
Abstract
Dear Editor:
Brain metastases (BMs) represent a significant cause of morbidity and mortality in cancer patients, and with an increasing number of management options the diagnosis has a considerable impact on resource use. With a few exceptions 1 the information on the service use of such a common diagnosis has not been systematically studied.
The aim of this study was to assess the frequency of the first diagnosis of BMs and the primary management pathway at a single institution over a defined three month period to provide a baseline of current service provision for this group of patients.
Between July 1, 2010 and September 30, 2010, 53 consecutive patients (20 men and 33 women) aged 33 to 79 years (median 58 years) were diagnosed with BMs at the Royal Marsden Hospital. This represents 5% of the population treated in the cancer center on an annual basis. Patient characteristics are shown in Table 1. The most common primary tumors were nonsmall cell lung cancer (26%), breast cancer (21%), colorectal cancer (11%), renal cell carcinoma (9%), melanoma (8%), and gynecological cancers (8%). This largely reflects the distribution of cancer patients by primary site and the recognized incidence of BMs in each group.2–4
PS, World Health Organization (WHO) performance status.
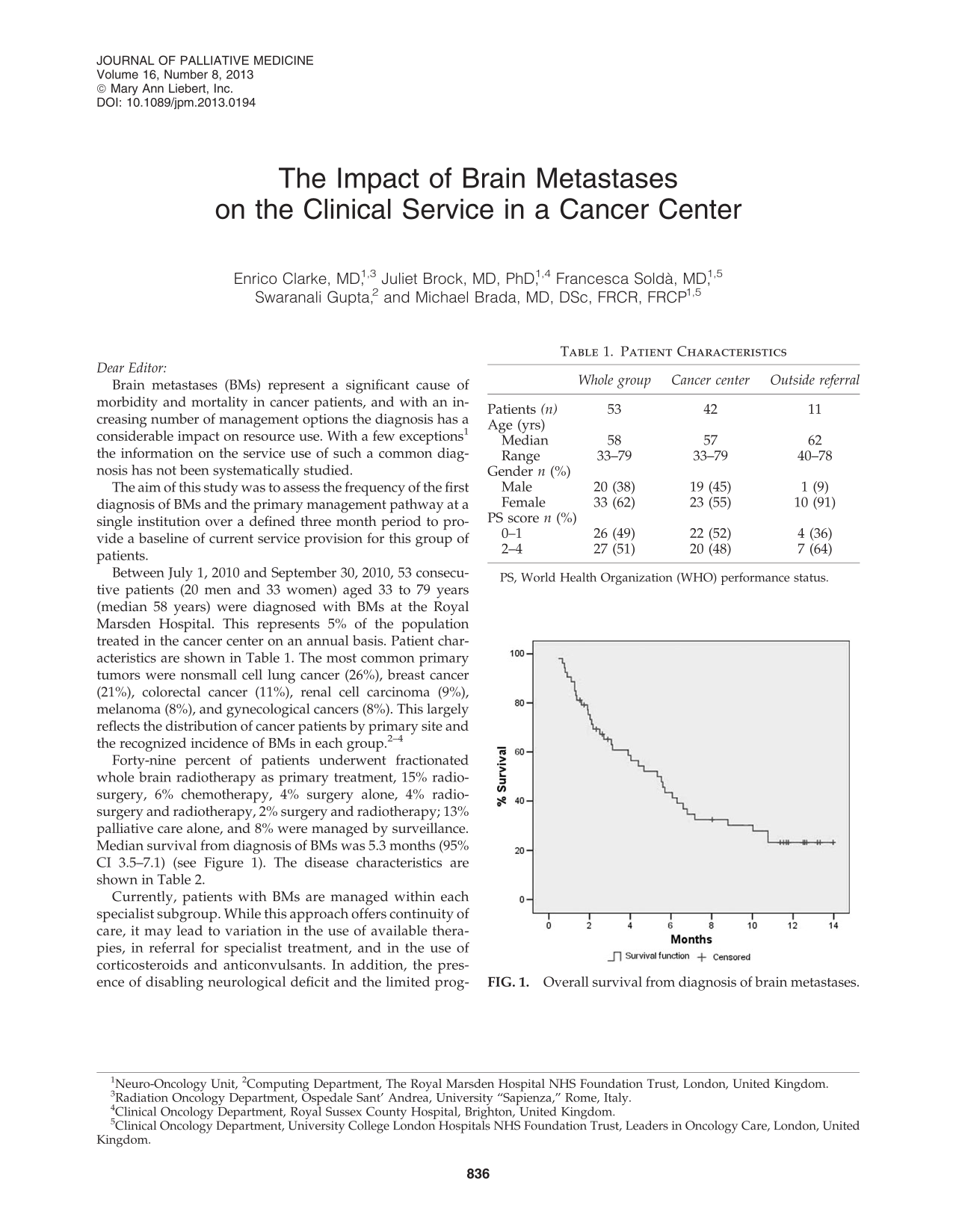
Forty-nine percent of patients underwent fractionated whole brain radiotherapy as primary treatment, 15% radiosurgery, 6% chemotherapy, 4% surgery alone, 4% radiosurgery and radiotherapy, 2% surgery and radiotherapy; 13% palliative care alone, and 8% were managed by surveillance. Median survival from diagnosis of BMs was 5.3 months (95% CI 3.5–7.1) (see Figure 1). The disease characteristics are shown in Table 2.
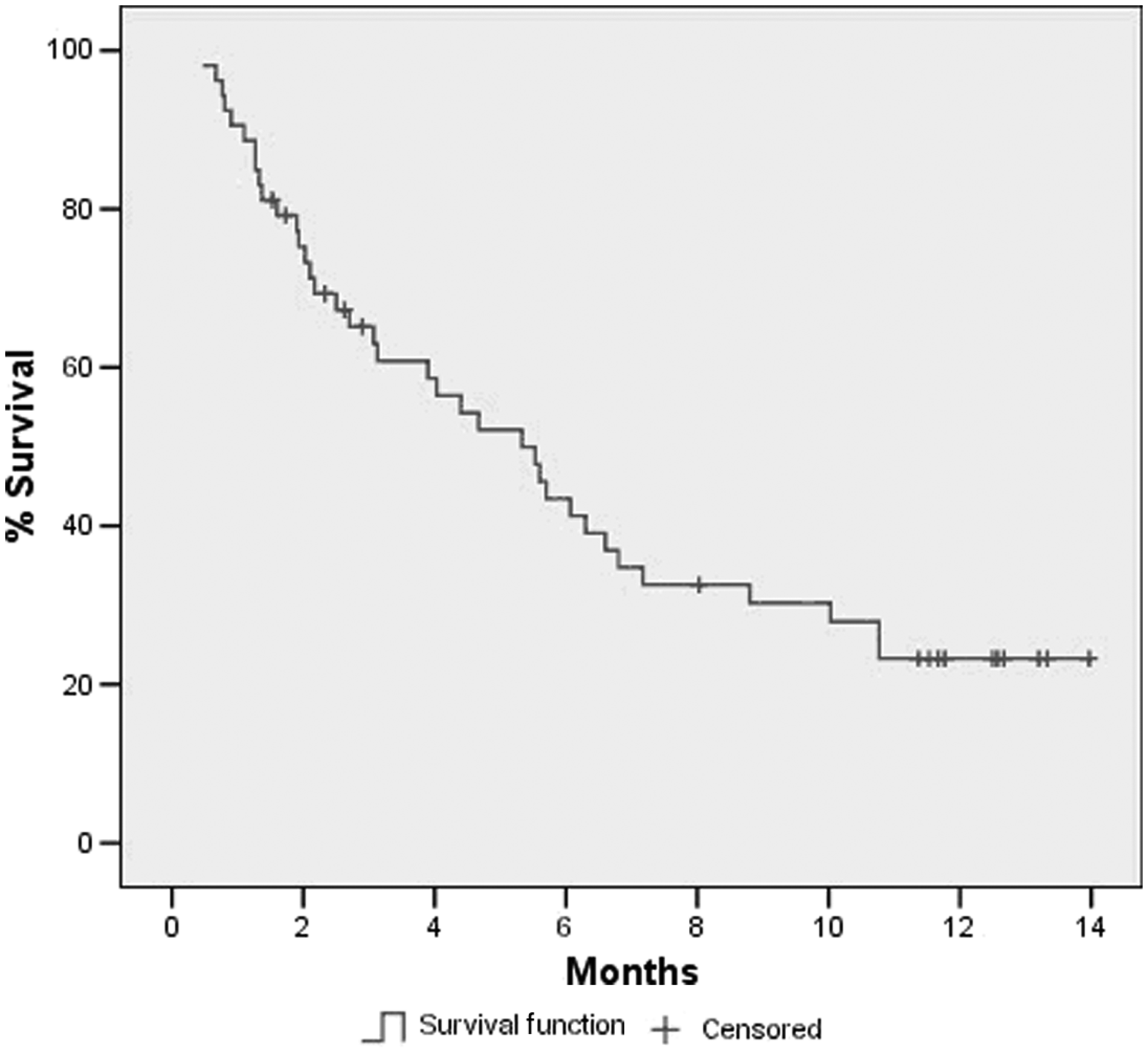
Overall survival from diagnosis of brain metastases.
BMs, brain metastases; CHT, chemotherapy; f RT, fractionated radiotherapy; NSCLC, nonsmall cell lung cancer; pall care, palliative care; SCLC, small cell lung cancer; SRS, stereotactic radiosurgery.
Currently, patients with BMs are managed within each specialist subgroup. While this approach offers continuity of care, it may lead to variation in the use of available therapies, in referral for specialist treatment, and in the use of corticosteroids and anticonvulsants. In addition, the presence of disabling neurological deficit and the limited prognosis in the majority of patients require access to support and palliative care services. BMs patients impose a significant workload with the need to access a range of management options.
The reported data provide a baseline of resource use within standard clinical practice and can be used for comparison with other models of care. A multidisciplinary centralized BMs service with direct access to all available treatments and links to palliative care is an alternative to the current model. It may optimize the referral pathway to other specialists and minimize the potential delay between diagnosis and start of therapy. While this approach, already implemented in some centers, has potential advantages, these should be validated. A centralized BMs service may have disadvantages for the individual patient, such as additional outpatient visits and lack of continuity of care, particularly in a difficult phase of the disease. In addition, with a relatively fast decision making process and easy access to specialist treatment using the conventional system of care, the potential advantages in terms of more appropriate referral and shortening of the management pathway should be demonstrated in prospective studies.