
Abstract
Abstract
Background:
Pediatric palliative care (PPC) aims to promote quality of life for children and their families through prevention and relief of physical and psychosocial symptoms. Little is known about how PPC/hospice services impact health care resource utilization in an uncertain financial landscape.
Objective:
The study objective was to compare pediatric hospital health care resource utilization before and after enrollment in a home PPC/hospice program.
Design:
The study was a retrospective administrative data analysis.
Setting/subjects:
The study took place in a pediatric multispecialty hospital. Data were analyzed for 425 children ages 1–21 years who received home-based PPC/hospice services between 2000 and 2010.
Measurements:
Hospitalization and emergency room (ER) administrative data were examined to determine whether or not there were changes in total number of hospital admissions, length of stay (LOS), and hospital billed charges before compared to after PPC/hospice exposure.
Results:
There was no change in average total number of admissions pre-/post-PPC/hospice exposure; however, we found a significant increase in hospital/ER admissions for children with cancer diagnoses with longer exposure to PPC/hospice services. There were statistically significant reductions in LOS and total charges for hospital-based care; reductions were more pronounced in the noncancer group. Noncancer patients with at least six months of PPC exposure showed a significant decrease in total LOS from pre- to post-program admission by an average of 38 days, and an average decrease in total hospital charges of nearly $275,000.
Conclusion:
Enrollment in home-based PPC/hospice was associated with lower hospital and ER LOS and total hospital charges as compared with the period prior to enrollment for children with noncancer diagnoses.
Introduction
T
There is no standard insurance model for U.S. children, and public and private reimbursement practices vary, creating a barrier to access for many. In contrast to the majority of older adults, many children do not have public insurance coverage, and because they tend to live much longer than adults with palliative care (PC) needs, their benefits may be used up too quickly. 2 Each of the 50 U.S. states has its own version of Medicaid for children. Some progress was made in 2010 with the passage of the Patient Protection and Affordable Care Act (PPACA), which contains a new provision, Section 2302, called the Concurrent Care for Children Requirement (CCCR). It allows children receiving hospice to continue to receive services related to their medical condition without waiving their rights to concurrent care. 9
It is a widely held belief that PC pays for itself as a result of better pain and symptom management and treatment adherence. 10 There is a dearth of information about the cost of PPC delivery and whether or not PPC saves money by offsetting costs from ER visits and hospitalizations. There is some evidence in the adult PC literature to support the notion that palliative or hospice care services reduce or offset other costs during the final months of life,11–15 and even some evidence that PC increases survival time in recent adult studies.16–18 Similar studies have not been conducted in pediatric populations, and the few that do tend to focus on the end of life without examining prior resource utilization.19–21
Children with life-limiting or life-threatening illnesses experience substantially higher inpatient resource use, LOS, and technology-assistance charges compared to all other children who are hospitalized. 22 A small study looking at inpatient PPC costs reported those who received specialized PPC underwent fewer radiologic procedures and received better pharmacological services for symptom management. 21 Another U.S. study examined the cost of PPC during the last year of life for infants ($110,000) and children ($62,000) compared to adults ($28,000), showing PPC is more resource intensive. 23 The ideal way to track individual pediatric patient costs across time and multiple locations of care in the US is through the Medicaid and State Children's Health Insurance Programs (SCHIP). However, billed charges are often reimbursed by multiple private and public payers and sources, some of which are not easily captured via billing records or insurance claims data. Simpler methods may be the best approach to examining costs associated with PPC, such as LOS, intensive care unit (ICU) LOS, and hospital admissions. 15
Little is known about if and how PPC delivered in the home impacts medical service utilization and associated costs for children living with life-threatening conditions. Children's Hospitals and Clinics of Minnesota's (CHC) Homecare, Pain Medicine, Palliative Care & Integrative Medicine Programs combined represent one of the largest comprehensive home-based pediatric care services in the United States. In 2010, approximately 1480 children received care at home, of whom 141 received formal PPC and 29 received hospice care. Palliative/hospice home services emphasize 24/7 access and care coordination across children's medical and wider community (e.g., school) through home-based visits by nurses, social workers, child life specialists, chaplains, music/massage therapists, physicians, and volunteers. The primary goal of this study was to explore health care service utilization by children prior to enrollment in home-based PPC/hospice programs compared to the period after enrollment. Primary outcomes of interest included change in number of hospitalizations, LOS, and total billed charges for hospital/ER stays.
Methods
Data sources
Institutional review board (IRB) approval was obtained. All administrative data were captured through electronic medical record (EMR) systems CareFacts® (PPC/hospice) and Cerner® (hospitalwide): patient age; gender; race; date of death; primary and other treated diagnoses (ICD-9s); PPC program enrollment date and duration of time in program; and inpatient hospitalization data (e.g., length of stay; total charge per inpatient stay). Total charge per hospital visit was generated by SMS Invision (Malvern, PA) software as the sum of all billed charges incurred during the visit period, such as medications, room and board, and ancillary services. For patients with more than one admission to either PPC or hospice, we used the earliest program admission and first discharge date to calculate duration of time in program. All hospital admission records for the 12-month period preceding the PPC program start and the 12-month period after PPC program start were used to compute the number of hospitalizations, total LOS for each hospitalization, and the total hospital billed charges.
Discharges and readmissions that occurred within 24 hours of each other were counted as a single admission. We anticipated that utilization patterns would differ for patients with cancer versus noncancer patients so we coded patients as such, and adjusted for this as was done in a recent study of pediatric hospital admissions. 24 The International Children's Palliative Care Network's (ICPCN) 2011 list of most common diagnoses of children needing PC was used to create diagnostic categories (see Table 1). 25
56.0% (n=112) of cancer patients fell into ≥2 diagnostic categories, and 62.2% (n=140) fell into ≥2 diagnostic categories.
Includes Medicaid and Prepaid Medical Assistance Program (PMAP).
Sampling frame
Home PPC/hospice patients between the ages of 1 and 21 years old were identified and included if they initiated treatment for at least one day between 2000 and 2010 inclusive. Infants under one year of age were excluded, as data would not have been available for up to a full 12-month period preceding enrollment. This yielded a final sample size of 425 patients.
Statistical analysis
Analyses were conducted using SPSS 19.0 (SPSS Inc., Chicago, IL). Bivariate analyses were conducted using Wilcoxon signed-rank tests on outcome measures to determine significance between pre- and post-program admission. Multivariate analyses were conducted with generalized linear models using the generalized estimating equations option to assess the difference between pre- and post-PPC program enrollment outcome variables (i.e., number of hospital admissions, total LOS across admissions, and total hospital visit charges) while adjusting for patient-level variables like age, race, gender, “deceased” indicator, diagnostic conditions, and exposure to home PPC/hospice services.
Multivariate analyses were run separately for patients with cancer and non-cancer patients. “Exposure to home-based PPC services” was collapsed into the following categories: under 3 months, 3 up to 6 months, 6 up to 12 months, and 12 months or more duration. A Poisson regression in the form of a generalized linear model, with log link and Poisson distribution for the random component, was used to analyze the number of hospitalizations for each individual in the sample.
Total LOS and charge outcomes were more difficult to assess, because some subjects had no admissions (i.e., no LOS or charge data) while some subjects were hospitalized for the entire observational period. Separate regressions in the form of generalized linear models, with a log link and log normal distribution for the random component, were used to analyze total LOS and charge for each individual. We divided overall charges by a factor of 10,000 to reduce variability. Sensitivity analyses were performed by creating ordinal response variables, then running a conditional probit model to compare results.
Results
Patient characteristics are displayed in Table 1 separately for patients with cancer and those with noncancer diagnoses. Patients were mostly white, male, grade school age or younger, and had less than one year exposure to PPC/hospice care services.
Relationship between number of pre-post hospital admissions, home PPC/hospice exposure, and treatment for cancer
The average number of hospital admissions did not change significantly from pre-PPC program admission (3.09±3.6) to post-PPC (3.18±4.3) (Z=−0.616, p=0.538). A Poisson regression produced a significant three-way interaction between level of PPC exposure, patients treated for cancer, and study period (pre- versus post-PPC program admission) (p<0.001) while adjusting for other demographic and clinical characteristics. Specifically, cancer patients with the least amount of PPC/hospice exposure experienced a decrease in number of admissions, while those with the most exposure experienced an increase following exposure to PPC/hospice.
Relationship between pre-post total LOS, home PPC/hospice exposure, and treatment for cancer
A comparison of the mean total pre-PPC program admission LOS versus post-PPC program admission LOS revealed a significant drop by nearly two weeks from pre-PPC program admission (34.09±59.7 days) to post-PPC (19.37±34.0) (Z=−6.175, p<0.001). Multivariate regression of LOS produced a significant three-way interaction between level of PPC exposure, patients treated for cancer, and study period (pre- versus post-PPC program admission) (p<0.001). Specifically, noncancer patients with at least six months of PPC exposure showed a significant decrease in total LOS from pre- to post-program admission by an average of 38 days. Figure 1 depicts average LOS in days by duration of PPC exposure for patients with cancer and those with noncancer diagnoses.

Average LOS by PPC exposure for cancer and Noncancer patients.
Relationship between pre-post total charges, home PPC/hospice exposure, and treatment for cancer
A comparison of average pre- versus post- total charges revealed a significant drop by over $100,000 from pre-PPC program admission (20.97±43.3) to post-program admission (10.91±21.3) (Z=−6.581, p<0.001). Multivariate regression of charges produced a significant three-way interaction between level of PPC exposure, patients treated for cancer, and study period (pre- versus post-PPC program admission) (p<0.001). Specifically, noncancer patients with at least six months of PPC exposure showed a significant decrease in total billed charges. The average decrease in total hospital billed charges from pre- to post-program admission among noncancer patients with at least six months' exposure to PPC services was nearly $275,000. Total charges did not differ significantly for patients with cancer. Figure 2 shows average billed charges for hospitalizations before and after exposure to PPC/hospice services for patients with cancer versus those with noncancer diagnoses. Total charges across all hospitalizations decreased significantly for noncancer patients enrolled in PPC/hospice for at least six months.
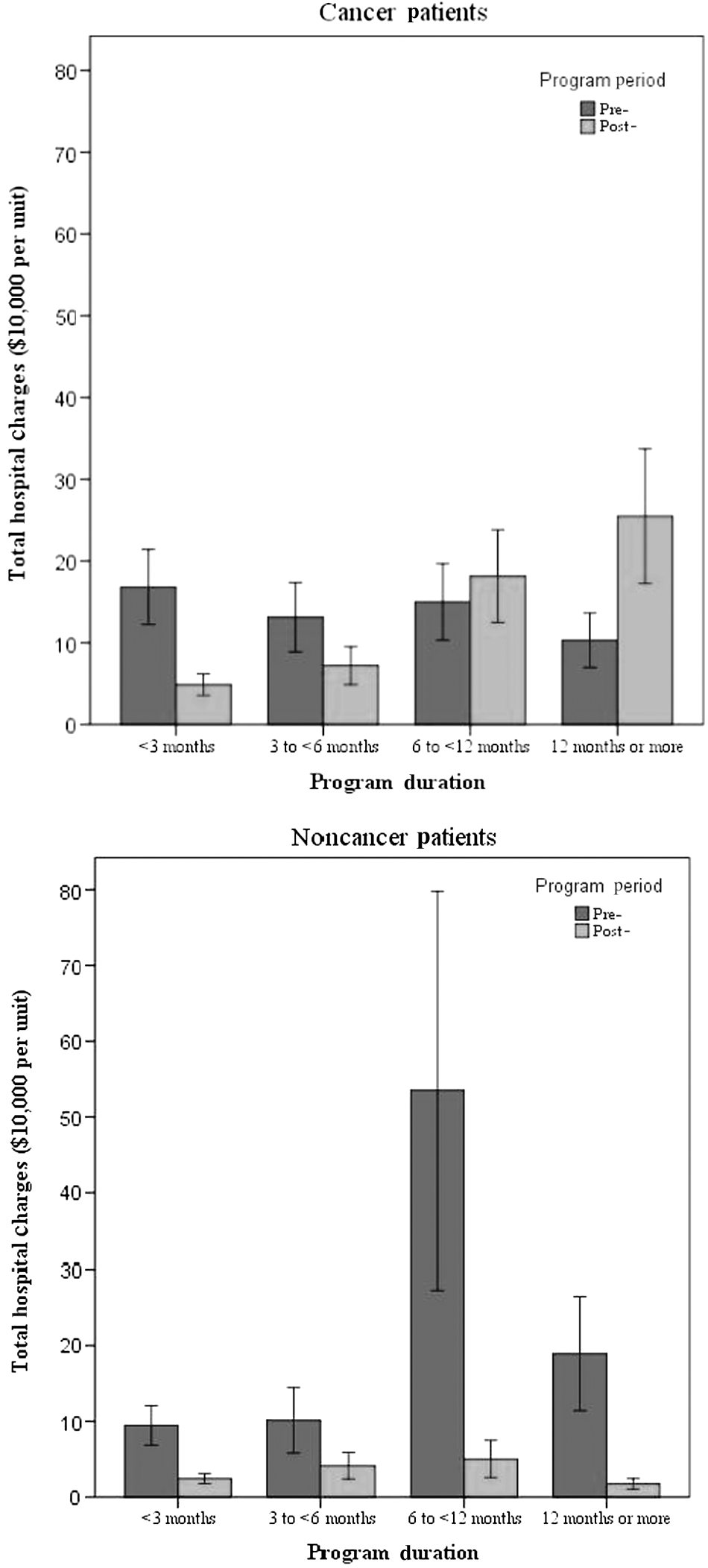
Average total cost of admissions by palliative care exposure and pre-post study period.
Discussion
The primary goal of providing PPC to children and their families is not to save money for the health care system, but rather to ensure that children with serious illnesses live as long and as well as possible. At times of increasing scrutiny around the implementation of advanced care models such as PPC, we often find ourselves making a “business case” to administrators. Results from this study showed that PPC home care reduces total hospital LOS and it may result in a reduction in billed charges. Under the previous U.S. “fee for service” model, this would have been considered financially disadvantageous. With the shift toward diagnosis-related group (DRG) and accountable care organization payment structures, these savings are often advantageous for medical institutions.
More than two-thirds of U.S. children with palliative care and hospice needs have an underlying nonmalignant condition. 26 The largest decreases in resource utilization post-PPC/hospice enrollment were seen for the 225 children in the noncancer group. Average LOS decreased by an average of 38 days, and total hospital charges decreased by an average of $225,000 for patients exposed to PPC/hospice for at least six months as compared to the period before PPC/hospice exposure. These reductions are substantial. Some have speculated that children who receive comprehensive PPC services may avoid unnecessary hospitalizations due to routine monitoring, care continuity, and advanced pain and symptom management. It might be possible that children receiving palliative home visits are better prepared for preventing and managing distressing symptoms at home when they arise, and for averting crises resulting in acute admissions. Finally, because we did not see a significant decrease in frequency of hospital or ER admissions for the noncancer group from the period before PPC/hospice exposure compared to the period after, we can speculate that the benefit of PPC and hospice may come in the form of better care coordination, resource management, and technology avoidance while patients are in the hospital. We can further speculate that LOS does not appear to be a proxy for number of admissions in this noncancer population.
The pattern of reduced LOS and billed charges in the post-PPC/hospice period seen in the noncancer group was not found for the group of patients with underlying malignancies. Instead, the average total number of admissions increased significantly for cancer patients enrolled in the PPC/hospice program for over 12 months. This was not surprising, since cancer treatment protocols almost always involve planned inpatient stays for chemotherapy or other treatment administration and symptom management. There also may have been a referral bias towards home PPC and hospice for children who were more symptomatic.
Limitations
There were several limitations in this study. First, we were unable to examine the complete picture of health care utilization, because we accessed hospitalization and ER visits within a single institution. Despite this, the children that were included in this study had an established record of medical care at CHC prior to PPC/hospice enrollment, making it more likely that they would be treated again at the same institution following PPC/hospice enrollment. Further, CHC discharges the vast majority of pediatric patients in the metro area of Minneapolis/St. Paul, Minnesota.
Another limitation was the lack of access to a control group of children with PPC needs that were not referred to the PPC/hospice programs. It should be noted that some children had more than one admission to PPC/hospice during the 2000–2010 study period, so we chose to select the first admission only. It is likely that some of these children were discharged and re-exposed to PPC/hospice services during the follow-up period (i.e., they did not have continuous services), and that the additional services they received impacted health care utilization that was not accounted for in the analysis.
The analysis did not account for inflation or variables that were unattainable from EMR or billing data, such as lost time from work for the patient or family, reduced quality of life, increased stress, etc. For ER visits, providers' professional fees are lumped together with all other charges for the visit; for inpatient visits, professional fees are billed separately and data is not available for patients seen prior to 2004, so we did not include professional fees for inpatient stays in the analysis. Therefore, inpatient stay total charges are underestimated for many patients in the sample. Another limitation is that we did not capture information about which children received additional extended hours nursing services from an outside agency, on top of CHC's PPC/hospice services. However, we estimate that less than 10% of children in the sample would have received these additional in-home nursing services, and few, if any, would have continued to receive them upon enrollment. It is possible that the extra medical care and attention these children received contributed to the reduction in LOS and hospital charges seen in the noncancer group.
Though the regression model accounted for hospitalizations during the year prior to PPC/hospice exposure, we do not know what circumstances led them to PPC/hospice enrollment, or whether there was a referral bias. This would have provided a clearer picture of why children were referred at the time they were. Finally, we had access to five current procedural terminology (CPT) codes per admission, and it was outside the scope of the current study to further classify and analyze these codes. If combined with DRGs, the information might have provided insight into the general reasons for and types of admissions as they relate to total charges.
Conclusion
Results from this exploratory study suggest that there is an association between exposure to home PPC/hospice services and reduced inpatient stays and related charges. Children enrolled in CHC's PPC/hospice programs with noncancer diagnoses experienced a significant decrease in average total hospital LOS and total billed charges for hospitalizations following program enrollment compared to the period before enrollment. This effect was seen for children with noncancer diagnoses that were enrolled in home PPC/hospice for six months or more, but was not seen for children treated for cancer.
Future studies should examine total cost of health care utilization for children with life-threatening conditions using a single payer administrative dataset (e.g., Medicaid) and a comparison group, such as children with PPC needs who did not receive services. Home-based PPC/hospice is not only the most advanced form of care for children with serious illness, but for children with nonmalignant diseases it may also be cost saving. In the current health care environment, this is advantageous to pediatric health care institutions and insurers alike.
Footnotes
Acknowledgments
We wish to thank Dr. Sheila Payne, Dr. Rob Payne, and Dr. Andrew Flood for their thorough reviews.
Author Disclosure Statement
No financial support was provided for this study. No competing financial interests exist.