
Abstract
Abstract
Background:
Patients with dementia, an underrecognized terminal illness, frequently visit the emergency department (ED). These patients may benefit from ED-initiated palliative care (PC) consultation.
Objective:
The study's objective was to track the rate of ED-initiated PC consultation for patients with advanced dementia (AD) after an educational intervention, and to categorize decision making for physicians who chose not to initiate consultation.
Methods:
As part of a quality improvement project at a suburban, tertiary care, university-affiliated medical center, emergency physicians (EPs) were taught to identify AD patients and initiate PC consultation. A convenience sample of patients over age 70 was screened for AD by research staff from July 1, 2012 to August 1, 2012 using the Functional Assessment Staging (FAST) criteria. A questionnaire was then administered to patients' physicians to inquire about barriers to initiating consultation. Questionnaires and medical records of those who met AD criteria were reviewed to examine patient characteristics, disposition information, and consultation initiation barriers.
Results:
Patients (N=548) over 70 who visited the ED were approached and 304 completed the screening. Fifty-one of the 304 met criteria for AD. Their average age was 86; 33% were male. Eighteen of the 51 (35%) patients received a PC consultation sometime during their ED or hospital stay. Four of the 18 (22%) consultations were ED initiated. In 23 of 51 (45%) unique cases, physicians responded to the questionnaire. The majority felt that a PC consult was not appropriate for patients based on their knowledge, attitudes, or beliefs.
Conclusion:
Preexisting physician attitudes, knowledge, and beliefs prevent emergency physicians from addressing PC needs for AD patients.
Introduction
D
To improve access to PC services, studies have begun exploring different models of integration and ED-based barriers.7–8,10–15 We developed an intervention to educate clinicians on how to identify advanced dementia (AD) patients in the ED and how to initiate PC consults. For our study we aimed to observe the prevalence of ED-initiated PC consultation for AD patients after a quality improvement intervention and to assess emergency physicians' (EPs) barriers to initiating PC consults. AD patients were chosen as our population because they are highly likely to benefit from early PC intervention, and the existing screening methodologies were used to find these patients.18–21
Methods
EPs at one tertiary care, academic medical center with 120,000 annual ED visits were educated on the identification of AD patients and how to initiate a PC consultation. For attending physicians, education took place at two separate, one-hour-long, monthly faculty meetings and included a presentation on the significance of early PC involvement in seriously ill patients, the identification of patients with AD using the Functional Assessment Staging (FAST) criteria, and the PC consult initiation procedure. A screening tool listing the FAST criteria was attached to physicians' ID badges. Research assistants (RAs) were given the same presentation, with additional instruction on approaching patients, caregivers, and providers.
RAs screened patients 70 years or older on the ED tracking board for one month from 9 a.m. to 5 p.m. RAs approached patients and inquired about their clinical status using the screening tool. If the patient was physically or mentally incapable of participating, their accompanying caregiver was interviewed. The RAs confirmed FAST criteria with clinical staff if a caregiver was unavailable. If a patient met the criteria for AD (FAST stage of 7), the RAs interviewed the attending physician using the questionnaire in Figure 1.

Questionnaire administered to attending physicians.
The screening tool was adopted from primary literature and piloted with input from ED and PC staff and members of the research team.16–18 The physician questionnaire was designed by the same staff. FAST is a National Hospice and Palliative Care Organization endorsed, validated tool that categorizes the severity of functional decline in dementia patients. 19 The seventh stage of FAST represents a diagnosis of functionally severe dementia; characteristics include limited speaking ability, limited intelligible vocabulary, ambulation loss, inability to sit up or hold head up, or inability to smile. 16 If patients met any of these criteria as their baseline characteristics, they were classified as AD patients. Attached to the screening tool was the physician questionnaire (see Fig. 1).
For patients determined to have AD, medical charts were reviewed to determine disposition and PC consult information. EPs' responses to the questionnaire were qualitatively reviewed. For physicians who chose to elaborate on their questionnaire answers, their responses were categorized by the principal investigator (PI) and two RAs according to distinct conceptual themes developed using grounded theory methodology. 9 The institutional review board of the North Shore–Long Island Jewish Health Care System approved all research processes.
Results
Patients 70 years or above (N=548) were approached for screening, and 304 patients completed the screening (304/548, 56%). Patients were excluded for the following reasons: clinical instability, could not participate and no surrogate present, non-English speaking, and communicable disease. Of the 304 patients who were screened for AD, 51 met criteria with a FAST stage of 7 (51/304, 17%). In 23 of the 51 unique visits, attending physicians caring for these patients were available and chose to respond to the questionnaire (23/51, 45%). Table 1 describes the characteristics of the study participants.
Percentages in each column are calculated with N (first row) as the denominator.
As seen in Figure 2, of the 51 patients who met the FAST criteria for AD, 18 of 37 (49%) admitted patients received a consultation sometime during their hospitalization. Of the 18 patients receiving a PC consultation, four were initiated in the ED. None of the discharged patients received PC consults, since our hospital does not offer an outpatient PC service.
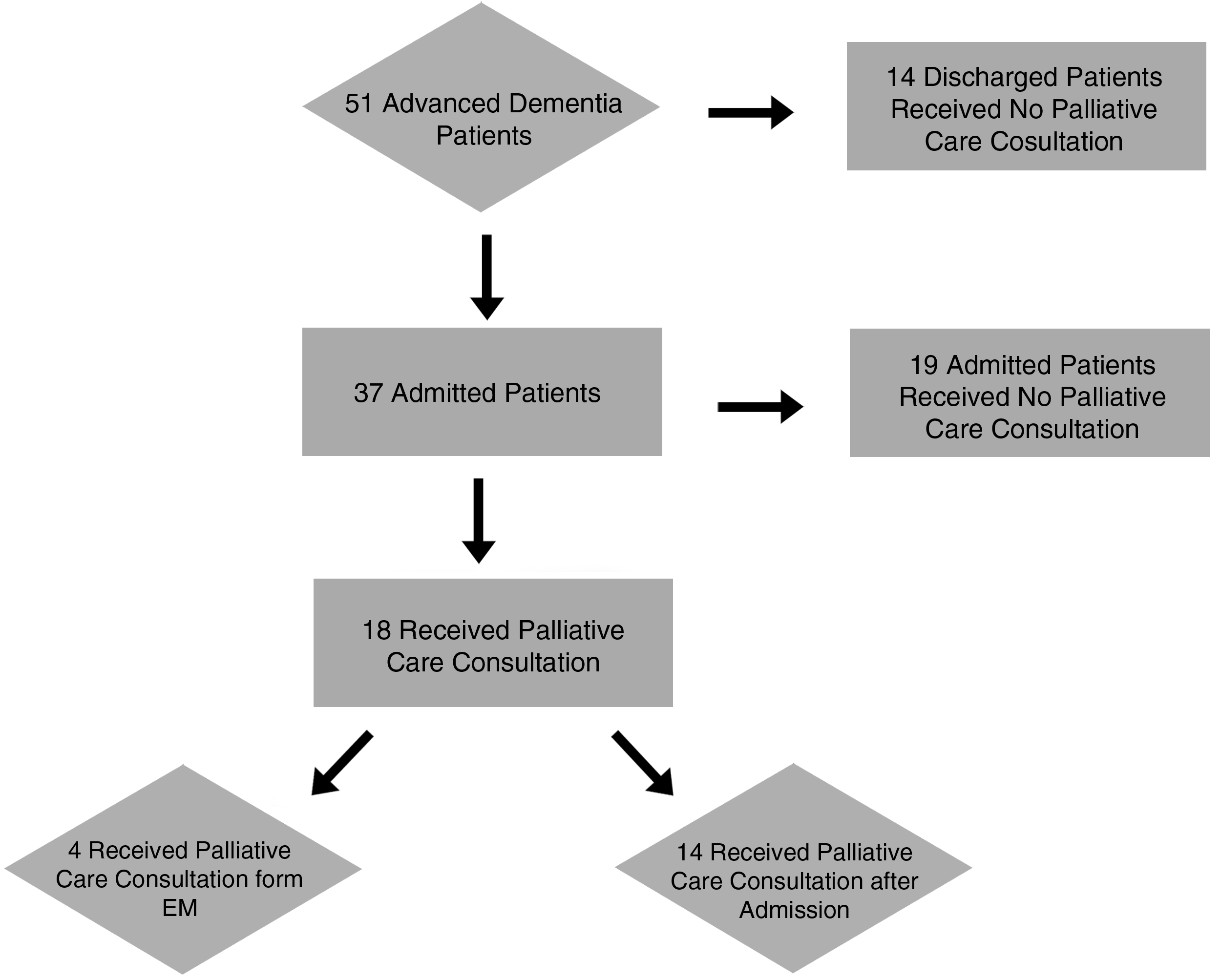
Flowchart depicting patient disposition and how many received a PC consultation.
In 23 of the 51 (45%) patients, attending physicians caring for the patients responded to the questionnaire. When asked why they chose not to initiate a consult for a patient meeting the FAST criteria, in 19 cases physicians stated a PC consult was not appropriate for the patient. In three encounters physicians responded that they were “too busy” and did not have the time to initiate this conversation. Finally, one physician was not comfortable initiating a consult because he did not want to “go against the family's wishes.”
In 13 of the 19 cases physicians chose to elaborate on their inactions. These responses all fell into the conceptual theme previously described by Grudzen and colleagues of “physicians' attitude, knowledge, and beliefs” (see Fig. 3). Physician knowledge about the importance of PC consults for dementia patients was lacking. Representative quotes falling under “physicians' attitude, knowledge, and beliefs” based on our coding scheme are as follows: “This patient does not have a severe case of dementia” and “The patient is already in a nursing home, so they do not need a consult.” In addition, it was a common belief that once the patient is admitted, “The admitting physician will take care of initiating PC consults.” EPs also declined to initiate consultation because of their belief that the patient was not “end-stage.”

ED physician barriers to initiating palliative care consults.
Discussion
Dementia patients are at high risk for in-hospital death, and a growing number of people are dying from dementia. 20 Studies have shown that dementia patients frequently develop pneumonia, febrile episodes, and eating problems, all of which are associated with high six-month mortality rates.20–21 In addition, their distressing symptoms have a frequency and pattern similar to those in terminal cancer patients.4,21 Dementia patients frequently receive suboptimal end-of-life care, which includes burdensome interventions such as tube feeding or hospitalization for pneumonia; in some states up to 44% of nursing home residents with dementia die with feeding tubes in place.4,21–22 Given this evidence and growing support for integrating PC into the ED, we assessed the rate of PC consultations for AD patients presenting to the ED, and identified common barriers to physician-based PC initiation in the ED.
Overall, we reported a low rate of ED-initiated PC consults. Most AD patients meeting the screening criteria did not receive a consultation until after admission. However, prior to this intervention there were no ED-initiated PC consults, suggesting a small improvement from the baseline. In addition, we found that a large number of patients (27%) meeting the FAST criteria for AD were discharged. Given the potential benefits of PC outpatient services, it would be helpful to explore the use of these services for AD patients discharged from the ED. 23
Upon examining the barriers to initiating PC consults by trained EPs, the most frequent reasons for not initiating consults were categorized as physician attitudes, knowledge, and beliefs. EPs did not recognize the importance of initiating PC consults for AD patients. Our findings support those from other studies, though ours uniquely identifies barriers to PC for AD patients in real time. 24 This study demonstrates that the physicians continue to struggle viewing patients with dementia as dying slowly due to the gradual loss of cognition and function in this terminal illness. At the same time, clinicians need to actively understand that PC is not solely for the imminently dying. AD patients and families continuously face emotional and psychological challenges, including guilt related to withholding unnecessary treatments; PC services can guide patients and caregivers through these difficult times and decisions from the point of diagnosis. 4
Despite increasing interest in ED-initiated PC consults, we conclude that many preexisting beliefs, misconceptions, and a lack of knowledge persist in preventing physicians from initiating PC consults for AD patients. New models should be explored for addressing PC needs in AD patients, not relying solely on physician initiated interventions. Furthermore, although it was beyond the scope of our study, it would be helpful to compare clinical outcomes and perceived quality of life for AD patients with and without early PC interventions.
Limitations
This is a small, convenience sample at one suburban, academic ED. As such, findings may not be applicable in all settings. Although the majority of EPs received the educational intervention, we did not test their understanding or mastery of the material. In addition, all RAs received standardized training (see Methods), but we did not have the resources to validate the screening technique for all RAs by the PI. However, two trained, senior RAs had screening techniques validated by the PI and subsequently oversaw all RAs to ensure standardization.
Author Disclosure Statement
No competing financial interests exist.