
Abstract
Abstract
Background:
Moral distress is a pervasive reality of palliative care practice. An existing framework for understanding it has been proposed as a way to begin to address moral distress's detrimental effects on clinicians.
Objective:
The objective was to illustrate the application of this adapted conceptual framework to a clinical case and to offer recommendations for enlarging the professional repertoire for responding to challenging cases involving moral distress.
Analysis:
In the clinical case, clinicians are expected to respond to the patient's suffering based on four factors: empathy (emotional attunement), perspective taking (cognitive attunement), memory (personal experience), and moral sensitivity (ethical attunement). Each of these interrelated and iterative factors may become activated as clinicians care for patients with life-limiting conditions. This creates the foundations for clinicians' responses. When responses risk becoming aversive in the face of moral dilemmas, strategies are needed to foster principled compassion instead of unregulated moral outrage. A number of cognitive, attentional, affective, and somatic approaches derived from contemplative traditions are consistent with the framework. Combined with a systems-focused approach that incorporates organizational factors, they offer a means of improving professional repertoires for responding to difficult situations.
Conclusion:
Application of the proposed framework to a clinical case provides opportunities for understanding mechanisms of response that may be amenable to intervention and for suggesting appropriate alternative strategies and practices. A full understanding of the process can help to mitigate or to avoid the progression of distress and concurrently to appraise the situation that leads to moral distress or moral outrage.
Introduction
A Framework for Understanding Moral Distress
The proposed framework 11 (see Figure 1) addresses the effects of moral distress on clinicians. To illustrate this framework we relate it to a clinical case (see Table 1) and postulate how components might unfold in clinical practice. Using the case of Maria, we theorize how clinicians might respond to her suffering based on four antecedent factors: empathy (emotional attunement), perspective taking (cognitive attunement), memory (personal experience), and moral sensitivity (ethical attunement). 11 Although the process may appear linear, these aspects of appraisal are seen as interrelated and iterative, each triggering event initiating another response chain. An imbalance in any could cause destabilization and lead to self-focused behaviors, such as moral outrage, avoidance/abandonment, or numbness. Each of these factors can be activated as clinicians care for patients with life limiting conditions, creating the bases for adverse reactions. This framework will be applied to Maria's case, with recommendations on how it can be used to reduce the detrimental effects of moral distress.
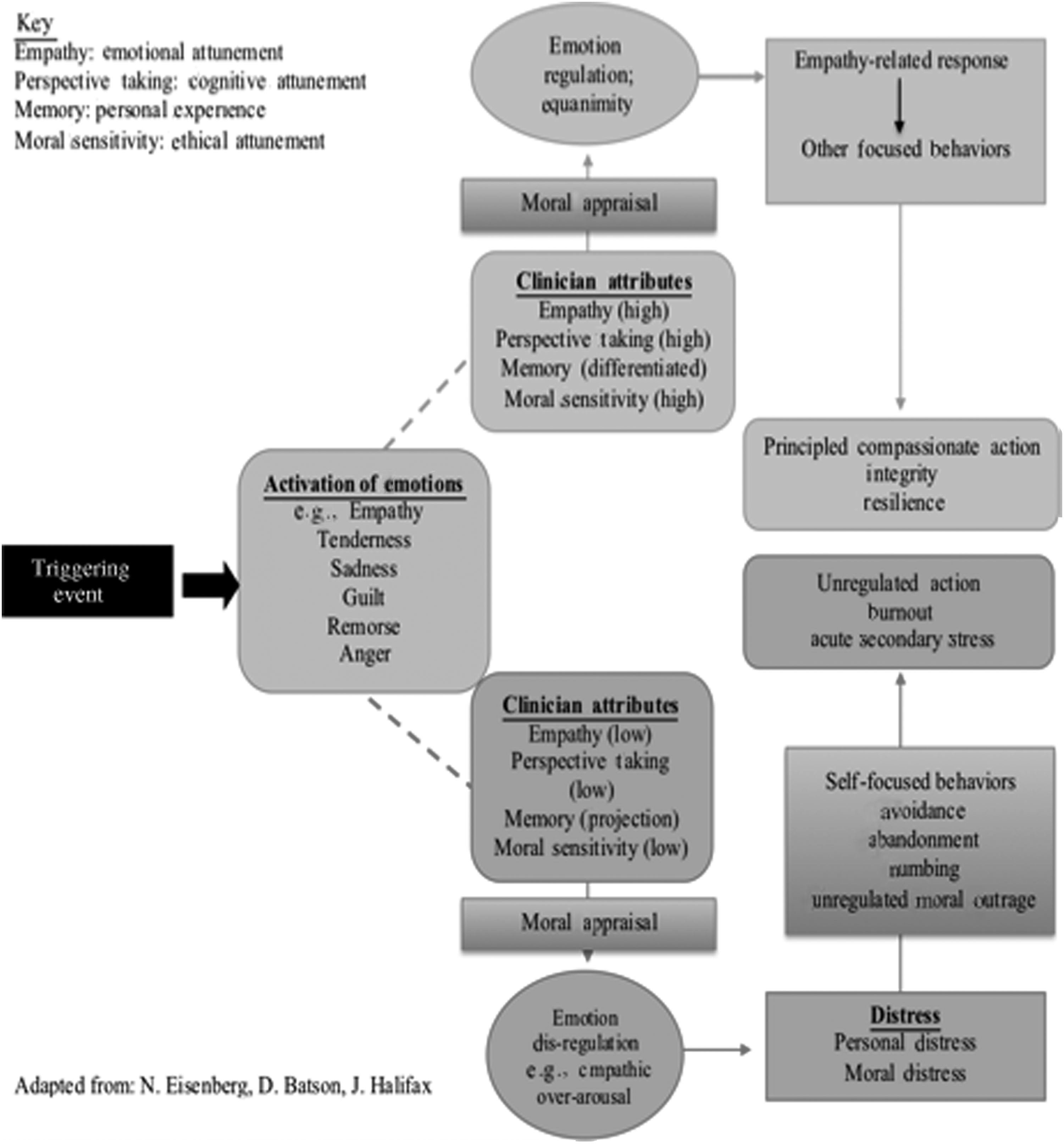
A framework for addressing moral distress. 11
Based on a clinical case; identifying data altered to protect privacy.
Empathy
Empathy, an affective process, was likely aroused in relation to Maria's suffering. Caring for her physiologic, emotional, and spiritual needs may be motivated by an intention to realize a balance between short-term burdens and the longer-term goal of survival with a desirable quality of life. Actions to care for Maria likely arose from the clinicians' empathic concern for her well-being and their professional commitment to alleviate suffering. Healthy modulated affective arousal from witnessing Maria's responses to treatment may have allowed empathic concern to arise. At such a juncture, care could be provided with integrity if there was congruence and understanding about care, goals, and treatment plan.
Central to cultivating modulated empathy and principled compassion is the capacity to differentiate self from other. 14 When clinicians see Maria's suffering as separate from their own they can regulate their arousal so it remains in a zone of resilience, rather than becoming overwhelming.15,16 When there is a clear recognition that the patient's suffering is not their own, and there is empathic resonance, clinicians may be able to enter Maria's world and remain personally and professionally grounded. 17
As Maria's condition deteriorated, however, clinicians may have questioned actions that they perceive as causing harm. 18 For example, a nurse may not be able to witness Maria's suffering with healthy empathy. Despite cognitively understanding the patient's and family's goals, a nurse may find it challenging to respond with balanced emotional attunement; this internal processing can be exacerbated by cumulative stress associated with Maria's care; the depletion of physical, emotional, and spiritual resources over the patient's long hospitalization; and the moral dissonance associated with competing values and commitments.18,19
No longer able to see Maria's suffering as justified, clinicians may have shifted to a self-focused response based on a negative appraisal of the situation and characterized by empathic overarousal and aversion, 17 thus turning away from the patient in response to their own distress. Increasing reports of physical symptoms such as headaches, nausea, and generalized feelings of fatigue and overall depletion, particularly by nurses, may reflect autonomic arousal and give clues about the negative impact of moral distress. Refusing to provide care, not wanting to go into the patient's room; expressing revulsion at participating in treatments perceived as harmful; and feelings of numbness, despair, and regret—all can be indicators of the aversion often born of empathic overarousal typical of clinicians who find themselves in a moral bind or dilemma.18,20,21
When the boundaries between self and other blur it becomes difficult to separate the suffering of the other from one's own. As Maria's condition worsened, the integrity of her body began to erode; and decubitus ulcers, nonhealing wounds, and ischemia gave evidence of her decline. Coupled with the facial expressions, body language, mute cries, and mouthed requests to relieve her pain, the physical decline may have ignited an attunement between her suffering and feelings of despair, personal distress, and moral outrage in some of the clinicians caring for Maria.17,18,21
Perspective taking
Perspective taking or cognitive attunement involves the ability to understand and appreciate the unique vantage points of others. Aggressive interventions to treat Maria's physiologic and emotional needs may have been motivated by the patient, family, and health care team's alignment about the goals of care and the values informing decisions. This attunement would have allowed the team to perceive their efforts as aimed at an achievable and ethically based goal to preserve life when recovery was possible. The congruence between the team's goals and those of the patient and family may have contributed to compassion-based responses.
As Maria's condition declined, no longer was there congruence in goals and values between patient, family, and team. First, Maria's husband Tom, as the patient's health care agent, prioritized doing “everything possible” to sustain her life as the primary goal of her care, despite mounting complications and diminished quality of life. Clinicians may have interpreted Maria's condition as irreversible, and perceived their efforts to sustain her life as unjustifiably burdensome, causing undue pain and suffering, and prolonging an inevitable death. There may have been differing interpretations of Maria's preferences for treatment, quality of life, or end-of-life care. Clinicians likely experienced dissonance between scientific evidence, assessments of prognosis, and her husband's request to continue despite the progression of Maria's disease process. 19
Second, Tom believed that the best way to support Maria's progress was by minimizing sedation, maximizing mobility, and enhancing awareness and engagement with her family. For Tom, Maria's suffering was justified as facilitating her relational capacity and recovery. This may have widened the gap in alignment of goals between the husband and the health care team. Clinicians who did not agree with his perspective may have reasoned that the most compassionate action would be to alleviate her pain and suffering to the fullest extent possible.22,23 This, coupled with their primary ethical mandate to “first do no harm,” may have fueled their moral distress.
Third, Maria's decisional capacity was uncertain, making it difficult to determine what she would have chosen had she been able to speak for herself. Prior to surgery Maria was clear that she wanted to live as long as possible, independently, with better quality of life. As her health declined, clinicians interpreted her physical expressions of pain and suffering, coupled with attempts to mouth words suggesting that she did not want to live in her current condition, as evidence that continued treatment was not in her best interest. The situation was complicated by a diagnosis of depression, and Tom's perspective on the impact on Maria's will to live and her ability to engage of clinical strategies for managing pain and anxiety. 24 Guided by a commitment to honor patient autonomy, clinicians may have perceived that their actions were disrespectful of Maria's choices. As her capacity to communicate and discern became intermittent, the gap between what her husband was requesting and what the team understood to be morally correct widened, contributing to cumulative moral distress.
Finally, the perspectives of various team members are also morally relevant. Nurses providing direct and round-the-clock care for Maria were likely different from the physicians who provided intermittent care. The surgeon who initiated the transplant may have experienced a heightened level of responsibility for the outcome and perceived an imperative to give her “every chance to live.”25,26 In contrast, the nurses may have perceived their efforts as more harmful than beneficial, undermining their ethical mandate to relieve suffering.8,27 Lack of understanding of differing perspectives and efforts can contribute to an exacerbation of both personal and moral distress. These and other factors may have contributed to the incongruence in goals and erosion of client and team relationships.21,28
Memory
Conscious and unconscious memories inform a clinician's responses in cases like Maria's. Memory includes personal and professional experiences, cultural or societal experiences, and differences in physiologic and emotional responses. 29 Core values, personal and familial history, and professional culture also impact what individuals bring to caregiving. If memories are positive and prior professional experiences have led to a sense of self-efficacy, arousal may evoke a positive emotional response, resulting in regulated altruistic behavior 30 and leading to compassionate and integrity-preserving action. Clinicians who are able to maintain a state of emotional neutrality and/or positive orientation may be less likely to experience a high intensity of moral distress, even if they perceive a conflict in values or do not agree with the treatment plan. 31
In contrast, clinicians who have had repeated professional experiences with cases like Maria's may have developed negative or unconscious response patterns influencing how they appraise and act. Unrecognized or unprocessed grief, or unconscious identification with the patient's situation because of age or contextual features, can impact one's appraisal and response to the case. Maria's disease progression may have reminded a clinician of similar experiences with other patients or family members, arousing grief or regrets about how these situations were handled. 29 Repeated unresolved or negative experiences with similar cases involving situations of “futility,” moral distress, or moral dilemmas that were refractory to negotiation or mediation can contribute to negative appraisal.8,20 Eisenberg 32 suggests that if unconscious negative memory is overly activated, responses to the situation are more likely to be self-focused, causing empathic overarousal, vicarious or secondary stress, or personal distress. The cumulative impact of repeated experiences of moral distress may leave a “moral residue” that alters the ability of clinicians to return to a baseline of well-being and stability and creates a “crescendo” effect with each subsequent exposure. 9
Moral sensitivity
Being ethically attuned is foundational to recognizing ethical conflicts and the obligation to respond to them. Becoming aware of an ethical problem involves both conscious and unconscious processes. Being aware of and trusting one's intuition in the face of conflicting ethical commitments or unethical behavior can cultivate moral sensitivity. The ability to locate and articulate the source of internal discontent helps the clinician imagine possible courses of action and their consequences. When a clinician recognizes that a patient is in distress, a regulated empathic response may create the awareness of an ethical obligation to alleviate the patient's distress through a process of ethical appraisal and discernment. Similarly, recognizing the source of ethical unease or conflict can help to inform the appraisal and discernment process.
In Maria's case, clinicians may have experienced feelings such as empathy, tenderness, sadness, guilt, remorse, shame, frustration, or anger in response to perceived conflicts in values, interpersonal disagreements, and institutional constraints. These have been identified as key elements in the experience of moral distress and can either provide support or intensify the distress.10,33,34 Although the proposed dynamic framework 11 focuses on the responses of individual clinicians to moral distress, it is also integral to creating a healthy work environment supporting clinicians to practice with integrity. 35
The ethical dilemmas in Maria's case escalated, as the perception of conflicting values and commitments and team disintegration grew. Some clinicians may have concluded it was unconscionable to participate in actions that caused disproportionate suffering and pursue goals perceived as unattainable. 36 Clinicians struggling to address the dissonance between what they are doing and their professional roles 14 often express this conflict as a lament of “Why are we doing this?” Coupled with an experience of injustice on behalf of the patient and/or broader society, this conflict can lead to unhealthy emotional arousal and moral distress. 14 Acting against informed moral judgment creates a conflict of conscience by abandoning, consciously or unconsciously, convictions, ethical values or norms, and/or personal integrity. 37 Conflicts of conscience are common among clinicians, particularly involving the care of patients at the end of life.38,39
Emotion regulation
Clinicians caring for Maria are likely to have experienced an initial empathic response, potentially experienced later as aversion. Being fixated on a particular appraisal of the situation, unable to reappraise it from a different perspective, can result in emotion disregulation. 40 The lack of awareness of the perspectives of others may lead to inaccurate conclusions. For example, some clinicians may have concluded that Tom was in denial about the possible outcome for his wife—and that his request to continue aggressive treatments and limit certain therapies to treat pain was unreflected or uninformed.41,42 Similarly, Tom may not have been aware of the level of the clinician's moral distress, and may have concluded that they were uncaring. Members of the interdisciplinary team could also react to the responses of their colleagues from an uninformed perspective.
The past experiences of family members and clinicians may create distress and negative responses to Maria's situation. 19 If not stabilized, these emotional responses may exacerbate feelings of distress and instigate a focus upon one's own pain instead of Maria's suffering. In these instances, a clinician may try to convince the patient and family that their appraisals are inaccurate, or that they should accept the clinician's recommendations to forgo life-sustaining therapies. 43 Family members may adopt a defensive stance to protect the patient from a perceived threat of abandonment by the health care team. The result is often an intractable power struggle, where neither party is able to maintain a therapeutic relationship, and where isolation, conflict, and distrust grow.
Strategies for Addressing Moral Distress
After months of pursuing various options, the team caring for Maria requested ethics consultation in response to their moral distress, which was negatively impacting their ability to function well, individually and as a group. The consultation involved a series of meetings with the team and Maria's husband, where aspects of the framework were applied. Empathy and perspective taking were highlighted when Tom spoke about his fears and concerns about Maria's recovery and his acknowledgement of her impending death. This gave the clinicians an opportunity to attune to his situation and for some to shift to a more empathic response. Similarly, when nurses described their distress in how their actions were adding to Maria's suffering, both the physicians and Tom were able to acknowledge the intensity of the exposure to witnessing Maria's suffering and the distress that accompanied it. A particularly poignant moment in the consultation occurred when the surgeon spoke about his distress and sense of accountability for doing the transplant in the first place and the overwhelming sense of responsibility for her current status. Additionally, moral sensitivity was cultivated by the questions posed by the ethics consultation team, illuminating the morally salient aspects of her case and leading to greater awareness of the ethically permissible boundaries of treatment. At the end of the meeting several of the clinicians expressed a renewed commitment to provide care for Maria because of greater understanding of Tom's perspective and the acknowledgement of each other's predicament.
Subsequent meetings with consultants familiar with the proposed framework included an overview of the elements of the framework and highlighted the contribution of memory, empathic overarousal, and the physiologic consequences of unregulated moral distress. Various strategies outlined in Table 2 were offered as alternatives. Although there has not yet been systematic adoption of all the strategies, the case has fueled ongoing exploration of individual and system contributions to the issues that arose, continued dialogue, and commitment to design support systems and educational programs to enlarge the professional repertoire.
The authors propose that moral distress might be transformed through the adoption of various interventions that assist clinicians in the regulation of emotion and attention and assist with cultivating insight and a metacognitive perspective. Table 2 includes strategies that might prevent or transform aversive responses to moral dilemmas and provide the stability to foster principled compassion instead of ungrounded moral outrage. These include cognitive, attentional, affective, and somatic approaches that are derived from contemplative traditions used for capacity building, resilience training, and reduction of distress. 44 According to Halifax, 45 five interrelated domains need strengthening when developing principled compassion. These include attentional balance; affective balance; cognitive dimensions, including intention and insight; and embodiment. 45 Mental training techniques aid in the development of these domains and aid individuals with mental pliancy, equanimity, and principled, ethically based compassion.
Approaches to transform moral distress include mindfulness practices aimed at stabilizing attention and emotions; insight practices to distinguish self from other (patient/family); the development of the capacity to inquire and explore; 46 awareness practices that assist clinicians in recognizing emotional triggers and states of negative arousal, including symptoms of empathic overarousal; and an ethic of care derived from insight into the nature of suffering (see Table 2).
Peer support and use of experiential learning to enhance socialization, while exploring actual cases to foster ethical responsibility, are also recommended. Reported in more detail elsewhere,17,45,47 these modalities are most effective when coupled with systems-focused approaches 48 beyond the scope of this paper, such as patient care conferences on goals of care, 49 proactive identification of ethically problematic cases, 50 and debriefings after patients die. 51
Footnotes
Conclusion
Applying the Framework for Understanding Moral Distress to the case involving Maria provides opportunities for understanding response mechanisms amenable to intervention. Using the proposed framework as a guide, it is possible to notice where the process can go awry, causing emotional destabilization, personal distress, avoidance behaviors, and unregulated moral outrage. Alternative strategies and practices are illustrated above and in ![]() . Using the framework to understand the process may help mitigate or avoid the progression of distress and a concurrent negative appraisal that leads to moral distress or moral outrage. Intervention evaluation research is needed to determine the efficacy of the framework.
. Using the framework to understand the process may help mitigate or avoid the progression of distress and a concurrent negative appraisal that leads to moral distress or moral outrage. Intervention evaluation research is needed to determine the efficacy of the framework.
Acknowledgments
The authors acknowledge their colleagues of the Upaya Institute's Professional Training Program in Compassionate End-of-Life Care (Being with Dying) for their invaluable contribution to the development of this model and the various researchers, cited in this article, whose work has inspired us. Gratitude to Cheryl Zogg and Kelly Wilson-Fowler for assistance with manuscript preparation.
Author Disclosure Statement
No competing financial interests exist.