
Abstract
Abstract
Background:
Polypharmacy and drug omissions (DO) (i.e., drugs prescribed but not administered) may impact on quality of life of hospice inpatients.
Aim:
The study's objective was to assess for polypharmacy and DO across hospice inpatient units in Northern Ireland (NI).
Design:
A retrospective chart review of consecutive admissions to five adult hospices in NI in 2011–2012 was performed. Only regularly prescribed oral and nebulized medications were analyzed.
Results:
Inpatient admissions (n=138) were reviewed (58% male, median age 68, 91% had cancer). The average number of regularly prescribed medications was eight (range 0–17) on admission, 10 (1–21) at discharge, and two (0–15) at time of death. Of all prescribed doses, 8.8% were omitted. The most frequent DOs were laxatives (38%), mouth care (11%), and mineral supplements (9%). Reasons for DO included patient refusal (46%), patient asleep or drowsy (20%), and drug not available (7%). DOs numbering 197 lasted 24 to 72 hours. No action was taken by medical staff for 79% of these. DOs numbering 85 lasted over 72 hours. While fewer drug doses were prescribed for patients who died during admission, the proportion of DO was higher (12.4%) than for those discharged (6.9%). DO increased in the last week of life (23%).
Conclusions:
Polypharmacy is prevalent among hospice inpatients. Drugs omitted amounted to 8.8%, with the frequency of DO increasing in those who were dying. Documentation justifying DO was lacking. Daily focused drug chart review, pharmacy support, and electronic prescribing may all help to reduce and rationalize medication burden and aid prompt and effective management of DO.
Background
UK hospitals hit the headlines in 2011 when it was reported that an estimated one in five prescribed drugs were not being administered to patients. 3 Omitted and delayed medications were the second largest cause of medication incidents reported to the National Patient Safety Agency in 2007, and have been shown to occur in up to 20% of secondary care admissions.4,5 Very little is known about the prevalence of DO in the hospice context, nor the impact of these omissions on patient care. A pilot study suggests that DOs are the most common form of drug error. 6 DO may occur for a variety of reasons in a hospice setting and may well be justifiable and in the patient's best interest. However omitting or delaying some medications in hospice patients may result in actual or potential harm. It is important that reasons for DO are clear, appropriate, and documented by those omitting the medication, to allow the medications to be reviewed and action to be taken promptly when necessary.
The purpose of this study was to assess both polypharmacy and DO across five hospices in Northern Ireland (NI). It aimed to quantify the level of polypharmacy by determining the number of regular medications prescribed for patients on the day of admission and how this compared with the number of medications on discharge. Additionally, it aimed to evaluate how prescribing patterns change during admission, particularly as death approaches, and to determine the frequency, nature of, and reason for DO, and identify if these were causing issues in patient care.
Methods
A retrospective chart review of consecutive admissions to five adult hospices in NI in 2011–2012 was performed. A pro forma was used to record the number of regularly prescribed medications, number of and reasons for DO, DO lasting longer than 24 hours, classification of omitted drugs, and DO in the last week of life. Only regularly prescribed oral and nebulized medications were included.
Results
Clinical notes for 138 inpatient admissions were reviewed (80 males, 58 females) across the five hospice sites (range 17–35 per site), and all were included in the analysis. The median age was 68 years (range 20–93), and 91% of patients had a diagnosis of malignancy. A total of 2377 admission days were assessed and the median duration of admission was 14 days (range 1–104). In total, 68 (49%) of surveyed patients died during the assessed admission. The average number of regularly prescribed oral and nebulized medications at the time of admission was eight (range 0–17) (see Figure 1). This increased to 10 (range 1–21) at the time of discharge, but reduced to two (range 0–15) at the time of death for those patients who died during the admission.
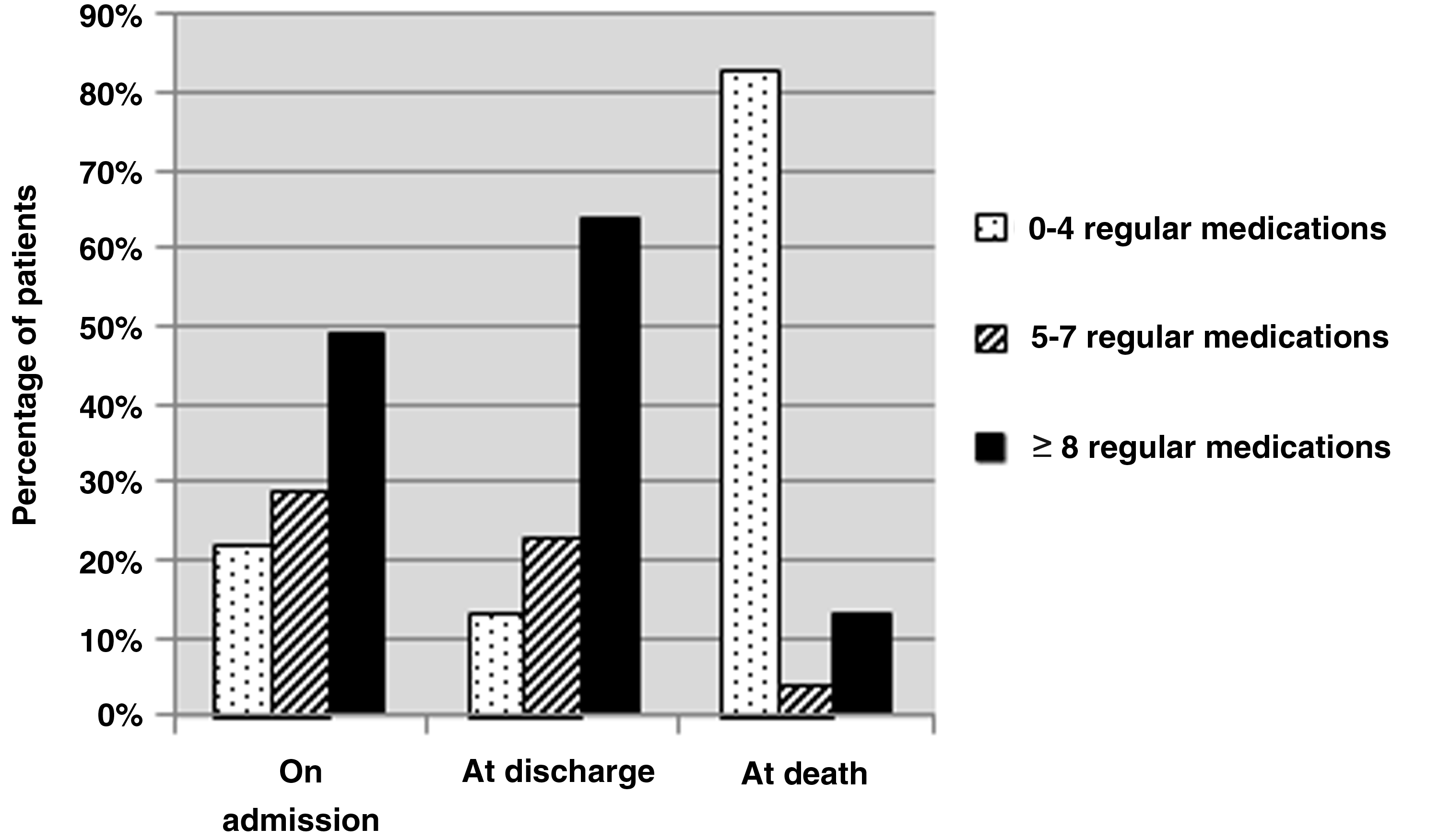
Number of regularly prescribed medications per patient.
From a total of 35,575 doses prescribed for 138 inpatient admissions, there were 3129 omitted doses (8.8% of all doses prescribed). On average, 6.9% of medications were omitted for patients who proceeded to be discharged from the hospice. This compares to an average of 12.4% of DO for patients who subsequently died during that admission. Further analysis of DO in the last week of life demonstrated that on average, 23% of regularly prescribed medications were omitted. The reasons for DO were documented on the medication kardex by nursing staff in 88% of cases and are demonstrated in Figure 2. The classification of omitted drugs is demonstrated in Figure 3.

Documented reasons for drug omissions.
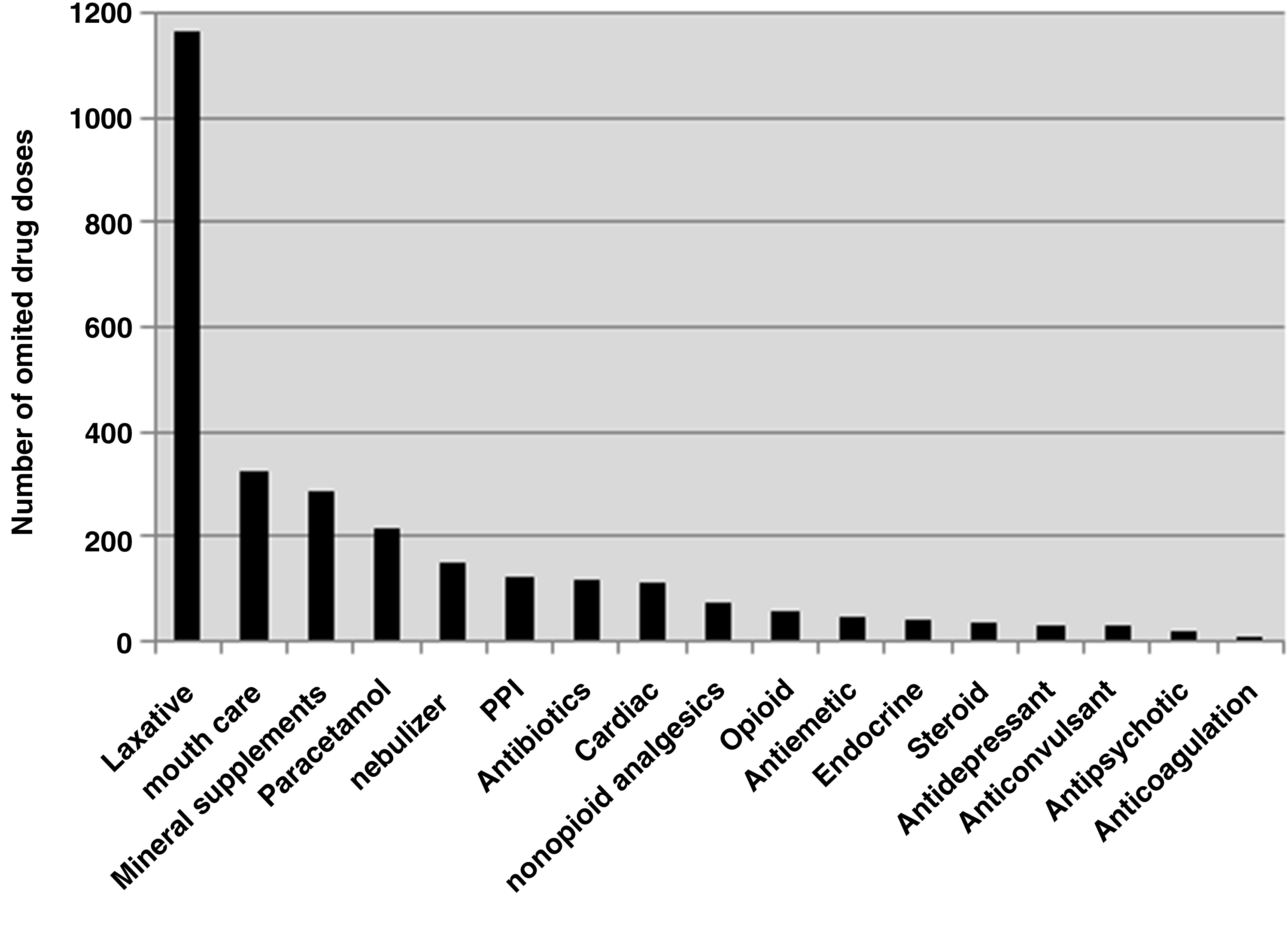
Number of omitted drug doses by drug classification.
There were 197 DOs lasting between 24 and 72 hours. No action was taken by medical staff for 156 of these (79%). There were 85 DOs lasting longer than 72 hours. No action was taken in 51 (60%) of these instances. There was no documented recognition by medical staff for 52% of prolonged DO. On review of all DOs, four were felt to be clinically significant in relation to the patient's current symptoms and disease. These included omission of an oral PPI within 24 hours of significant hematemesis, an antiepileptic medication omitted for more than 24 hours as it was not available on the ward, steroid nebules not being available on the ward for a patient with COPD who was significantly short of breath, and verapamil not being available for a patient with fast atrial fibrillation.
Discussion
Palliative care aims to optimize symptom control and maximize comfort in individuals with limited prognoses. Polypharmacy may arise as a consequence of trying to achieve these goals, but may itself adversely affect the quality of life of the individual patient and be potentially harmful through drug interactions, adverse effects, and medication burden.2,7,8 It may also increase health care costs.2,7
In this study, polypharmacy was an issue for patients admitted to hospices in NI. Of patients at admission, 78%, and of patients at discharge, 87% were prescribed five or more regular oral or nebulized medications. This does not account for regular medications that may have been administered parenterally. Due to the complexity of the patients who are referred for inpatient management in hospices, multiple medications are often required to control symptoms and polypharmacy may be unavoidable.
At time of death, the average number of regularly prescribed oral or nebulized medications was reduced to two (range 0–15). This reduction may have been a consequence of a change in the route of administration or appropriate discontinuation. A breakdown of the actual medications still prescribed at the time of death would be useful. This was not included in the data collection and is a limitation of the study.
In view of the problems associated with polypharmacy, steps should be taken to regularly review the need for and benefit from all prescribed medications in the palliative care setting, such as lipid lowering drugs and vitamin and mineral supplements. The development of guidelines relating to the discontinuation of long-term medications at an appropriate stage in a patient's illness would be useful.
As discussed previously, DOs are one of the most frequent medication errors in the hospital setting.4,9,10 In this study, the average frequency of medication omissions varied between 6.9% in those who were subsequently discharged to 23% in the last week of life. For over 24 hours, 282 drugs were omitted, with 85 of these omissions lasting longer than 72 hours. The majority of prolonged omissions were not acted upon by medical staff and had no documentation in the medical notes to acknowledge that patients had missed medication doses. To ensure patient safety, medical staff need to be alerted to any DO, and in turn, medical staff need to be aware of the importance of actively seeking this information.
The most common reason for drug omission was patient refusal (46%) (see Figure 2). If patients are found to be refusing medications, the reason for this should be sought and discussed with the patient to determine if their decision is appropriate. The second most common reason for omission was ‘patient asleep or drowsy’ (19%). In the hospice setting, patients may be asleep at the time of a medication round. In this study there was no indication that medications were offered at a later time and it may be prudent to have a system in place enabling this.
The most commonly omitted drugs were laxatives (38%) (see Figure 3). Frequently, the reason documented for this was ‘loose stools.’ It may be appropriate to omit laxatives for a short time if a patient has diarrhea or increased stool frequency. However, patients with overflow diarrhea may have their laxative medications inappropriately omitted. For many patients on regular opioid medication, constipation can be an ongoing problem and therefore laxative therapy often needs to be continued, but may require adjustment.
Conclusion
Polypharmacy is prevalent among hospice inpatients. Medical staff should be proactive in reviewing the need for all medications to reduce this, particularly long-term preventative medications. Just under 1 in 10 prescribed drugs were not administered to patients in the assessed hospices. These DOs occurred for a variety of reasons. Robust documentation was found to be lacking in relation to explanations for this. Patient safety may be at risk, and although it may be difficult to eradicate DO, mechanisms should be put in place to reduce the frequency of inappropriate omissions. Nursing staff need to highlight DO to medical staff, who should then review these daily and take action when appropriate. Improving prescribing practices in hospices should result in improved patient care, a reduction in wasted costly drugs, and more proactive and patient centered symptom management.
Footnotes
Acknowledgments
We would like to acknowledge the support of Drs. Tracy Anderson, Laurence Dorman, Yvonne Duff, Joan Fyvie, Eilis Hope, Mary Mackle, Noel McElvanna, Paul McIvor, Conor McRory, Mary Quinn, and Pauline Wilkinson, who all helped in the data collection for this study, and Dr. Jenny Doherty, as chair of the NI regional audit committee, for her support.
Author Disclosure Statement
No competing financial interest exist.