
Abstract
Abstract
Background:
Complex interventions are common in palliative and end-of-life care. Mixed methods approaches sit well within the multiphase model of complex intervention development and evaluation. Generic mixed methods guidance is useful but additional challenges in the research design and operationalization within palliative and end-of-life care may have an impact on the use of mixed methods.
Objective:
The objective of the study was to develop guidance on the best methods for combining quantitative and qualitative methods for health and social care intervention development and evaluation in palliative and end-of-life care.
Methods:
A one-day workshop was held where experts participated in facilitated groups using Transparent Expert Consultation to generate items for potential recommendations. Agreement and consensus were then sought on nine draft recommendations (DRs) in a follow-up exercise.
Results:
There was at least moderate agreement with most of the DRs, although consensus was low. Strongest agreement was with DR1 (usefulness of mixed methods to palliative and end-of-life care) and DR5 (importance of attention to respondent burden), and least agreement was with DR2 (use of theoretical perspectives) and DR6 (therapeutic effects of research interviews). Narrative comments enabled recommendation refinement. Two fully endorsed, five partially endorsed, and two refined DRs emerged. The relationship of these nine to six key challenges of palliative and end-of-life care research was analyzed.
Conclusions:
There is a need for further discussion of these recommendations and their contribution to methodology. The recommendations should be considered when designing and operationalizing mixed methods studies of complex interventions in palliative care, and because they may have wider relevance, should be considered for other applications.
Introduction
Q
Numerous generic mixed methods resources exist, and there are an increasing number of examples of mixed methods studies conducted in palliative and end-of-life care (for examples of both, see Farquhar et al 2011 4 ). However, insufficient experience with this approach in palliative and end-of-life care research exists to support any best practice recommendations that are sufficiently detailed to be practically applied. The infancy of mixed methods in this field was well demonstrated by a review by Flemming et al, which identified just one published randomized controlled trial (RCT) that included a qualitative element among 146 palliative care RCTs. 7 Guidance will develop as more palliative and end-of-life care research with an integrated mixed methods approach is designed, delivered, and available for evaluation.
Generic guidelines are very useful, however there are challenges in the design and operationalization of studies within palliative and end-of-life care that affect the use of mixed methods. To address this, a one-day workshop, organized as part of the MRC and National Institute for Health Research (NIHR) Project MORECare, 8 brought together a diverse group of experts in mixed methods and palliative and end-of-life care research. The workshop and follow-up consensus exercise were intended to create guidance on the best methods for combining and integrating quantitative and qualitative methods for health service and social care intervention development and evaluation in palliative and end-of-life care.
Methods
Participants
Potential workshop delegates from across the United Kingdom were identified from the published literature on mixed methods and palliative and end-of-life care research. We sought approximately 30 delegates and expected a 50% response rate. All workshop delegates and the MRC MORECare Programme Advisory Group (PAG) were also invited to participate in a follow-up consensus exercise (short web-based survey).
Procedure
The study was approved by the University of Manchester Ethics Committee. Informed consent was obtained from all participants. The workshop began with a brief context-setting introduction defining complex interventions, 3 outlining the MRC framework for the development and evaluation of complex interventions,3,5,6 giving definitions of palliative 9 and end-of-life care 10 (see Table 1), and discussing six key challenges (recruitment, attrition, differing disease trajectories, respondent burden, randomization, and outcomes) of palliative and end-of-life care research identified from the published literature11–45 that may impact the use of mixed methods (see Table 2).
Three presentations were given by experienced mixed methods researchers on (i) mixed methods approaches to evaluating health care; (ii) combining qualitative and quantitative methods to give a fuller answer to research questions; and (iii) including qualitative methods in trials of health and social care interventions. Each was followed by open discussion with delegates.
Delegates then participated in one of three facilitated groups of 10–12 people. In order to ensure coverage of all types of studies, each group focused on a different phase(s) of the MRC framework: Group 1 on Pre-Clinical and Phase I studies, Group 2 on Phase II and Phase III randomized controlled trials, and Group 3 on Phase IV Implementation Studies. Group allocation was based on a combination of delegates' prior preferences depending on their area of expertise and a balance of group size. Within their groups, delegates were asked to identify potential recommendations for guidance on integrating qualitative and quantitative methods in the development and evaluation of complex interventions in palliative and end-of-life care in relation to their phase(s) of the MRC framework.
Each group was moderated by an experienced facilitator who explained the task and then kept delegates on task but stimulated discussion of issues as they arose. Facilitators asked participants to each spend ten minutes writing potential recommendations on cards, based on their expertise and experience. The cards were then read by each delegate to the group. Potential recommendations were entered on a laptop for screen projection to facilitate discussion. Each group then clarified and rephrased items as required. Any cards not considered to be duplicates that had not been read out were saved for later transcription. Each group was audiotaped, with permission, using digital recorders. The recordings enabled later synthesis of items into potential recommendations by the research team. Thus the Transparent Expert Consultation process was used, 46 based on a modified nominal group technique. Nominal group techniques have a long history of use in health and medicine, providing a structured format for discussion and synthesis of information, with the aim of rapidly producing solutions or decisions. 47
Following the workshop, items for potential recommendations from across the three groups were combined: over 200 items had been generated. The numerous duplicate items were removed by members of the research team, followed by items that were too generic, rather than specific to or pertaining particularly to palliative and end of life care research. The remaining items were synthesised into potential recommendations. A reduced list of nine draft recommendations was thus generated for presentation to all workshop participants and all members of the MRC MORECare PAG via a brief online consultation. Participants scored their level of agreement for each draft recommendation on a scale 1–9 (1, low; 9, high) using an anonymous web-based survey; written comments were also solicited.
Analysis
Descriptive statistics (frequencies and medians) and plots (box plots of inter-quartile ranges) were used to summarise and analyse the ratings of agreement, and grouped by level of agreement and level of consensus (see Table 3). Narrative comments were read in order to provide meaning to the quantitative ratings given; they were then summarized for reporting and informed the refinement of the nine draft recommendations. The recommendations were then considered in relation to the six identified key challenges of palliative and end-of-life care research upon which mixed methods may impact.
Results
Thirty-three delegates took part in the one-day workshop. These included 17 predominantly palliative and end-of-life care researchers and 16 health services researchers out of 67 invited: of the 34 nonparticipants, 9 had initially agreed but then had to withdraw. For the online follow-up consultation, 58 people were eligible and a 45% response rate was achieved (n=26/58), following a reminder at two weeks.
Table 4 lists the nine DRs and the median levels of agreement achieved by each in the online consultation. Figure 1 shows the range of levels of agreement and interquartile ranges for each draft recommendation.
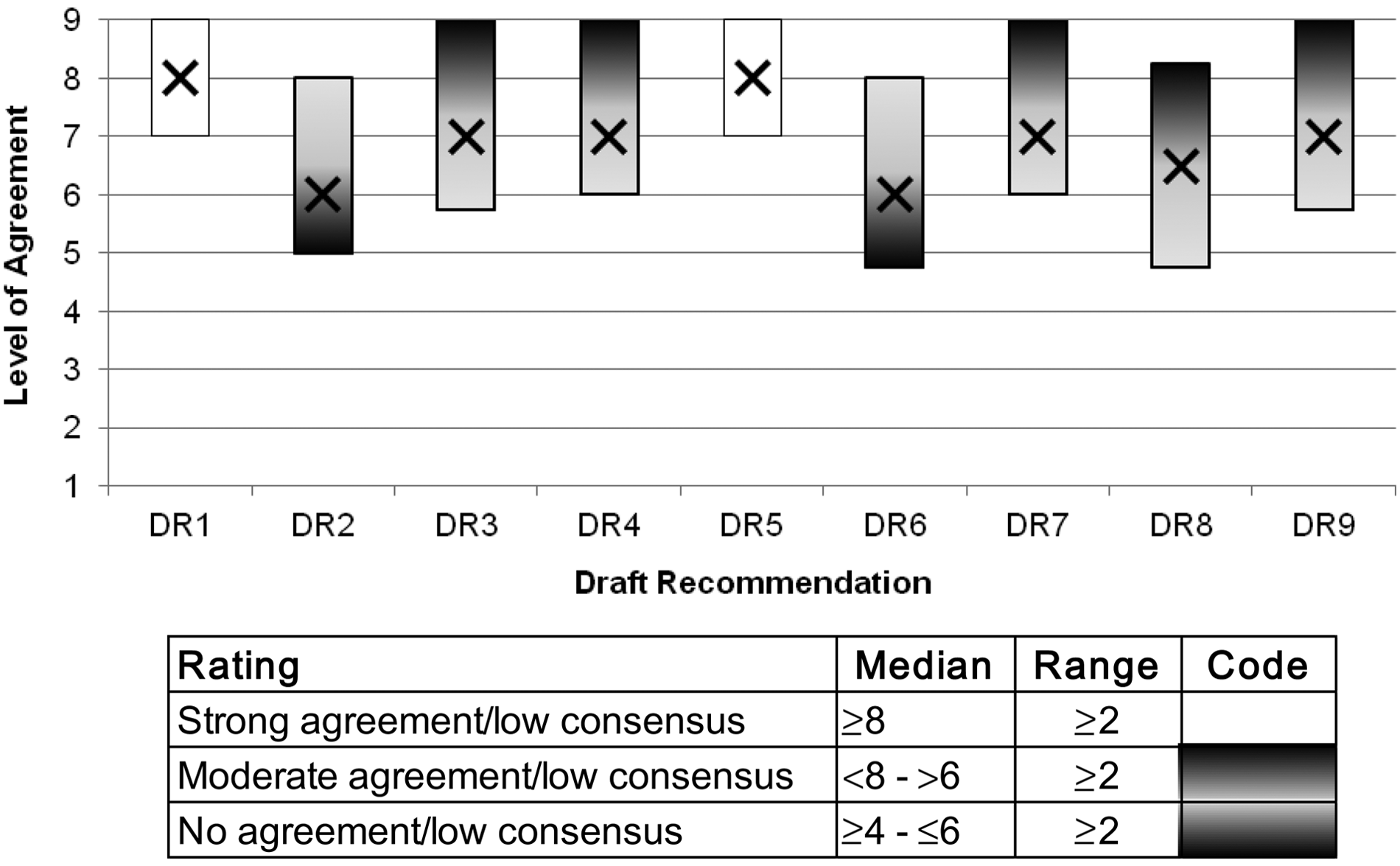
Box plot of the Interquartile ranges and medians of levels of agreement for the nine recommendations (box:25th and 75th percentiles).
Number of respondents=26;
Potential range 1–9: 1=strongly disagree; 9=strongly agree
DR=draft recommendation; IQR=interquartile range; R=fully endorsed recommendation; PR=partially endorsed recommendation; RDR=refined draft recommendation; RCT=randomized controlled trial
When considered in relation to Table 3, Table 4, and Figure 1, the strongest agreement (but low consensus) was with DR1 (the usefulness of mixed methods to palliative and end-of-life care research) and DR5 (the importance of attention to respondent burden), and the lowest level of agreement and consensus was with DR2 (the use of theoretical perspective) and DR6 (therapeutic effects of research interviews). Thus only DR1 and DR5 could be transitioned into fully endorsed recommendations (Rs; R1 and R5), five DRs could be transitioned into partially endorsed recommendations (PRs; PR3, PR4, PR7, PR8, and PR9), and two remained as DRs (DR2 and DR6).
Table 4 also provides a summary of the narrative comments in relation to each DR. Respondent comments linked to lower ratings for a DR sought clarification of recommendations (e.g., in relation to DR2 [the explicit use of theoretical perspective]), stated that methodology choice depended on the research question (e.g., in relation to DR3 [multidisciplinary team] and DR4 [exploration of the participation experience]), or expressed the view that the area was not problematic either in general or in the specialist field of palliative and end-of-life care research (e.g., DR5 [respondent burden], DR6 [therapeutic effects of research interviews], and DR8 [researcher skill-sets]). In light of the strength of agreement and the narrative comments, the final column of Table 4 presents refined versions of the two Rs, five PRs, and two DRs (then becoming refined draft recommendations [RDRs]). Figure 2 summarizes the entire process from initial item generation to the final transition into fully endorsed, partially endorsed, and refined draft recommendations.

Transition from items for potential recommendations to full recommendations.
A further set of narrative comments generated at the end of the online consultation raised important points, such as the need to consider mixed methods in palliative and end-of-life care studies other than those relating to the development and evaluation of complex interventions; the generic nature of many of the recommendations; the importance of the timing of participant recruitment in relation to the challenge of illness trajectories in palliative and end-of-life care; and the likely variation in the importance of recommendations depending on the audience, e.g., some will be more important for commissioners of research.
Due to the range of expertise among workshop delegates, the workshop had commenced with a context-setting presentation of six key challenges of palliative and end-of-life care research. The results of an analysis of the relationship of these key challenges to each recommendation (Rs, PRs, and RDRs) are provided in Table 5.
Discussion
There was moderate agreement among the respondents with the majority of the draft recommendations. This relatively modest level of agreement may relate to the subjective nature of qualitative and mixed methods research, or to the fact that not all of the initial delegation participated in the consensus exercise, which suggests that further development of the recommendations may be warranted. The highest level of agreement was with the usefulness of mixed methods to palliative and end-of-life care research (DR1) and attention to respondent burden (DR5), and the lowest level of agreement was with the use of theoretical perspective (DR2) and the therapeutic effects of research interviews (DR6). Thus only DR1 and DR5 were transitioned into fully endorsed recommendations (R1 and R5), five DRs were transitioned into partially endorsed recommendations (PR3, PR4, PR7, PR8, and PR9), and two remained as DRs requiring further debate but which we were able to refine (RDR2 and RDR6). Our analysis of the recommendations in relation to the six identified key challenges of palliative and end-of-life care research suggests that mixed methods should not be used in an attempt to address these challenges; rather it suggests that mixed methods can be appropriately used in relation to relevant research questions, but that the impact of mixed methods on these six key challenges should be considered, and that the recommendations may facilitate this.
Variations on five of these nine recommendations (i.e., R1, RDR2, PR3, R5, and PR8) may be found in generic texts on mixed methods. What this study adds, however, is that the wording of these five recommendations and the accompanying commentary presented here highlight those features of mixed methods research that should be considered when designing mixed methods studies within the particular context of palliative and end-of-life care: how to apply them and why. Thus these five recommendations are adaptations to existing mixed methods guidance. However, the remaining four (PR4: exploration of the participant experience; RDR6: therapeutic effects of research interviews; PR7: study registers to include mixed methods; and, PR9: contribution of mixed methods to implementation studies) are less often discussed in the established mixed methods literature and could thus be considered as potential new additions to even generic mixed methods guidance.
Reflection on the workshop process and outcome
The workshop generated a vast number of potential recommendations. Although most but not all were relevant to mixed methods research, the majority were not related to palliative and end-of-life care research and the challenges they face. This lack of focus on palliative and end-of-life care research may have reflected the lack of experience of some delegates in this specialized field, despite the context-setting presentation at the start of the workshop. In addition, a few of the potential recommendations generated did not take the form of recommendations but were individual words written on the cards. This varying level of development of the potential recommendations within the groups probably relates to the limited time for the group-work rather than any failings of the task set or its facilitation.
One of the limitations of this study is that the recommendations developed and their subsequent ratings may only reflect the views of those who participated in the study. All of the recommendations, regardless of their level of endorsement, will therefore benefit from wider discussion and application for their further refinement and uptake, in the spirit of calls for greater discourse.4,47
Conclusion
The results of the workshop and consensus exercise presented here suggest further discussion and consideration of these recommendations when designing and operationalizing mixed methods studies of complex interventions in palliative and end-of-life care research. These recommendations may not be regarded as entirely exclusive to palliative or end-of-life care research, but recommendations that are particularly helpful for palliative or end-of-life care research because of their known challenges. They may therefore inform other areas of research that face similar challenges and seek to apply mixed methods in addressing appropriate research questions. The recommendations may also be regarded as relating to studies other than those focused on the development and evaluation of complex interventions and so may have wider relevance.
This study identifies a need for robust evidence on the nature and duration of therapeutic (and potentially confounding) effects of interviewing and the need to consider that recommendations may vary in their importance depending on the research question, its context, and its audience.
Footnotes
Acknowledgments
MORECare is funded by the NIHR and managed by the MRC as part of the Methodology Research Programme (grant reference number G0802654/1). MORECare aims to identify, appraise, and synthesize best practices to develop and evaluate palliative and end-of-life care, particularly focusing on complex service-delivery interventions and reconfigurations.
We acknowledge Alicia O'Cathain, Elizabeth Murray, and Simon Lewin for presenting at the workshop; Catherine Walshe for additional facilitating; Ellie Anscombe for additional scribing; Mark Pilling for analysis of quantitative data; Stacey Body and Susie Edwards for administrative support; all delegates for participation in the workshop, and all respondents to the online consultation exercise; and the Cicely Saunders Institute for hosting the workshop on behalf of MORECare.
The principal investigator of this study is Irene J. Higginson, and the co-principal investigator is Chris Todd. The members of MORECare are co-investigators Peter Fayers, Gunn Grande, Richard Harding, Matthew Hotopf, Penney Lewis, Paul McCrone, Scott Murray, and Myfanwy Morgan; the project advisory group is Massimo Costantini, Steve Dewar, John Ellershaw, Claire Henry, William Hollingworth, Philip Hurst, Tessa Inge, Jane Maher, Irene McGill, Elizabeth Murray, Ann Netten, Sheila Payne, Roland Petchey, Wendy Prentice, Deborah Tanner, and Celia A. Taylor; the researchers are Hamid Benalia, Catherine J. Evans, Marjolein Gysels, Nancy J. Preston, and Vicky Short.
The workshop was funded by MORECare, CECO, and COMPASS. Morag Farquhar was funded by Macmillan Cancer Support.
Author Disclosure Statement
No conflict of interest has been declared by the authors.