
Abstract
Abstract
Context:
Dementia care giving can lead to increased stress, physical and psychosocial morbidity, and mortality. Anecdotal evidence suggests that hospice care provided to people with dementia and their caregivers may buffer caregivers from some of the adverse outcomes associated with family caregiving in Alzheimer's Disease (AD).
Objectives:
This pilot study examined psychological and physical outcomes among 32 spousal caregivers of patients with AD. It was hypothesized that caregivers who utilized hospice services would demonstrate better outcomes after the death of their spouse than caregivers who did not utilize hospice.
Methods:
The charts of all spousal caregivers enrolled in a larger longitudinal study from 2001 to 2006 (N=120) were reviewed, and participants whose spouse had died were identified. Of these, those who received hospice care (n=10) were compared to those who did not (n=22) for various physiological and psychological measures of stress, both before and after the death of the care recipient. An Analysis of Covariance (ANCOVA), with postdeath scores as the dependent variable and pre-death scores as covariates, was used for all variables.
Results:
Significant group differences were found in postdeath depressive symptoms (HAM-D; F(1,29)=6.10, p<0.05) and anxiety symptoms (HAM-A; F(1,29)=5.71, p<0.05). Most psychological outcome variables demonstrated moderate effect sizes with a Cohen's d of>0.5 between groups.
Conclusions:
These data suggest that hospice enrollment may ameliorate the detrimental psychological effects in caregivers who have lost a spouse with Alzheimer's Disease. Based on these pilot data, further prospective investigation is warranted.
Introduction
Hospice care seeks to improve quality of life and reduce suffering at the end of life for seriously ill patients and their caregivers.20,21 Psychological and physical distress related to caring for someone with an advanced, life-threatening illness, such as Alzheimer's dementia, is an important target of hospice care. Currently, 5.4 million U.S. adults suffer from AD, which, in its final stages, is now considered a terminal illness.22,23 Care for people with AD is provided by 14.9 million caregivers, accounting for $183 billion in annual costs. 23 Caregiver stress is common and costly, as well as a major source of suffering for patients and families. In this context, effective strategies to reduce the distress associated with family caregiving in AD have the potential to significantly impact quality of life and health outcomes in this large population, while reducing health care costs.
This preliminary pilot investigation examined whether hospice care may ameliorate some of the psychological and physiologic stresses associated with caregiving for a spouse suffering from AD.
Methods
Participants
Subjects were drawn from a larger, longitudinal investigation that prospectively assessed psychological and physical health outcomes for a cohort of 120 elderly spousal caregivers of people with AD, during the five-year study period from 2002 to 2006. Detailed methods for the larger study are provided elsewhere. 19 Subjects had participated in this larger study at the University of California, San Diego (UCSD) Alzheimer's Disease Research Center. All participants provided in-home care for their spouse with AD, were at least 55 years of age, and were free of serious medical conditions at the time of enrollment. Participants were excluded if they were caring for a friend, a sibling, a child, or otherwise were not caring for a spouse. Additional exclusion criteria included the use of beta-blocker or anticoagulant medication, or uncontrolled hypertension, as these were potential confounders for biological outcomes assessed in the parent project. The UCSD institutional review board approved the protocol, and all participants provided written informed consent prior to enrollment.
The charts of all caregivers enrolled in the parent study (n=120) were reviewed, and participants whose spouse with AD died during the five-year study period were identified (n=32); these 32 caregivers served as the subjects in the present report. This report compares changes in pre-death to postdeath psychological and physiological outcomes for participants in the parent study who reported hospice enrollment for their spouse (n=10) as compared to those who did not use hospice services (n=22).
Procedures
In the parent longitudinal study, research staff conducted face-to-face assessments of caregivers at 12-month intervals. In addition, regular check-in phone calls were made every six months to inquire about changes in health status and transitions in caregiving (i.e., placement of the AD spouse in long-term care or death of the AD patient). After any reported transition in caregiving, an additional follow-up assessment was scheduled within six months.
Measures
A detailed description of the measures used for demographic and outcomes variables is provided elsewhere. 19 Briefly, demographics included age, gender, ethnicity, years of education, and income. Dementia severity (of the person with AD) was assessed using the Clinical Dementia Rating Scale. 24 The primary psychological outcomes included symptoms of depression and anxiety, as measured by the 17-item Hamilton Rating Scale for Depression (HAM-D)25,26 and the 14-item Hamilton Rating Scale for Anxiety (HAM-A). 27 Modes of caregiver coping were measured using the Avoidance Coping subscale of the Ways of Coping instrument, 28 since this coping strategy has been most consistently linked to psychological morbidity and decreased well-being. 29 Assessments of physical health included the following: (1) an overall health outcomes score derived from a semistructured interview assessing participants' health outcomes over the prior six months; (2) resting blood pressure and heart rate; and (3) hemodynamic reactivity to stress, as measured by response of blood pressure and heart rate to a simulated stressor.30,31 Finally, caregiver sleep was evaluated using the Global Sleep Quality Score of the Pittsburgh Sleep Quality Index (PSQI). 32 All instruments were administered by research staff and based on participants' self-report of symptoms.
Data analyses
Change in the dependent variables from pre-death to postdeath was analyzed using Analyses of Covariance (ANCOVAs), with postdeath scores as the dependent variable and pre-death scores as covariates, controlling for the effect of pre-death differences on outcome measures. This analysis used pre-death and postdeath measures most proximate to the spouse's death (i.e., the set of measures immediately before and immediately after the spouse's death). For heart rate and blood pressure reactivity, residualized change scores (i.e., the posttest score as a deviation from the posttest-on-pretest regression line)32,33 were created and the postdeath score was used as the dependent variable, with pre-death scores as covariates. Hospice involvement was used as the primary predictor in all analyses. Due to the small sample size, effect sizes for group mean differences (Cohen's d) were calculated for all outcome variables in this study. For statistical tests, significance was assumed at the p<0.05 level.
Results
Pre-death demographic data, scores of dementia severity, and baseline blood pressure measurements for all participants are presented in Table 1. Caregivers who utilized hospice were more highly educated (16.1±1.85 years versus 14.18±1.76 years; t(30)=2.81; p<0.01) and showed a trend toward higher incomes. No other significant baseline differences were observed, including depressive symptoms (p=0.314), anxiety symptoms (p=0.356), avoidance coping (p=0.759), health symptoms (p=0.710), SBP (p=0.702), or DBP (p=0.966).
p<0.05
After controlling for differences in pre-death outcomes scores, significant group differences were found in postdeath symptoms of depression and anxiety as measured by the HAM-D and HAM-A, respectively (see Figure 1). Specifically, caregivers who utilized hospice reported lower postdeath symptoms of depression (2.2±0.55 versus 5.73±1.18; F(1,29)=6.10, p<0.05) and anxiety (3.70±1.16 versus 6.14±1.12; F(1,29)=5.71, p<0.05), compared to those who did not use hospice. No group differences were observed with use of avoidance coping, physical health measures (overall health outcomes, or blood pressure or heart rate reactivity), or sleep quality. Table 2 provides depictions of raw depressive symptoms, anxiety symptoms, and health outcomes scores (pre- and postdeath) by group, as well as Cohen's d values.
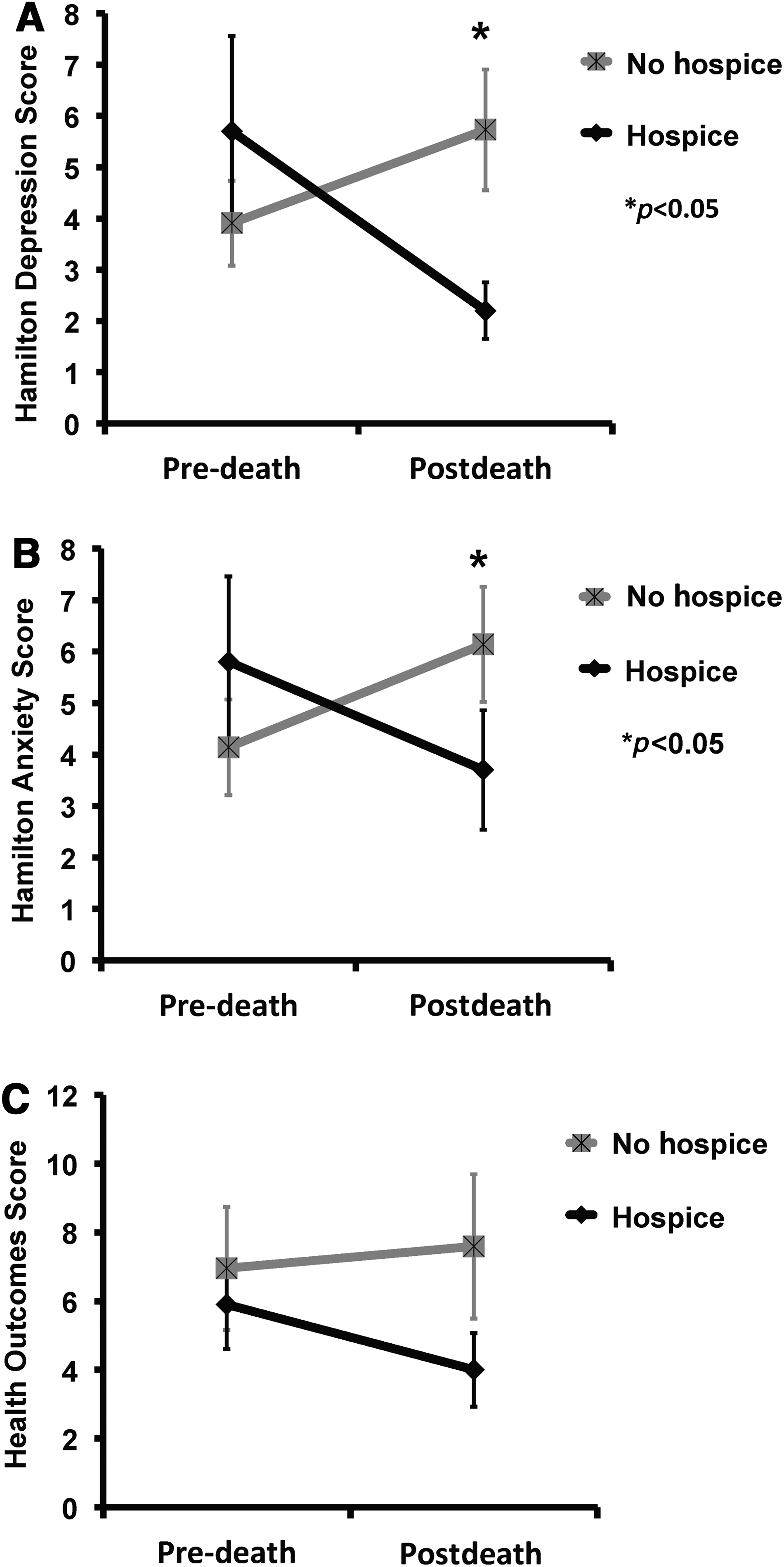
Change from pre- to postdeath by hospice and nonhospice groups±standard error for
p<0.05
PSQI, Pittsburgh Sleep Quality Index.
On average, the postdeath assessment occurred 7.3 months after the death of the spouse (SD=1.3 months). Including this variable as a covariate in the analysis did not significantly predict HAM-D scores (p=0.493). Also, hospice condition remained significant (p=0.022).
Discussion
This pilot investigation was aimed at providing preliminary evidence for the relationship between hospice care and the well-being of family caregivers for patients with AD. The data reported here suggest an association between hospice enrollment and decreased psychological distress in these caregivers, specifically with reductions in symptoms of depression and anxiety. The data failed to show a relationship to several physical health outcomes, coping strategies, or sleep quality.
Caution should be used in interpreting these findings, given the small sample size and nonexperimental design of the study. Only a small number of caregivers experienced the death of their spouse during the study period, and even fewer utilized hospice care. Recruitment from a single geographic region also limits generalizability. Similarly, participants were not randomized to exposure groups, and other methodological strategies to control for baseline differences between the groups were not prospectively incorporated into the study design. For these reasons, alternative explanations for the results cannot be ruled out, such as baseline (pre-death) group differences that might account for hospice utilization and influence change in psychological distress.
Despite these limitations, these data point to potentially fruitful areas of further investigation. Larger, experimental studies are needed to validate and further characterize the relationships suggested by the results of this pilot study. For example, the effects of specific hospice care elements on psychological distress should be explored in order to inform effective strategies for caregiver support in this population. Specifically, does the location of hospice care (in-home versus inpatient, for example) influence the amelioration of psychological stress? Do specific elements of bereavement care (individual counseling versus support groups, for example) affect psychological benefits associated with hospice use? Does the duration of engagement in hospice influence psychological benefits? A larger study with more robust methods would allow an exploration of these important questions. Similarly, this data suggests a trend toward significance in health outcomes scores (p=0.07). Whether or not hospice participation may also confer some physical health benefits to caregivers deserves further study and attention in more robust trials.
Although preliminary in nature, the data from this study suggest a relationship between hospice care and caregiver psychological well-being. The consequences of unrelieved psychological distress are substantial: depressive symptoms, for example, have been shown to contribute to the development of cardiovascular disease in caregivers 19 as well as to increased cardiovascular morbidity and mortality in the general population. 34 Moreover, increased symptoms of depression and/or anxiety, if not detected or addressed, can increase the perceived severity of pain and other physical symptoms;35–38 affect physical health and quality of life;35,39 impair decision making; impact the relationship with a care recipient, and significantly increase the probability of morbidity, mortality, 40 and suicide.41–45 Effective strategies to ameliorate psychological distress, particularly in the setting of caregiving for family members with AD, are likely to have a profound impact on the end-of-life experiences of these patients and their family members. Hospice care may serve as a model to deliver such interventions and thereby support caregivers in this final phase of caring for loved ones with AD.
Footnotes
Acknowledgments
The Palliative Care Psychiatry Program at San Diego Hospice and the Institute for Palliative Medicine was supported, in part, by the National Palliative Care Research Center, Award Number K23MH091176 (Dr. Scott Irwin) from the National Institute of Mental Health, and by donations from the generous benefactors of the education and research programs at San Diego Hospice and The Institute for Palliative Medicine. Other relevant support came from National Institute on Aging grants R01 AG015301 (Dr. Igor Grant), R01 AG031090 (Dr. Brent Mausbach), and R01 AG08415 (Dr. Sonia Ancoli-Israel). The authors gratefully acknowledge the contributions of JSN TANAS. RIP San Diego Hospice. ↑→
Author Disclosure Statement
No competing financial interests exist.