
Abstract

Dear Editor:
Palliative literature is replete with written descriptions of how to conduct a family conference in order to elicit goals of care. There is nothing in the literature that specifically describes, in picture form, a method of consultation that is clear, easy to grasp, and that can be used as a prototype to teach other clinicians at either a primary or advanced level.
Dr. Tom Huchinson in his edited book Whole Person Care 1 describes the difference between “curing” and “healing.” Curing involves preserving life and everything that makes up a person's life and is based on medical science where control and power reside with the clinician. Conversely, healing entails an acceptance of changed life, bringing a new wholeness predicated on the inner resources of the patient who is the one in control and with whom the power resides.
In view of Dr. Hutchinson's explanation of “healing,” we considered how we could create a “climate of healing” in every clinical encounter (Fig. 1). For most of us, home is the place where we heal from the assaults of the world. It is the visual model of a house that we use to describe how a “climate of healing” can be established.
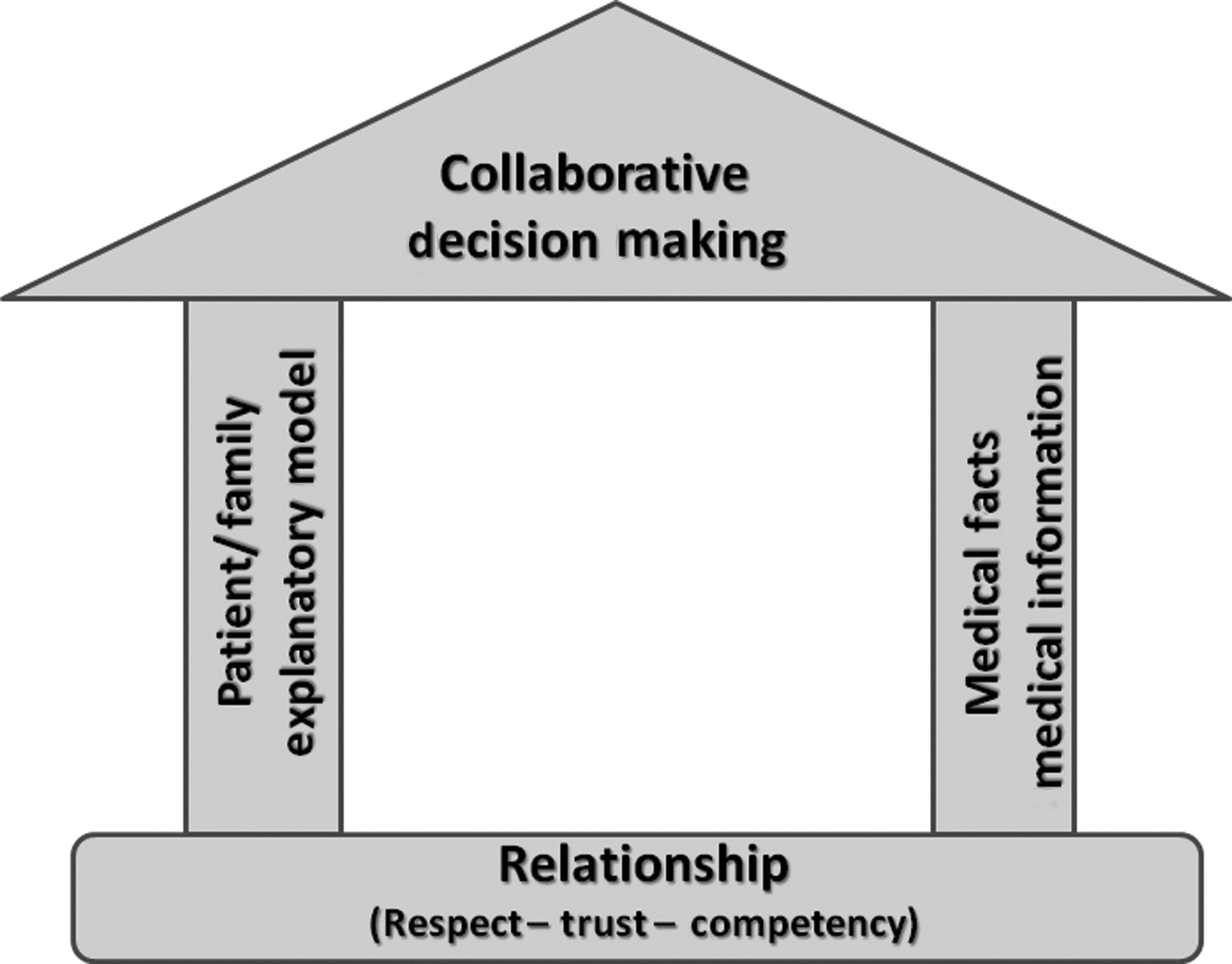
Create a climate of healing.
Every house needs to be built on a robust foundation and that foundation in our model is representative of the crucial need to establish relationship with the patient and family.
The next component of house construction is the framing. The wall to the left represents the patient/family explanatory model of illness. This is where we find out what they have heard from their clinicians regarding their condition and what to expect going forward. It is here that we gain an understanding of how their illness is affecting them not just physically but also emotionally, relationally, and spiritually; what they might be worried about; or what concerns them the most. Careful listening anchors this wall into and builds on the foundation of relationship.
The wall to the right represents the disclosure of medical facts. This needs to match the opposite wall in order to eventually place a roof. If the clinician discovers in the course of building the patient explanatory model wall that medical disclosure is incomplete, then this will need to be addressed.
Finally, the roof, representative of collaborative decision making, can be placed.
In this visual model it is easy to see that without relationship the house will sink. If the “framing” walls of the patient explanatory model and medical disclosure are missing or unequal then the house will give way when attempts are made to place the roof of collaborative decision making. If attempts are made at roof placement while neglecting placement of the foundation or bearing walls, the result will be collapse.
If every component of the house model is robust and built in the correct order, then we can cultivate a climate for healing. We have found this simple, visual model to be effective and have incorporated it into clinician training in both primary and advanced Palliative consultation.