
Abstract
Abstract
Background:
Palliative care services are lacking in rural hospitals. Implementing palliative care services in rural and remote areas requires knowledge of available resources, specific barriers, and a commitment from the hospital and community.
Objective:
The purpose of the study was to determine awareness, knowledge, barriers, and resources regarding palliative care services in rural hospitals.
Methods:
A descriptive survey design used an investigator-developed needs assessment to survey 374 (40% response rate) health care providers (chief executive officers, chiefs of medical staff, chief nursing officers, and social worker directors) at 236 rural hospitals (<100 beds) in seven Rocky Mountain states.
Results:
Significant barriers to integrating palliative care exist: lack of administrative support, mentorship, and access to palliative care resources; inadequate basic knowledge about palliative care strategies; and limited training/skills in palliative care. Having contractual relationships with local hospices is a key facilitator. Respondents (56%) want to learn more about palliative care, specifically focusing on pain management, communication techniques, and end-of-life care issues. Webinar and online courses were suggested as strategies to promote long distance learning.
Conclusions:
It is imperative for quality of care that rural hospitals have practitioners who are up to date on current evidence and practice within a palliative care framework. Unique challenges exist to implementing palliative care services in rural hospitals. Opportunities for informing rural areas focus around utilizing existing hospice resources and relationships, and favoring Web-based classes and online courses. The development of a multifaceted intervention to facilitate education about palliative care and cultivate palliative care services in rural settings is indicated.
Introduction
Challenges to implementing rural palliative care services include differences in the environment, infrastructure, and resources.1–4 Barriers include lack of administrative support, mentorship, and access to resources to implement change; inadequate palliative care knowledge and skills; and insufficient training.4–7 Additionally, personnel constraints, limited access to physician mentors or advance practice nurses with palliative care skills, and lack of resources (both financial and human) for palliative care are present.1,8,9 While some similarities exist, rural communities have unique characteristics.
Rural patient populations tend to be widely distributed over large, sparsely populated geographic areas whose resources cannot support specialists knowledgeable about palliative care. Primary care providers (physicians and advance practice nurses) play important roles, but in rural areas they may not have the knowledge and skills to deliver palliative care effectively. Rural health care professionals may perceive they are providing palliative care, yet identify significant barriers, which they perceive differently based on their role. 5 Many rural palliative care services respond only to the individual patient's needs and do not exist as coordinated plans to address population needs. It is imperative for quality of care that rural hospitals have practitioners who are knowledgeable on best palliative care evidence.
A systematic review examined the organizational provision of palliative care in rural settings and found that primary care professionals reported difficulty in obtaining education and training in palliative care and had inadequate knowledge related to pain and symptom management and emotional issues, e.g., support and bereavement counseling. 1 They viewed information technology developments such as Web-based interventions and telemedicine as possible solutions.
Multiple programs have been implemented to bring palliative care services to rural communities. The national Rural Palliative Care Project (RPCP), funded by the Australian Government Department of Health and Aging, provides resources to remote general practices to implement key elements of a rural palliative care model, addressing communities' local needs. 10 The program goal, to provide rural Australia access to high-quality, coordinated palliative care, includes the establishment of a Web-based resource kit. In addition, Project ENABLE II, a randomized controlled trial to improve palliative care for advanced cancer patients, found it was feasible to provide educational and care management consultation in rural New Hampshire communities. 11 The Palliative Care Education, Research, and Training project at the University of New Mexico created a palliative care network of seven rural communities, with successful access to palliative care expertise of physicians and project team. 12 Essential features for successful rural palliative care models include coordinated program development building, access to resources and partnerships, and implementing outcome pain and symptom management measurements.3,13 Based on focus groups of interdisciplinary Canadian rural health care providers, a theoretical model was developed to guide the development of rural palliative care programs suggesting a needs analysis before creating a team and developing a program. 14
Objective
Our study's purpose is to assess awareness, activity, and available resources related to palliative care in rural hospital practice settings. Future goals include using needs assessment results to inform the development of a multifaceted palliative care educational intervention for rural hospital health care providers.
Methods
A descriptive survey gathered data from chief executive officers, chiefs of medical staff, chief nursing officers, and social work directors in 236 Rocky Mountain rural hospitals (<100 beds) in seven states (Colorado, Wyoming, western Nebraska, western Kansas, northern New Mexico, Montana, and eastern Utah). Hospitals were selected from the American Hospital Association Registry; hospital leadership staff were identified from individual hospital websites to facilitate direct survey mailing. An invitation to complete the needs assessment was disseminated in spring 2010 to targeted health care providers (N=944) by U.S. Postal Service mailing with a stamped, self-addressed return envelope for the completed survey. A two-dollar incentive was included; postcard reminders were mailed three weeks later. 15 The Colorado Multiple Institutional Review Board determined this study was not human subjects research.
Instrument development
An extensive literature review identified previously developed needs assessment instruments assessing palliative care provision in the following key areas: services provided, staff education offered, barriers to palliative care delivery, and resources useful to participating institutions.8,16 An expert panel of palliative care physicians, nurses, and interdisciplinary team members reviewed results, making final recommendations for an assessment tool to determine interest, knowledge, and existing resources regarding rural hospital palliative care.
The seven-section instrument includes both quantitative and qualitative questions addressing current palliative care services, professional education programs, desired learning methods, satisfaction with and barriers to palliative care provision, available community resources, and populations requiring assistance. Respondent demographic and hospital characteristics were also queried. Several questions asked what respondents would like to learn about palliative care and how they preferred to receive that information. An additional question asked what would make it possible for rural staff to attend a palliative care offering.
Data analysis
Quantitative survey items and demographics were summarized with descriptive statistics, tests of difference, and association, using SPSS 19.0 (SPSS Inc., Chicago, IL). 17 Missing data were omitted from each calculation. Significance was tested at ά=0.05. Qualitative responses were analyzed by research team members, who collaborated face to face for the final analysis. Using content analysis, the researchers combined the responses into thematic groups, reconciling rival explanations until consensus was achieved. 18
Results/Quantitative
Demographics
Of the potential 944 health care providers, 374 participated (response rate 40%) from 199 hospitals in seven states (see Figure 1) and included nurses (44%), physicians (24%), social workers/case managers (17%), and hospital administrators (15%). The average respondent had 21.8 years of experience (SD±10.80), personally cared for six patients (SD±6.30) in the past year who had died, and was employed in a critical access hospital (82%) with a mean (M)=25.60 licensed beds (range 4–99) and an average daily census of 11 patients.

Survey respondents' geographic locations.
Palliative care services
When asked how familiar respondents were with the palliative care concept, 58% and 41% said they were very or somewhat familiar, respectively. Respondents believed palliative care is integrated into the care plan for seriously ill patients (M=1.61; SD±0.80) and health care professionals are able to recognize the active dying process (M=2.23; SD±0.58) with 0=never, 1=sometimes, 2=frequently, 3=always. Responding to the statement, “I believe staff is comfortable knowing what to do for the dying patient,” health care professionals indicated concurrence (M=2.02; SD±0.62, with 0=strongly disagree, 1=disagree, 2=agree, 3=strongly agree). Respondents identified the most common existing palliative care services offered in rural hospitals (see Table 1) as having a contractual relationship with a community hospice to provide such care and having a program to promote advance directive completion. Less common were professional palliative care educational programs and having access to board certified hospice/palliative care physicians.
More than one response may have been recorded.
Palliative care education and learning methods
Seventy-two percent of respondents (n=271) recalled a palliative care professional educational offering to their rural hospital staff in the previous year (see Table 2). The most common inservice content included advance directive completion, community hospice resources, and pain management. Asked to share how they would like to learn more about palliative care, respondents identified various modalities (see Figure 2), favoring Web-based classes and online self-study modules. Attending a workshop or partnering with local hospice providers and area health education centers were other preferred learning methods.
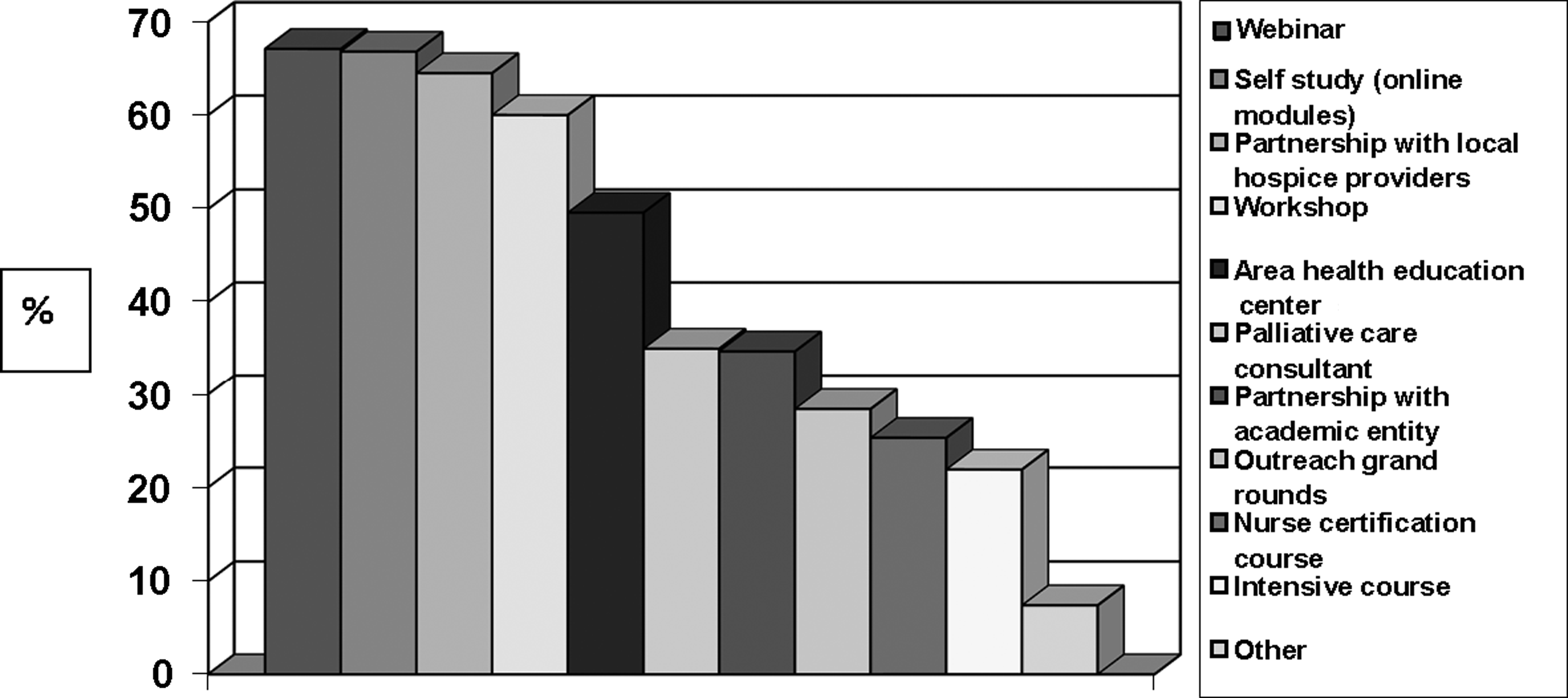
Preferred methods to learn more about palliative care (n=374). More than one response may have been recorded.
More than one response may have been recorded.
Satisfiers and barriers to the provision of palliative care
Concerning palliative care delivery, respondents were satisfied (0=not satisfied; 3=extremely satisfied) with the degree to which advance directives (M=2.43; SD±0.67), pain (M=2.30; SD±0.70) and symptom management (M=2.10; SD±0.77), and effective transitions for discharge plan of care (M=1.99; SD±0.74) were addressed. Health care professionals were less satisfied with ethical issue discussions (M=1.65; SD±0.89) and psychosocial support provision (M=1.68; SD±0.80).
From a list of barriers to providing optimal palliative care to hospitalized patients, respondents most often identified patients'/families' avoidance of issues around dying (M=1.1; SD±0.51), lack or inadequacy of written palliative care policies/procedures (M=0.99; SD±0.68), and lack of health care professional palliative care knowledge (M=0.91; SD±0.54).
Results/Qualitative
Palliative care education topics
Responding to an open-ended question, 55% (n=205) wanted to learn more about palliative care. The most common responses to, “What specifically would you like to learn?” (n=119; multiple responses possible) included pain management (n=34), general education about palliative care (n=33), end-of-life communication (n=26), end-of-life care and symptom management (n=16), and business management (n=16).
Concerning pain management, respondents specifically mentioned prescribing and dispensing analgesic medications (e.g., alternatives to intravenous administration). The general education category included a desire to correct basic misconceptions about palliative care and “anything that can help my staff and patients to understand.” Desired communication techniques included counseling of and communication with families; preparing patients, families, and coworkers to accept end of life; communicating bad news; bereavement counseling; and interacting with physicians. Care management topics ranged from service coordination, interdisciplinary care programs, and end-of-life care to specifics such as transferable physician orders and setting standards for individualized care. Respondents indicated a substantial need for business management education, including implementation of palliative care in small hospitals and across departments, Medicare skilled nursing criteria, transitioning from acute to palliative care, reimbursement, and liability.
Other concerns, less frequently mentioned, included community and institutional climate, e.g., availability of resources, palliative care sources other than hospitals, and clinician buy-in; staff issues; quality improvement; and the need for ethics committees.
Facilitation of palliative care education
Fifty-nine percent (n=221) offered suggestions for making it possible for staff to attend a palliative care course. Primary issues included location (n=92); course funding (n=68); electronic educational forums (n=61); and timing, especially for staff coverage (n=63). Since travel is expensive, respondents preferred local education sites or technology-based media such as Webinars, teleconferences, and online courses. To make offsite education financially possible, respondents desired “decent” prices or waiving of registration fees, funding for transportation/lodging, free continuing education credits, paid time off, or funds to pay for additional staff coverage. Respondents noted the need for substantial advance notice (at least three months) to allow for scheduling and for the subsequent year's budgeting. They suggested flexibility with locations, dates, and times; options to repeat programs so that more people from different shifts could attend; and scheduling classes during lunchtime or at day's end.
Existing program strengths and resources
Asked what their hospital is doing well to provide palliative care, 71% (n=265) noted strengths. Most common responses concerned providing support to the patient and family. Many believed the small setting of their hospital provided personalized patient attention and care. “We are very small, it is more of a family atmosphere which helps each patient.” Respondents often cited staff as “sensitive and caring,” with an emphasis on the nursing staff, which allowed their facilities to provide a personal touch. Some centers included a team approach as a means to address the palliative care needs of patients; only one hospital had a formal on-call palliative care team.
Approximately 1/5 (22%) of respondents (n=82) had active working relations with hospice programs to address patients' palliative care needs, usually involving referral to hospice services. Few were able to obtain inhouse consults from the local hospice (n=11), described a designated room or “Comfort Care Suite” for end-of-life patients (n=15), used social work services as their palliative care resource (n=14), or noted having their own hospice program (n=5).
Only nine facilities cited pain management as a strength in provision of palliative care services, and one facility utilized an end-of-life order set. No respondents noted formal staff certification training in Hospice and Palliative Medicine; yet two hospitals employed a physician who also served as hospice medical director.
When asked about existing resources that could be utilized to help improve palliative care, many referred to some type of hospice service to help improve palliative care, e.g., providing education to staff and patients and deferring to hospice for advice. Additionally, spiritual care was identified as a common resource, varying from local churches, pastors, ministers, chaplains, spiritual care team, spiritual leaders, to a “Medicine Man.” One provider noted, “Spiritual care is highly sought and provided well but with minimal structure within our hospital.” Thirty-three (9%) respondents looked to home health services as a resource, while just as many (n=32; 9%) noted inadequate or nonexistent resources. Three hospitals reported not needing any resources. “We are a 2000 people community and know exactly how to handle a dying patient.”
Discussion
The major aims of this study were to understand awareness of and familiarity with palliative care, describe palliative care activities currently in place, and identify existing resources that rural hospitals have in providing palliative care. Findings can inform planning a multifaceted intervention to enhance knowledge, skills, and resources for rural palliative care practitioners.
The majority (85%) of respondents were clinically oriented practitioners who reported being familiar with the concept of palliative care. Rural hospitals consistently provided hospice contractual services and advance care planning activities. Fewer hospitals reported having a formal palliative care program, pain service, ethics committees, or employing clinicians with formal palliative care training. Various qualitative comments indicate that there may be confusion distinguishing between palliative care and hospice concepts. These results demonstrate possible areas for targeted program development or educational opportunities to augment somewhat fragmented services.
It is interesting that while only 46% of respondents personally wanted to learn more about palliative care, 80% thought their clinical staff would like to learn more, which presents an opportunity for outreach education to rural hospital staff. Based on reports of current educational activities in their organizations, future educational topics could address end-of-life care issues, symptom management, and communication strategies. Respondents were additionally interested in improving care around ethical issues and psychosocial support to patients and families. This sample preferred online modules and Web-based instruction as educational strategies; these modalities have effectively delivered educational offerings to rural hospitals. 19 The existing relationship with local hospices strongly suggests working with them to assist with palliative care education and services to improve knowledge and care to patients. Local area health education centers offer another avenue for continuing education programs.
Considerations in planning an intervention: Web-based education
As found in our research, multiple barriers often prevent rural health care practitioners from attending traditional conference-based education sessions with live presenters: difficulty accessing programs, lack of time, insufficient workload relief, and competing personal responsibilities. 20 These challenges are consistent with Kortes-Miller's findings and suggest that continuing education programs need to be more accessible, flexible, and affordable. 21 Adapting traditional conference offerings to meet these needs will promote career development for rural-based and isolated health care professionals serving low-income and unique rural populations.
Web-based instruction has potential as a valuable educational tool, as it is available remotely, eliminates travel, and can provide more varied stimulation than traditional lecture-based instruction, which may result in improved attention and retention of material.22–24 Academic institutions have successfully used Web-based instructional techniques to teach evidence-based medicine and practice to health care professionals and postgraduate nurses.22,25–27 The application for Web-based networking and learning has the potential to improve rural palliative care.
Challenges associated with Web-based education often overlap with those associated with traditional conference programs. Lack of time, competing demands at work and home, inadequate computer skills and access, absence of face-to-face interaction, and lack of recognition for Web-based learning have been identified as barriers.22,28 Health care professionals wishing to promote Web-based education will need a plan and support for the use of internet technology.29,30
Large urban hospitals, with successful existing palliative care services, bear the responsibility to provide updated knowledge and information by mentoring rural hospital staff to build a palliative care culture and infrastructure. At the University of Colorado Hospital (UCH), components of such an intervention already exist. For the last seven years, UCH has offered a yearly palliative care symposium to professionals throughout the region, including a research day highlighting a nationally known palliative care researcher. Currently, our palliative care service, in collaboration with School of Medicine faculty, offers weekly Web-based palliative care one-hour educational, research, and networking sessions to interdisciplinary health care professionals from affiliated sites, including rural hospitals. In addition, a Web-based graduate-level palliative nursing class is offered through the University of Colorado, College of Nursing. This three-credit class on complex symptom management focuses on assessment and management strategies including pharmacological and nonpharmacological approaches, physical, psychosocial, and spiritual interventions. Ethical consideration of comfort versus cure, evidence-based palliative care practices, and the advance practice nurse's role are explored. Future intervention development may include using Web-based technology for periodic case consultation rounds, developing a rural hospital palliative care network and online mentoring follow-up, recognizing rural hospitals' limited staff flexibility and resources. In addition, promoting palliative care certification for physicians and nurses in rural hospitals is an important strategy to improve palliative care in rural settings.
Limitations and future research
The 40% response rate may be a limitation and may reflect a selection bias of respondents that results in inadequate knowledge about rural palliative care services and needs or, conversely, only providers interested in palliative care may have responded, thus limiting our findings' generalizability. In addition, while we used a newly developed survey instrument without established reliability and validity, we did ascertain items based on our previous work, expert panel, and literature review. We surveyed both clinicians and hospital administrators; the blending of responses may not adequately represent each worldview or clinicians providing frontline patient care. While the ability of respondents to differentiate palliative care from hospice was not this study's focus, it may have skewed results. Future research should include using our needs assessment survey in other settings and geographical regions.
Conclusions
Rural hospitals demonstrate interest in learning more about palliative care issues for clinical staff. Opportunities for informing rural areas focus around utilizing the existing hospice resources and relationships, and favoring Web-based classes and online self-study modules. These palliative care needs assessment results can be used to inform development of a multifaceted educational intervention in rural settings.
Footnotes
Acknowledgments
Kate Miller, RN, BSN, research assistant, is acknowledged for assistance with data collection and data entry. Funding was provided by the University of Colorado Program in Palliative Care Research Pilot Grants Program.
Author Disclosure Statement
No competing financial interests exist for any of the authors.