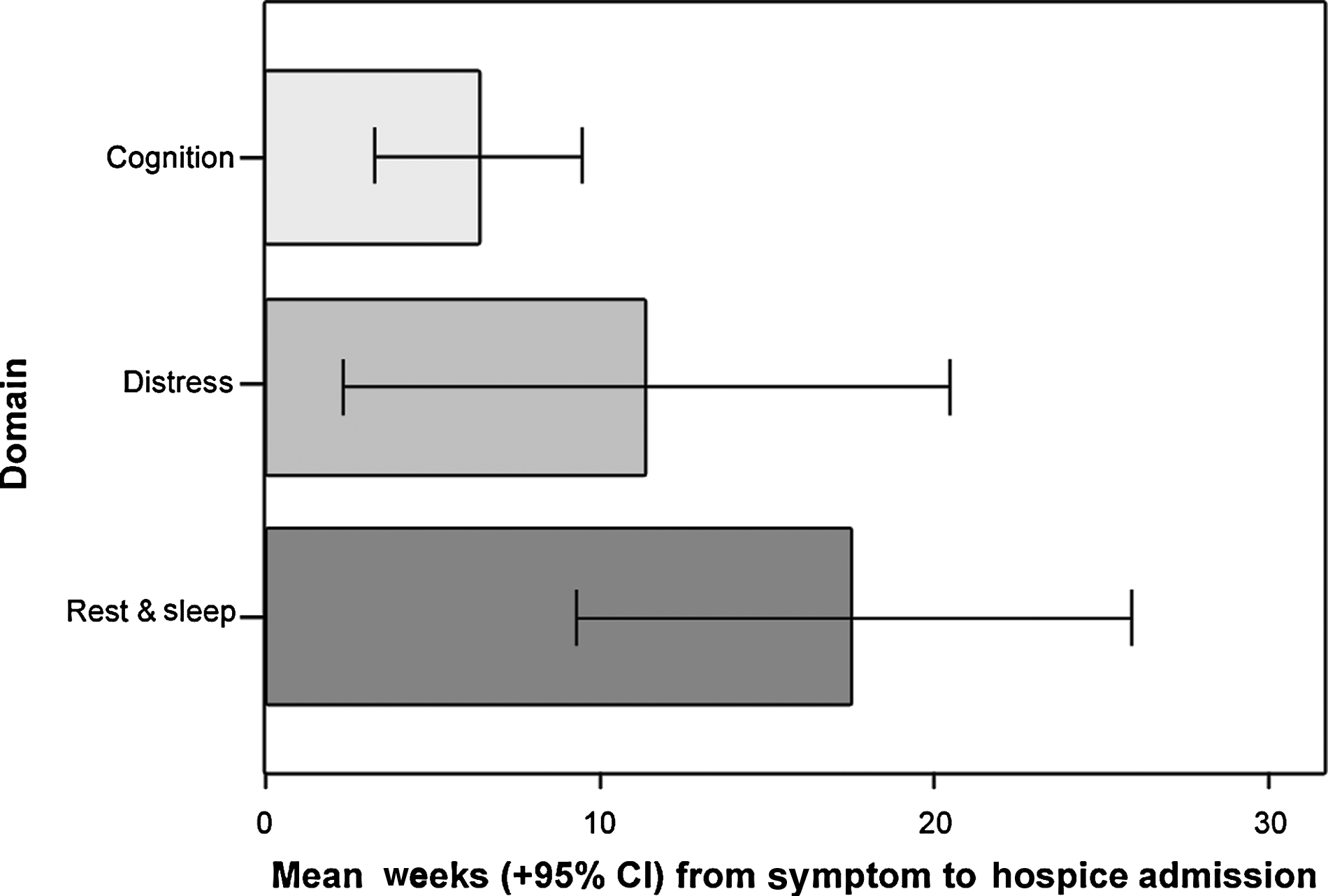
Error bar chart of delirium domains by time to hospice admission. CI, confidence interval.
The final analysis examined the relationship between the 10 clusters and time. In Figure 3, median time to admission to a hospice inpatient unit with acute delirium is plotted by cluster. Medians were chosen, because they are not influenced by outlying values, which might be particularly strong in a plot with a relatively large number of divisions of the data as in the 10-cluster solution. The pattern of early emergence of problems in Rest and Sleep is again apparent, with more typical delirium symptoms observed closer to time of admission. As this plot shows, three of the four clusters in the Rest and Sleep domain emerged before any of the clusters in the Cognition domain, which includes the more recognizable features of acute delirium. The fourth Rest and Sleep cluster, Agitation and Restlessness, emerged after the Cognition clusters.
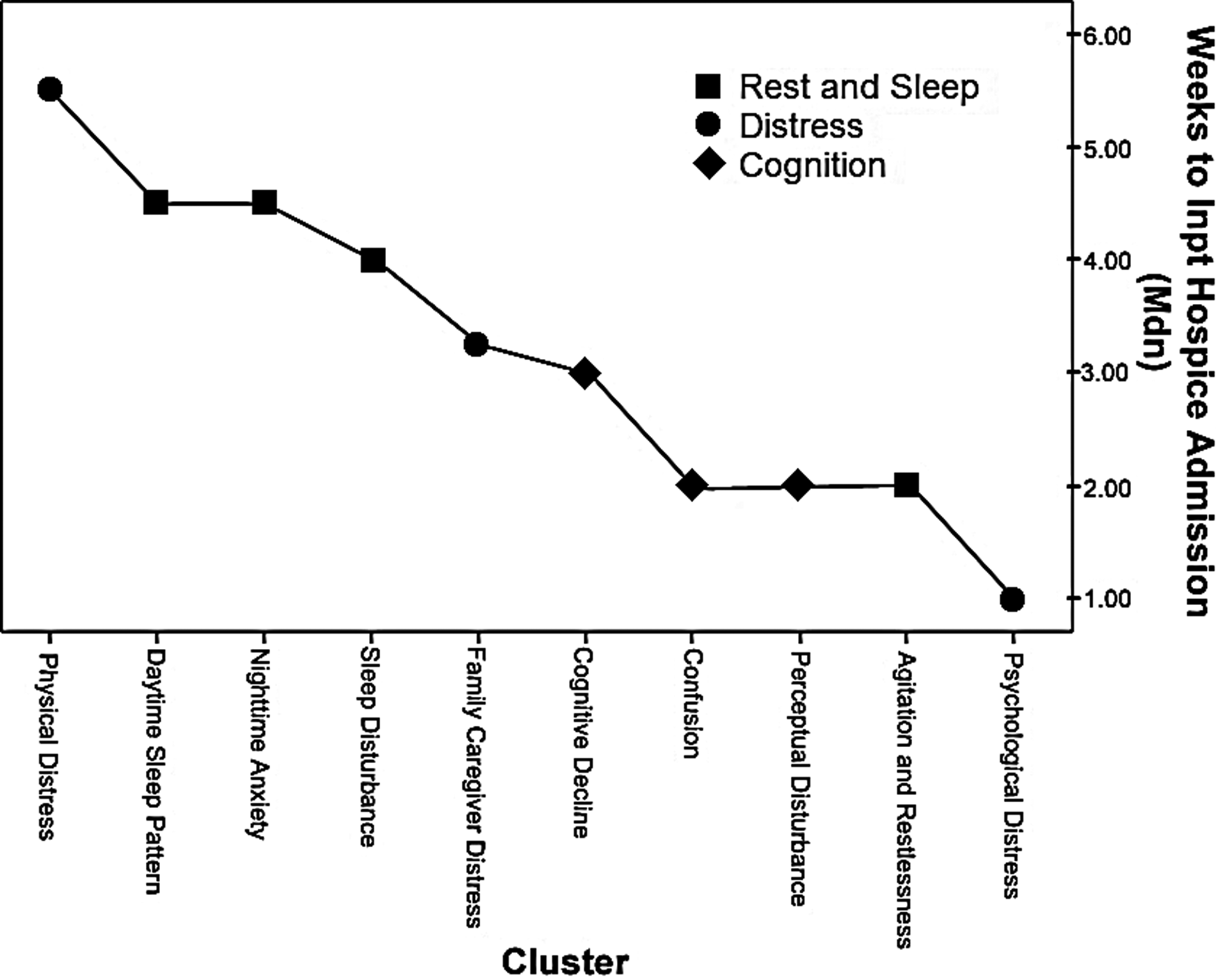
Plot of delirium clusters by time to hospice admission.
Discussion
This study utilized two kinds of “expertise” to describe the pathogenesis of delirium. The first was that of family caregivers who observed a loved one's progression toward an episode of delirium that warranted inpatient hospice admission. Caregivers met with a research team member to describe the signs, behaviors, and symptoms preceding the delirious episode. The study also drew on the expertise of hospice clinicians, who sorted caregiver observations into symptom clusters based on commonality. The result of this combined expertise is a three-level conceptual model that describes the clinical course progressing to delirium: (1) a list of 99 signs and symptoms observed by caregivers prior to the diagnosis of delirium, (2) 10 symptom clusters, which were identified by clinicians according to similarity, and (3) three major domains of symptom clusters. The list of specific symptoms provides a source of items that could be used in developing a predictive instrument for delirium, while the 10-cluster solution suggests potential subscales of such an instrument. The clinician-sorted symptom clusters and both major and minor symptom domains provide a conceptual structure that is descriptive of the pathogenesis or prodrome towards delirium.
One of the principal findings of this study is that sleep disturbance was identified by almost all family caregivers much earlier than other more commonly recognized symptoms associated with delirium. This suggests that there may be a temporal progression to delirium, with a prodromal phase characterized by sleep fragmentation and progressing towards cognitive deterioration with diminishing likelihood of reversibility. It is well established that sleep disturbances are common in patients with serious illness and that delirium is a near inevitable consequence of dying.2,6 The inversion of the sleep-wake cycle in delirious patients is an old observation, and delirium is an amalgam of several variables influenced by sleep, including alertness, awareness, arousal, and attention. The question remains whether the relationship between sleep disturbance and delirium is causal or correlational.3,20,21 Sleep deprivation leads to several clinical manifestations of delirium, and there is overlap between the symptoms caused by sleep loss and those associated with delirium.22,23 A recent prospective, longitudinal study of 105 hospice patients found that poor sleep quality precedes delirium onset, suggesting a causal relationship between sleep disturbance and delirium. 24 Others have proposed a link between severe REM deficiency and the development of delirium in neurodegenerative disease25–28 as well as in ICU patients. 29
The risk factors for delirium are multiplicative 30 and can be conceptualized as a “threshold” model in which there is a relationship between predisposing and precipitating factors that reaches a clinical threshold. 3 The findings of this study suggest that sleep disturbance may be an early predictor or risk factor for the onset and pathogenesis of delirium. Recognition of the core deficit of sleep dysfunction may help direct the clinician to the early signs of delirium and may also prompt earlier treatment of other causes of delirium such as infection or adverse medication reaction. Issues such as changes in sleep quality represent an opportunity to counsel patients and caregivers on the potential development of delirium and thereby reduce caregiver stress. 24 In a recent study, nearly half of all cancer patients reported difficulty falling asleep, waking up frequently in the night, and vivid dreaming. 31
Previous studies have demonstrated the deleterious consequences to those caring for patients with sleep-wake disturbances 31 and/or delirium.2,32 The current study adds to this evidence but also highlights the incidence of predelirious behaviors and symptoms that contribute to the sufferable state for both the patient and the caregiver. While the diagnosis of delirium may be ‘acute,’ those providing care witness a remarkably similar course of protracted patient decline and suffering. The current study suggests the existence of a constellation of signs and symptoms that precede delirium by weeks to months, and those providing care witness a remarkably similar course of protracted patient decline and suffering. Many of the issues raised by caregivers, such as nocturnal agitation, may not be routinely assessed in proportion to the actual clinical prevalence. It can be argued that delirium is one of the most common events for patients at the end of life, yet one of the least anticipated by caregivers who are unknowingly witnessing its emergence. A better understanding of the psychopathological sequence of delirium may improve diagnostic acumen, ease suffering, and provide meaningful support to the patient and their caregivers.
The study is limited by the retrospective identification of delirium precursors by family caregivers, perhaps especially in estimation of timing of events. However, the retrospective interviews generated a large number of specific predelirious events that could only be known in hindsight. These events could form the basis of an item pool that can be utilized in a prospective study on the development of delirium. A prospective hypothesis testing study would enable examination of the causal relationships suggested in the retrospective exploratory study presented here. The sample sizes in both phases of the study were considered adequate, but whether the findings would be replicable with different caregivers or clinicians is an important empirical question. It would also be interesting to determine if the model identified here would be replicable with clinicians who were not aware of patients' delirium diagnosis. Similarly, the long-term meaningfulness of the items, clusters, regions, and ratings can be tested in future studies aimed to improve measurement, prevention, and management of delirium in advanced illness.
Footnotes
Acknowledgments
The authors gratefully acknowledge the following individuals for their contributions, constructive discussion, and critical reading of the manuscript: Megan Farrell, MD, Elizabeth Maher, MD, Cary Sisti, NP, Kristi L. Szarpa, NP, John Tangeman, MD, and Stefanie Von Ohlen, LMSW.
Author Disclosure Statement
The authors declare that there is no conflict of interest.