
Abstract
Abstract
Background and Objective:
Even though cancer is the second most common cause of death, little is known about the extent to which family caregivers find meaning and benefit in the loss, and associated demographic characteristics and caregiving experiences. This study addressed this gap in our knowledge.
Design and Subjects:
Family caregivers participated in a nationwide survey for cancer caregivers two years after the relative's diagnosis (T1). Of those, 121 were identified as bereaved by five years postdiagnosis (T2) and provided valid data for the study variables. Participants were primarily middle-aged, spouse of the deceased, and bereaved for an average of 2.9 years.
Measurements:
Perceived caregiving stress, caregiver esteem, and patient's cancer severity as indicators of initial caregiving stressors and caregivers' demographics were measured at T1. Social support and time since bereavement as indicators of current resources and benefit finding in bereavement as an outcome were measured at T2.
Results:
Reports of personal growth from bereavement emerged in multiple domains, although some caregivers were less likely to find benefit: nonspousal caregivers who had greater caregiving stress and spousal caregivers with lack of social support.
Conclusions:
Findings suggest that bereavement programs designed to help bereaved caregivers find meaning in the loss should be personalized reflecting individual differences in caregiving stress and caregiver esteem. Such programs should also be tailored differently for spousal versus nonspousal caregivers.
Introduction
Most studies of benefit finding in the experience of cancer have focused on the patients,5–8 but a few studies have examined benefit finding among family members,9,10 mostly spouses of breast cancer patients assessed while the patients were alive. For example, husbands reported benefit finding one to five years after their wives' breast cancer diagnosis.4,11 Caregivers reported personal growth from providing care to a family member with various types of cancer 12 and other illnesses, such as HIV/AIDS 13 and multiple sclerosis. 14
What happens when caregiving gives way to bereavement? Existing bereavement studies are mostly mixed with regard to cause of death. These studies have found that bereaved family members often search for new hope, meaning, and purpose in life, both in qualitative15–17 and quantitative studies.18–21 Only a few studies examined benefit finding in bereavement focused on cancer caregivers and prospectively investigated the effects of initial caregiving experiences on benefit finding in bereavement, however.
Predictors of benefit finding in bereavement
The main goal of this study was to examine predictors of benefit finding after the relative's death. Both theory 22 and evidence suggest that greater challenges may promote greater benefit finding. For bereaved caregivers, prior caregiving experiences and perceptions about their role as a caregiver represent significant stressors.17,23–24 Thus, it seems plausible that greater earlier caregiving stress—i.e., higher levels of stress from caregiving, lower self-worth as a caregiver, and providing care to recipients whose cancer was more severe—might promote benefit finding in bereavement.
A number of demographics were also examined. Some studies found greater benefit finding linked to younger age4,25 and lower education, 8 though another study found the opposite for education. 7 Another relevant demographic variable is whether the caregiver was the spouse/partner of the patient. Most studies include only spousal/partner caregivers, rendering comparison by spousal status impossible.16,18 In the few studies that have compared, effects of this variable have been inconsistent: greater benefit finding was found among spousal caregivers in some, 26 with others finding no difference by spousal status. 12 Although cancer is more common with older age, because adulthood cancer can occur at any age, spousal status is not a mere proxy for age, which may carry implications independent of age per se that influence the benefit finding in bereavement. We thus examined effects of being a spouse of the cancer patient by comparing with nonspousal (e.g., offspring, parent, sibling, or friends) caregivers.
The perceived availability of social support as a resource has also been related to greater benefit finding in cross-sectional studies of husbands of breast cancer patients, 27 caregivers of persons with cancer, 12 bereaved spouses,20,28 and a variety of others.14,29–30 We thus hypothesized that greater perceived availability of social support would be associated with greater benefit finding in bereavement.
Finally, full apprehension of the loss experience evolves as time proceeds.31–32 Thus, bereaved family members need time to construct the meaning of their care recipients' death. One study found that searching for meaning among bereaved spouses decreased with time. 33 Another study found that positive appraisal of the loss increased with time. 28 Yet another study found no significant effect of time since bereavement. 34 Thus, we explored the role of time since the death in finding benefit in bereavement, testing both linear and quadratic functions of time.
Domains of benefit finding
Benefit finding in response to adversity can occur in diverse ways.7,8,22,35 This was confirmed with respect to cancer caregiving, in reports made by persons while they were providing care two years after diagnosis. 12 Six distinct subdomains of benefit finding emerged in response to cancer caregiving: acceptance, empathy, appreciation, family, positive self-view, and reprioritization. No study to date has tested whether benefit finding in bereavement is multidimensional. Thus, another goal of the present study was to explore whether the multiple domains of benefit finding that emerged during caregiving also emerged as distinct from one another after the death of the care recipient.
Methods
Participants
The National Quality of Life Survey for Caregivers 36 was designed to longitudinally assess the impact of cancer on the quality of life of family members and close friends who were caring for cancer survivors. Caregivers were nominated by the cancer patients for whom they provided care. The patients were identified using multiple-state cancer registries as diagnosed with one of the 10 most common cancers. 37 Caregivers were adult family or family-like individuals who provided consistent help during a patient's cancer experience. Eligibility criteria for participating in the caregiver study were (1) 18 years and older, (2) able to speak/read English or Spanish, and (3) residing in the United States.
At caregivers' initial assessment (T1: n=1634), patients were 2.2 years (SD=0.6 years) postdiagnosis. Follow-up data collection 38 at five years postdiagnosis (T2) included a survey designed for caregivers whose index patient had passed away by T2. A total of 179 caregivers were identified as bereaved at T2. Of those, 121 provided valid data for study variables, which were used in subsequent analyses. Caregivers who provided complete information for the study variables did not differ from those with incomplete data (p>0.10), with two exceptions: Completers had been bereaved for a longer period of time (t=2.42, p<0.02) and were more likely to be females (χ2=21.27, p<0.001) than incompleters. Characteristics of caregivers with complete information are reported in Table 1.
Procedure
This study was conducted in compliance with the regulations of the Emory University institutional review board. A packet containing an introductory letter, T2 Main Survey (MS), self-addressed stamped envelope, and a $10 gift card as an incentive was mailed to the sample of nominated family caregivers who completed T1. The T2 MS included an item to identify bereaved caregivers. Caregivers who responded “no” to the question, “Is [patient's name] alive?” received the Bereaved Caregiver Survey replacing the T2 MS. Returning the completed survey served as evidence of informed consent to participate. Two cycles of mailing and telephone follow-up calls were made during an eight-week data collection period corresponding to each time point.
Measures
Initial caregiving stressors
Three measures served to capture caregiving experience at T1. First, the extent to which caregivers felt overwhelmed by tasks and responsibilities was assessed by the four-item stress overload subscale of the Pearlin Stress Scale (1=not-at-all, 4=completely). 39 Higher mean scores reflect greater stress from providing care to the cancer patient. This scale had been validated in samples of caregivers for frail elders and patients with Alzheimer's disease 39 and had acceptable internal consistency in the present study (α=.85).
Second, the extent to which caregiving imparts self-esteem was measured by the seven-item caregiver's esteem subscale of the Caregiver Reaction Assessment (1=strongly disagree, 5=strongly agree). 40 Higher mean scores reflect greater sense of value and worth as a caregiver. The subscale had been validated in diverse samples of caregivers 40 and had acceptable internal consistency in our study population (α=.80).
Third, a severity index of the care recipients' cancer was created for each patient based on the mortality rate calculated by type and stage of cancer and the time since diagnosis.41–42 Information about cancer type; stage (localized, regional, or distant); and date of diagnosis was obtained from the state cancer registry. This index, ranging from 0 to 1, served as an indicator of the patient' cancer severity that is comparable across the 10 most common cancers and different stages of cancer at the time of diagnosis. For example, the cancer severity index for localized prostate cancer diagnosed 2.5 years ago is 0, whereas the index for localized lung cancer diagnosed 2.5 years ago is 0.40 and that of distant lung cancer diagnosed 2.5 years ago is 0.94. Higher scores reflect a more fatal cancer diagnosis and therefore greater caregiving strain.
Caregivers' demographics
Age, gender, education, and familial relationship to the patient were self-reported at T1.
Current resources
Two measures assessed concurrent resources at T2. First, the extent to which the bereaved caregivers perceived that emotional, informational, and instrumental support were available to them was measured, using the Interpersonal Support Evaluation List (ISEL: 1=definitely false, 4=definitely true). 43 The mean of the six items represents the level of perceived availability of social support. This scale had been validated in other caregiver populations 44 and had acceptable internal consistency in the present study (α=.82). Second, caregivers' self-reported date of their bereavement was used to calculate the time between the death and caregivers' T2 survey completion date. Longer time reflects greater concurrent resources.
Benefit finding
The degree to which family caregivers find meaning and experience personal growth from the loss of their care recipient was measured at T2 using the modified 17-item Benefit Finding Scale for bereaved family caregivers. 12 Caregivers were instructed to rate how much they agreed with each item in response to the statement that begins with “Having lost [patient's name] to cancer has..,” using a five-point Likert-style format (1=not-at-all, 5=extremely). This scale had been validated in samples of cancer survivors 6 and family caregivers. 12 The six-domain composite scores had acceptable internal consistency (0.68≤α≤0.84). Each domain score was created by averaging responses to the items contributing to that domain.
Results
Domains of benefit finding in bereavement
First we tested whether the factor structure of the Benefit Finding Scale found in cancer caregivers 12 would be confirmed with bereaved caregivers. Confirmatory factor analysis was performed using structural equation modeling with the 17 items as manifest variables (AMOS 19). 45 The six-factor model fit the data satisfactorily: χ2(95)=135.94, Comparative Fit Index (CFI)=0.958, Root Mean Square Error of Approximation (RMSEA)=0.061, and Standardized Root Mean Residual (SRMR)=.060. All items loaded on the expected primary benefit finding domains (βs>0.53, ps<0.001). Thus, we kept the same labels for the six domains (see Table 2). The six domains were correlated with each other, ranging from r=0.42 between acceptance and empathy, to r=0.87, between appreciation and reprioritization.
Predictors of benefit finding in bereavement
General linear models predicting the six domains of benefit finding simultaneously by initial caregiving stressors, caregivers' demographics, and current resources were conducted. As shown in Table 3, greater initial caregiving stress was associated with greater reports of feeling close to family and reprioritizing values after the loss. Caregivers who felt worthy as caregiver while they were carrying out the caregiver role also reported greater reprioritization after the loss. Among caregivers' demographics, both older age and higher education independently predicted greater appreciation of life and positive self-view, and older age also predicted more reprioritizing of values after the bereavement. Finally, spousal caregivers were more likely than nonspousal caregivers to accept what had happened, appreciate life, increase positive self-view, and reprioritize values in life from their bereavement experience.
†p<.08; *p<.05; **p<.01; ***p<.001.
Gender: Female=1, Male=0; Education: Greater than high school=1, Less than college=0; Spouse: Spouse=1, Nonspouse=0;
Time_linear=linear effect of time since bereavement; Time_quadratic=quadratic effect of time since bereavement.
Bereaved caregivers' current perception of the social support available to them was a strong and consistent predictor of all the subdomains of benefit finding in bereavement except the empathy subdomain. Two aspects of benefit finding (empathy and family) were related to time since the death in both linear and quadratic patterns (see Figure 1). Caregivers who were only recently bereaved (during the first year of bereavement) were the most likely to report elevated empathy for other people and valuing the surviving family members; these fell to their lowest levels one to three years after the loss and rose somewhat again about four years after the loss.
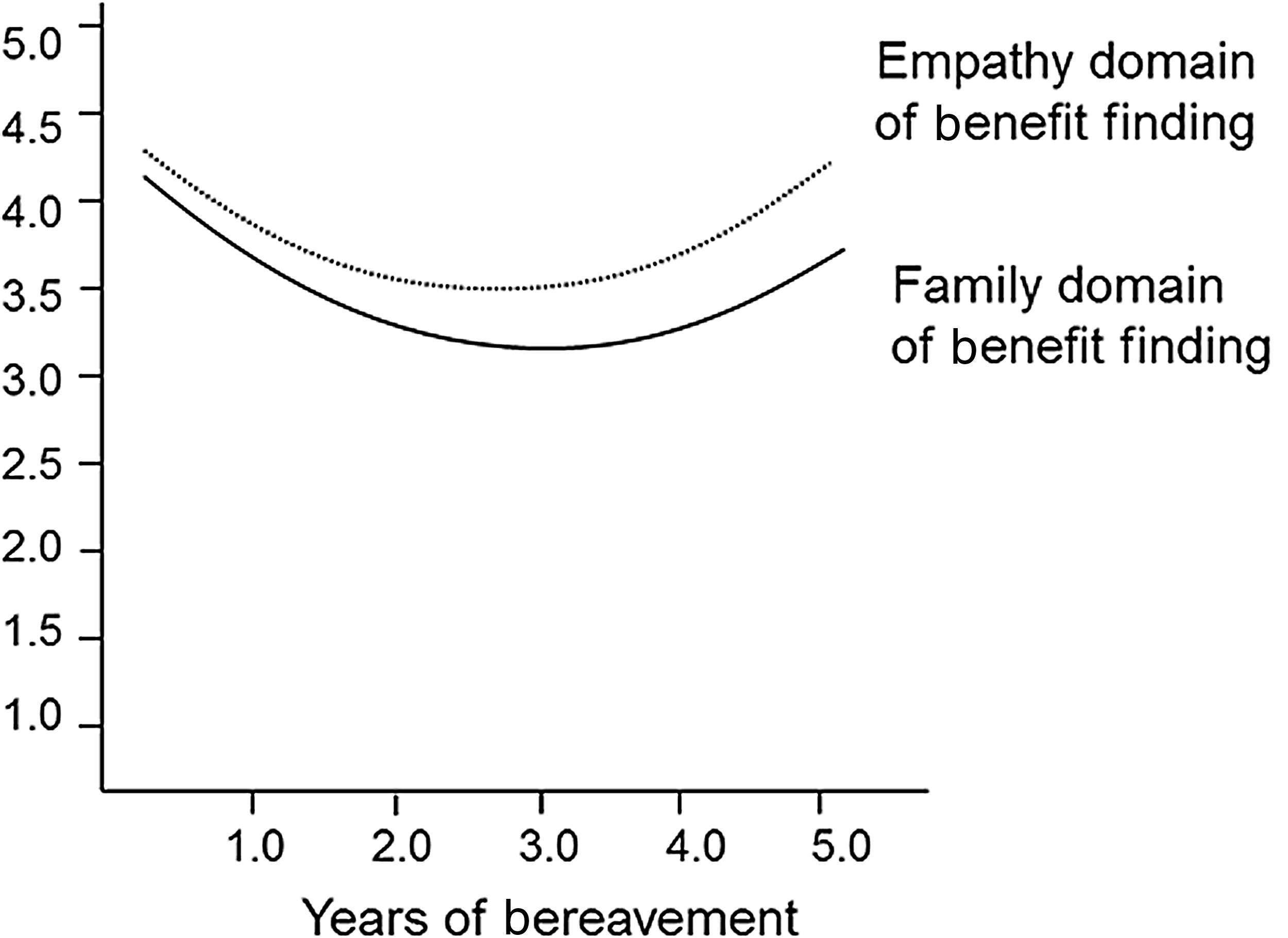
Quadratic effect of time since bereavement on empathy and family domains of benefit finding.
In the second model reported in Table 3 (Interaction Effects block), interaction effects were added. Three interaction effects were significant or marginally significant. The interaction effect between spousal status and caregiving stress on empathy took the following form: initial caregiving stress was not significantly related to subsequent empathy among bereaved spousal caregivers (b=0.20, p=0.22), whereas initial caregiving stress related inversely to subsequent empathy among bereaved nonspousal caregivers (b=-0.32, p=0.05; see Figure 2). A (marginally significant) spouse by caregiving stress interaction on positive self-view reflected a positive association between initial caregiving stress and subsequent positive self-view among spousal caregivers (b=0.33, p=0.04), whereas the association was not significant among nonspousal caregivers (b=-0.10, p=0.53). A similar pattern was found in the spouse by current social support interaction on empathy, which showed a positive association between current social support and empathy among spousal caregivers (b=0.52, p=.008), and a nonsignificant association among nonspousal caregivers (b=-0.06, p=0.74; see Figure 3).

Interaction between caregiving stress and spousal status on the empathy domain of benefit finding.

Interaction between current social support and spousal status on the empathy domain of benefit finding.
Discussion
Benefit finding in bereavement
The six domains of benefit finding observed among cancer caregivers regarding their caregiving activities 12 were confirmed with bereaved cancer caregivers. This supports the multifaceted character of benefit finding in bereavement as in other stressful circumstances. In addition, the degree to which our bereaved caregivers reported benefit finding was comparable to what was reported among nonbereaved caregivers. 12 The findings provide further evidence that family members who confront the challenge of cancer in the family—this time, the loss to cancer—also can gain a sense of personal strengths and new possibilities through the experience.
Predictors of benefit finding in bereavement
The stressors and resources we examined predicted benefit finding in bereavement in distinct ways. Initial perceived caregiving stress was a significant predictor of elevations in two domains of benefit finding: family and reprioritization. This result supports Tedeschi and Calhoun's 22 position that stress must be severe in order to prompt benefit finding. This is also consistent with other results.5,7–8,12 Initial caregiver esteem, however, was also a significant positive predictor of reprioritization, contradicting our hypothesis. It appears that greater challenges that the caregiver had to face while providing care9,10 brings the family closer together by the time the challenge ends with the death of the care recipient. On the other hand, both the greater challenge of the event and the greater sense of competence of the person facing the challenge seem to enable the person to reevaluate circumstances and reorganize priorities after ceasing the role that was the source of both challenge and competence.
Compared with nonspousal caregivers, spouses were more likely to report accepting the death of the care recipient, newly appreciate relationships with others, make positive changes in their self-view, and reprioritize their values in life. Initial caregiving stress also led spousal caregivers to endorse more-positive self-views, whereas it led nonspousal caregivers to become less empathic after the bereavement. These effects differed by spousal status of the caregiver, which might be attributable to different types of care tasks carried out by the two groups of caregivers. For example, spousal caregivers are more likely than other caregivers to be involved not only in providing instrumental care, assisting the care recipient with activities of daily living (e.g., dressing) and instrumental activities of daily living (e.g., housework), 24 but also providing emotional support, easing the psychological distress caused by cancer. 46 Elevated stress from such close involvement in caregiving might stimulate the process of finding meaning in the death of care recipient.
On the other hand, the caregiving stress among nonspousal caregivers, particularly adult offspring, might be attributable to their carrying out multiple social roles, as the so-called sandwich generation often does in addition to cancer caregiving per se. 47 The death might also have different implications to parents, offspring, and siblings due to their shared biological vulnerability with the deceased. If these various social roles and existential concerns were competing for limited resources, it might in turn dilute the possibility of nonspousal caregivers finding benefit in the loss experience.
It is also noteworthy that perceived availability of social support was a consistent and strong predictor of benefit finding. This is consistent with the literature and supports the view that social support is a critical component of growth following major life experiences.4,12,30,48 Our finding that social support leads bereaved caregivers to greater empathy only among spousal caregivers further suggests that social support is more beneficial to certain subgroups of caregivers. This should be taken into consideration when designing targeted programs.
Another novel finding is that time since the death related to two benefit finding domains in curvilinear patterns. Those who were bereaved reported varying levels over time of empathy for other people and valuing the surviving family members. These were at their lowest levels one to three years after the loss and were higher about less than one year or four years after the loss. The findings suggest that personal growth from bereavement, specifically pertaining to relatedness, is an evolving process that requires time. Former family caregivers whose care recipient died a couple of years ago might benefit from programs designed to facilitate their regaining the sense of relatedness with others.
Limitations and directions for future studies
Several limitations of the present study should be noted. All variables in this study were self-reported and therefore may be affected by social desirability, response shift, 49 or defensive reactions. 50 Each family member or close friend experiences different levels and kinds of stress from the cancer of the loved one and has different coping resources available. Current findings should be replicated in future studies that include multiple family members. Investigating psychological, behavioral, and physical correlates of benefit finding in bereavement may provide important information about how finding meaning in loss would influence mental and physical health of the bereave family members. It will also be important to replicate these findings with ethnic minorities and individuals of lower socioeconomic status.
Conclusion
The findings add significant information to a growing body of research on family caregivers of individuals with cancer. Many family members face the death of the relative with cancer within five years postdiagnosis. Personal growth experiences from bereavement emerged in multiple domains, although nonspousal caregivers who had greater caregiving stress and spousal caregivers with lack of social support were less likely to find benefit in bereavement. These findings suggest that programs designed to help bereaved caregivers find meaning in the loss should be personalized, reflecting individual differences in caregiving stress and caregiver esteem. Such programs should also be tailored differently for spousal versus nonspousal caregivers.
Footnotes
Acknowledgments
The authors thank Chiew Kwei Kaw for data management and extend their appreciation to all the families who participated in this investigation. The first author dedicates this research to the memory of Heekyoung Kim. This study was supported by the American Cancer Society National Home Office, intramural research.
Author Disclosure Statement
None of the authors have financial conflict of interest to disclose.