
Abstract
Abstract
Background and Objectives:
Very little information exists on the number of resources utilized by individuals living with and dying of pediatric life-threatening diseases (LTDs). This study quantifies end of life (EOL) resource utilization among the pediatric population in British Columbia, Canada.
Methods:
Data from Vital Statistics British Columbia were obtained for the pediatric population that died between 2002/03 and 2006/07. Our sample included three age groups: less than 1 year (excluding sudden infant death syndrome cases), 1 to 19 years, and 20 to 24 years. Using data from the Medical Services Plan and Discharge Abstract Database, we calculated annual rates of resources utilized (number of discharges, number of days in hospital, and number of medical services used) for every pediatric death that was due to an LTD in our selected 5-year time frame. Place of death was also explored.
Results:
During the fiscal year of death and the fiscal year prior to death, children/adolescents and young adults dying of a pediatric LTD respectively experienced 5.3 and 3.7 hospital discharges, spent 48 and 39 days in the hospital, and required approximately 222 and 230 medical services. Infants were discharged once on average, and required 21 medical services.
Conclusions:
Resource utilization was very high for all three age groups, demonstrating the intense need for care by children dying of disease. These findings call for the strengthening of palliative care services in the province.
Introduction
Canuck Place Children's Hospice (CPCH) was founded in 1995 in Vancouver, BC as the first free-standing pediatric hospice in North America. The CPCH program annually provides palliative care to approximately 250 individuals aged 0 to 19 years who are living in the province with various life-threatening diseases. The required multidisciplinary provision of care is provided by the hospice program throughout the child's entire lifetime and even after death through bereavement services. Still, the number of children/families who are eligible for palliative care is far less than the number who actually receive it.2,3 Many children are experiencing high frequencies of hospital admissions and long lengths of stays in facilities that may not be equipped to address the needs of these children beyond clinical management.4,5
The demand for palliative care can strain tertiary care resources, while simultaneously burdening the children and families who are experiencing unmet needs. Most studies examining pediatric palliative care focus on the development and implementation of services. Little information is available on the resource requirements of this population, or where children with terminal disease are dying. To navigate programming to address the care needs of children living with and dying of LTDs, we must first understand what level of resources they are utilizing. 6 Examining health care utilization among children receiving EOL care can allow us to grasp the intensity of care needed during the most encumbering stage of terminal diseases. 7 The objective of this article is to quantify various parameters of resource utilization near EOL by individuals who died of a pediatric LTD.
Methods
Our sample includes infants, children/adolescents, and young adults who died of a natural cause between the fiscal years of 2002/03 and2006/07 in BC, Canada. Anonymous, age-specific record level data were provided by Vital Statistics Agency–Government of British Columbia. All International Classification of Diseases, 10th Revision (ICD-10) chapters for deaths due to natural causes were obtained from Vital Statistics at the patient record level to determine the underlying and principle causes of death. These included neuromuscular, cardiovascular, respiratory, renal, gastrointestinal, hematology, immunodeficiency, metabolic diseases, and other congenital or genetic defects/malignancies. We excluded any deaths that were due to external causes (e.g., suicide, trauma, accidents).
Based on the varying disease trajectories for different pediatric LTDs, we categorized our study sample into three distinct age groups:
1. Infants: includes all infants who died of natural causes at less than 1 year of age. This group excludes any deaths due to sudden infant death syndrome. 2. Children/Adolescents: includes all children and adolescents between 1 and 19 years of age who died of natural causes. 3. Young adult: includes youth who died of natural causes between the ages of 20 and 24. We selected this cutoff to partially control for adult-acquired disease, but to also account for young people who died of pediatric diseases in the first few years after transitioning from pediatric to adult care.
We utilized patient records with a valid Public Health Number with which each case (death) could be linked to either the Medical Service Plan (MSP) and/or hospital Discharge Abstract Database (DAD). To calculate resource utilization rates for each individual who died of a pediatric LTD in BC, we divided the following indicators of resource utilization by the annual number of deaths in each age group:
1. Length of days spent in the hospital 2. Number of hospital discharges 3. Number of Medical Services (MSP) used (Medical Plan counts each billing by a physician as a “Medical Service”; this includes direct encounters, procedures, laboratory and imaging studies)
These data were linked to each case during the fiscal year of death and fiscal year prior to death. Our data demonstrate that resource utilization peaks in the fiscal year prior to death. By observing both the fiscal year prior to and the fiscal year of death, we captured the number of resources utilized by each case patient during their last full year of living, and during the last few months of life. To illustrate, to derive a rate for number of days spent in the hospital during the last 1 to 2 years of life for each 1- to 19-year-old who died in 2002/2003, we divided the total number of days they spent in hospital during 2001/2002 and 2002/2003 by the total number of deaths among them:
We then averaged per case resource utilization across 5 years to account for any year-specific occurrences that would have resulted in lower/higher than average rates (Table 1).
BC, British Columbia; SD, standard deviation.
Data on location of death were also obtained for each case and categorized as home, hospital, or other facilities (e.g., hospice). Two-tailed Z test for proportions were used to evaluate variations in place of death among our three age groups at p=0.05 level of significance.
Results
A total of 1353 deaths due to natural causes were recorded between 2002/03 and 2006/07 for all cases in our sample (records linkable to DAD and/or MSP). Of these, 58% were infants, 26% were children/adolescents, and 16% were young adults. Of the 213 deaths due to natural causes among young adults, 35 were due to adult-acquired cancers (diagnosed after the age of 20), for which we were unable to control.
On average, children/adolescents and young adults nearing EOL were expected to be discharged 5.3 and 3.7 times, respectively. The number of hospitalizations among children/adolescents appears to have declined from 6.4 and steadied at 4.9 over our 5-year study period. Infants who died of an LTD were expected to have 1 discharge during the same time period, and the number of discharges progressively increased over time for this age group (Table 1). Children/adolescents and young adults spent, respectively, 13% and 11% of their last 1 to 2 fiscal years in the hospital. The number of days spent in the hospital decreased near the end of our study's time frame among 1- to 19-year-olds (Table 2). The number of MSP services utilized by children/adolescents and young adults was also substantially high. Children/adolescents could expect to utilize more than 230 medical services during the last 1 to 2 years of life. Young adults required 222 MSP services on average; the rate of utilization for this group substantially increased over time (Table 3).
BC, British Columbia; SD, standard deviation.
BC, British Columbia; SD, standard deviation.
Figure 1 demonstrates that most infants died in the hospital, whereas children/adolescents and young adults died not only in the hospital, but also in the home setting and in other care facilities. Approximately 12% of infants died at home, which was significantly different when compared with the 24% of children/adolescents (p=0.02), and 30% of young adults who died at home (p<0.01). Only 1% of infants died in “other facilities,” which was also significantly different than the 10% of children/adolescents who died in “other facilities.” The majority of infants (87%) died in the hospital, a finding that was significantly different when compared with the 67% of children/adolescents, and 66% of young adults who died in the hospital (p<0.01). Place of death was not significantly different between children/adolescents and young adults (Table 4).
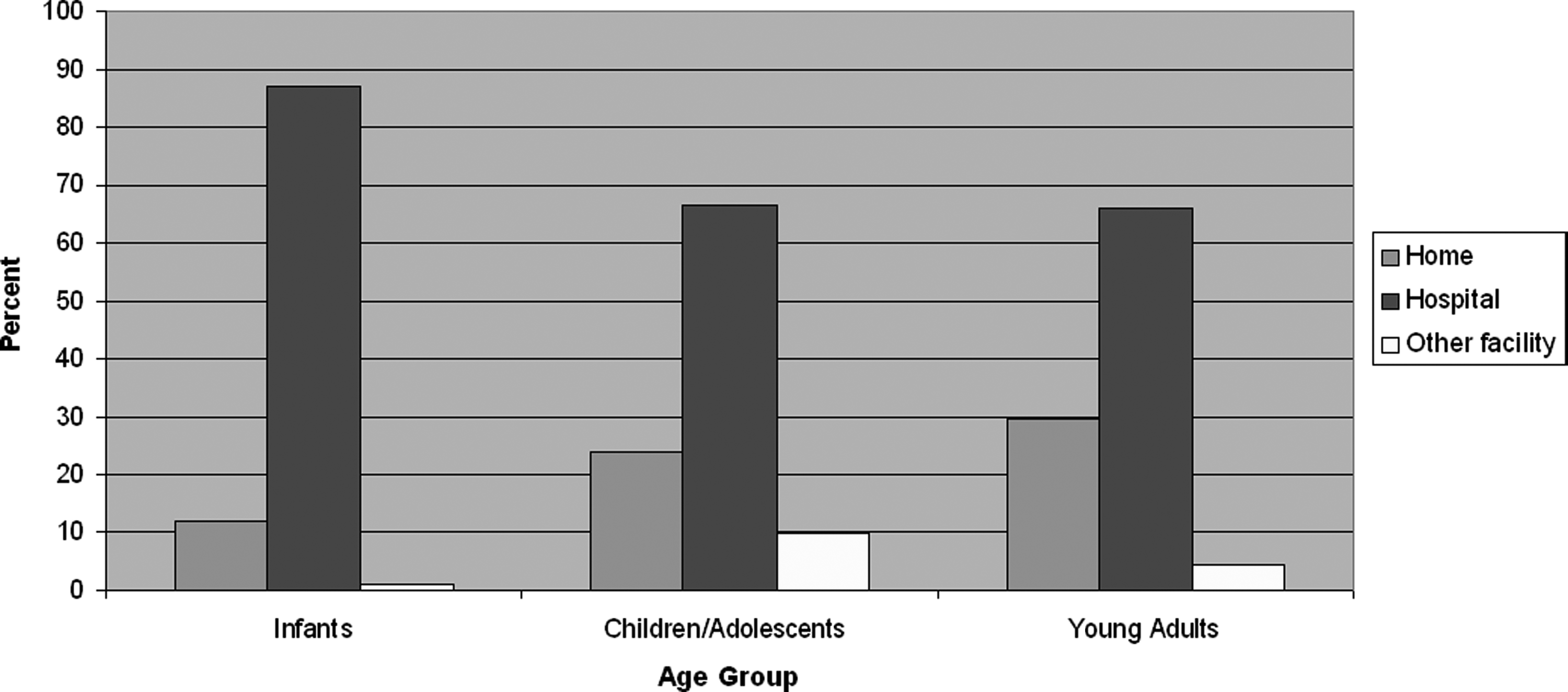
Place of death among individuals age 0 to 24 years who died of a life-threatening disease in BC during 2002/03–2006/07.
BC, British Columbia.
Discussion
In this study we attempted to estimate resource utilization by individuals aged 0 to 24 years who died of an LTD during the last 1 to 2 years preceding death. We confirmed that those living with a pediatric LTD are experiencing multiple hospitalizations with long lengths of overall stay. Other researchers have also demonstrated the high number of medical services required by individuals living with pediatric LTDs, 2 but have reported median lengths of hospital stays only, which does not reflect the number of times they are in and out of hospitals, or the total number of days spent in care facilities in a given year.
Different planning assumptions and service delivery issues need to be considered for different age and diagnostic groups. The bulk of pediatrics deaths occur among infants.1,8 Due to the short life span of infants who die of an LTD, most of the resources utilized occur in the same fiscal year of death and our rates should be interpreted as such. Infants who die of an LTD spend the majority of their lives in the hospital, and usually die there, 9 which is reflected in the 1 discharge per death rate derived from our hospital discharge data. The number of discharges and medical services used is steadily increasing among cases of infant deaths. We speculate that over time, sick infants are returning to the hospital at least once more after their first initial discharge to receive care and treatment before dying. Researchers have noted that the complex health conditions of infants with LTDs render a home death difficult to envision. However, they recommend examining the barriers to a nonhospital place of death as suited to family wishes. 4
The variations in place of death for children/adolescents and young adults may be a reflection of increased hospice utilization for individuals with pediatric LTDs in BC. The downward trend in admissions and number of days spent in the hospital among children/adolescents over time may also represent increased involvement of nonhospital-based palliative care providers in the home and at a free-standing children's hospice. Previous literature has demonstrated that many pediatric LTD deaths occur in the hospital 2 ; however, a considerable number die at home. 9 Other researchers suggest that when different areas of support are available, the location of death can also be shared in home and hospice settings,10,11 and they recommend advancements in home-based palliative care to address the increasing number of home deaths. 9 Further, advancements in medicine are extending the life expectancy for many pediatric LTDs. 12 Consequently, increases in medical services and care needs such as the trends observed among young adults can be expected over time and transition programming to adult palliative care must be carefully anticipated and planned for. 13
Children/adolescents and young adults with pediatric LTDs are experiencing multiple hospitalizations during the most trying time of their short lives. Researchers have used “visits to emergency departments” for patients who are at EOL as an indicator of poor quality care.14,15 Barbera et al. 16 argue that the high number of hospital emergency department (ED) visits for EOL patients is highly stressful for both the patients and families. The researchers also identified the main diagnoses from these admissions as ones that could have been properly managed by a comprehensive palliative team. Clinical descriptions of families who had visited the ED with their dying child frequently cited their inability to “cope” at home. 16 Admission to a hospice program early after diagnosis can provide continued support from an interdisciplinary team that has the opportunity to establish rapport, and facilitate an emotionally safe and highly individualized continuum of care. Over time, families can better anticipate and cope with expected outcomes, make informed decisions around the nature of EOL care sought, and enhance their in-home care capacities, rendering many EOL ED visitations unnecessary.16,17
Palliative care services can also reduce the need for redundant and taxing medical tests, while providing the psychosocial support that hospital teams may not be able to offer during EOL care.2,5,17 For BC Children's Hospital, an intensive care unit (ICU) or neonatal ICU (NICU bed) costs $4910 per patient day, whereas an equivalent bed for EOL care (range of medical services comparable to a NICU/ICU bed at a hospital) per patient day at CPCH is $3325. In addition to reducing costs, 18 patients who are nearing EOL may prefer care in a nonhospital environment if their pain can be appropriately managed. 19 Hospice deaths have been noted as less chaotic, with home-like comfort, and enhanced dignity.17,19 Further, hospital staff, many of whom do not have palliative training, may find the provision of multidimensional care required by such cases overwhelming.5,20 As such, patients, families, the acute health care system, and health care staff will suffer if appropriate support is not readily available.
We must acknowledge certain limitations within our methods. We may have not been able to capture families that experience unequal access to resources. Disparities in health care utilization may isolate the most marginalized individuals.21,22 BC's northern communities do not have accessible transportation that can easily accommodate the travel needs of a child with an LTD. As such, we cannot ascertain whether death at home is the family's preference, or only choice. Our resource utilization rates are underestimated as families and children that did not access resources were included in our denominators. Barriers to initiating palliative care for geographically isolated families must be identified, as they may be in most need of support. We were also limited by the nature of how our data were allocated. For each case, death would have occurred at any given point during the year, terminating resource utilization. As such, we are underestimating the number of resources that would have been used if each case patient had been alive during the entire fiscal year. We expanded our time frame to include the fiscal year prior to death to account for this limitation. Further, we were reliant on death certificate records that may have inaccurately captured cause of death. Our young adult group includes 35 deaths (of 213) that were due to adult-acquired diseases that we were unable to control for; the findings of this age group must be interpreted with this reality in mind. Further, 5% of all deaths were categorized under ICD-10, Chapter 18 where cause of death was due to “symptoms, signs and abnormal clinical and laboratory findings not elsewhere classified.” We included these cases to capture any deaths that could have been due to an undiagnosed disease, but we may have also captured deaths that were due to external causes.
Living with a pediatric LTD is extremely taxing on both the individual and the caregivers. Our findings demonstrate the critical need for the development and strengthening of advanced palliative care. In the least, patients and families should be provided with options that extend beyond hospitalization when deciding where they can be best supported. Research has demonstrated positive patient/family outcomes when decision making around pediatric EOL care takes family preferences and wishes into account. 23 The high utilization of resources by pediatric palliative cases presented in this study underlines the urgent need for effective planning that can equip centers with the ability to respond to the immense needs of dying children. Palliative care provision within hospitals can allow the families of terminally ill patients to make important decisions around the need for unnecessary aggressive interventions by facilitating dialogue for comfort care and EOL planning. 8 Enhanced development of in-home and hospice care programming can abate the large demand for medical services during EOL and can also foster a provision of treatment that extends beyond clinical management to include emotional, spiritual, mental, and psychological support for both the child and the family.
Footnotes
Author Disclosure Statement
No competing financial interests exist.