
Abstract
Abstract
Background:
Patients with severe chronic obstructive pulmonary disease (COPD) experience substantial symptom burden, psychological and social morbidity. The experience of this illness has an impact beyond the patient.
Objective:
This study seeks to understand the experiences and needs of family carers of people with severe COPD.
Design:
Semistructured interviews were held with current and bereaved carers of people with severe COPD. Several areas of content were targeted in the interviews, including the experience of caring for someone with COPD, views of treatment and prognosis, information and communication needs, and the understanding of palliative care. Data were analyzed thematically.
Results:
The carers' and bereaved carers' experiences and needs around COPD are best understood as a dynamic of change, recognition, and adaptation. Carers faced many changes as the patients' general condition deteriorated. These were changes in the nature of caring tasks, in their relationships, and their own expectations. Carers usually recognized change had happened and sought to adapt through new approaches, new equipment, a new stance of thinking, and in most cases, continued caring. Within this theme of change, recognition, and adaptation were a series of subthemes: (1) the impact of caring, (2) recognizing the role of the carer, and (3) the needs of the carer including their needs from palliative care services.
Conclusion:
The impact of caring borne by family carers is substantial and life changing. Health professionals may assist carers in their role through acknowledgement, facilitating recognition of the changes that have occurred (and their implications), and enabling creative adaptive responses for carers. Such assistance is likely to enhance the ability of carers to continue in this demanding role.
Introduction
C
The impact of COPD extends beyond the patient, and the effect on family carers is increasingly recognized. In Australia one third of those sampled in a population study had someone close to them die in the last five years, and of these, in 10% of cases the cause of death was COPD. 13 More than one fifth provided physical hands-on care. 13 International insights on the experience of family carers reveal they face uncertainty around the changes occurring day-to-day and what the future holds, fear associated with acute exacerbations, and a substantial impact on their own health as their world ‘implodes.’ 14 Carers also report gaps in knowledge about COPD, the illness course, and palliative care. 15 There are fewer data describing the experiences of caregiving in an Australian context and the needs and information requirements, particularly towards the end of life.
The aim of this study was therefore to explore the experiences of current and bereaved informal carers of patients with severe COPD with a particular focus upon their information needs and views of palliative care.
Methods
Consistent with the exploratory aims of the study, in-depth, semistructured interviews were held with English-speaking carers, both current and bereaved, of patients with COPD. In Australia, patients with severe COPD admitted to hospital are commonly subsequently seen in outpatient clinics. Therefore, consecutive patients with severe COPD attending tertiary respiratory outpatient clinics were approached and asked to nominate a carer who was in turn invited to participate. Severe COPD was defined as requiring hospital admission for an exacerbation in the previous six months, 16 and current carers were defined as those persons nominated by the patient, and verified by the carer, as regularly providing some level of assistance in daily life. This ‘level of assistance’ was defined by the patient as a task for which they required help, and may have varied considerably, ranging from driving to appointments, through to help with dressing, toileting, and mobility. Bereaved carers of patients treated in the respiratory unit who had died between 6 and 24 months previously were identified by the treating physician and were contacted by letter explaining the study and inviting participation with an opt-in clause. Those who made contact were given further information about the study and if consenting, were interviewed at a location of convenience.
Several areas of content were targeted in the interviews, including the experience of caring for someone with COPD, views of treatment and prognosis, information and communication needs, and the understanding of palliative care (see Appendix 1). All questions were framed to elicit the narratives of carers which would in turn reveal their experiences of caring. While questions guided the discussion, flexibility was maintained to enable the interviewer to follow up on particular concerns raised, consistent with the exploratory aims of the study. A single interviewer experienced in nursing and palliative care undertook all interviews.
All interviews were audiorecorded, transcribed verbatim, and then thematically analyzed by three investigators (JP, CB, MG). This process involved the transcripts being individually read and ‘open’ coded, with documentation of ideas that were subsequently grouped into categories according to shared meanings and content. In turn, these categories were further abstracted and grouped into themes. 17 The emergent themes were collectively discussed and refined, with points of difference examined and eventual agreement of themes reached. These were then reviewed by the remaining investigators, with feedback incorporated to reach the final themes and to ensure consistency and cross-validation of the results. The study was approved by the institutional research and ethics committee.
Results
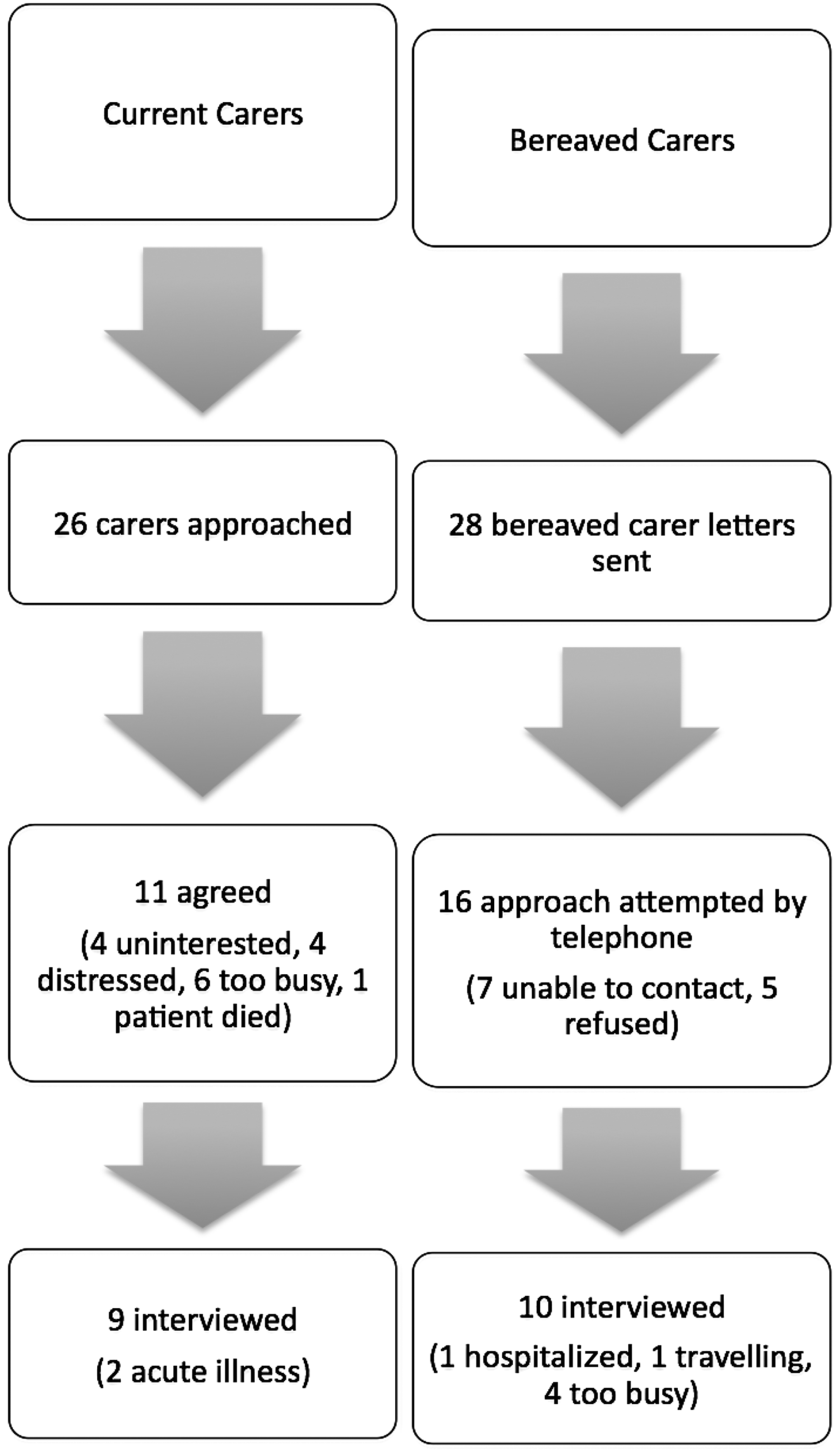
Interviews were conducted with 9 current and 10 bereaved carers at which point data saturation was reached (see Fig. 1). Interviews ranged in length from 35 minutes to 85 minutes (median 65 minutes). The carers' characteristics are listed in Table 1. The carers' and bereaved carers' experiences and ideas around COPD are best understood as a dynamic of change, recognition, and adaptation. Carers faced many changes which paralleled the deterioration of the patients' conditions. These changes had a direct impact upon the carers in terms of the caring tasks required, their relationships, and their expectations of their own lives. Examples of these changes included needing to spend increased time at home with the patient; fewer outside social contacts; and assisting with showering, dressing, even toileting. The carers generally recognized that these changes had occurred and sought to adapt to them, incorporating new approaches or new ways of thinking, and in most cases continued caring. It appeared that the recognition of change and its enduring nature was necessary in order that adaptation may take place. Within this theme of change, recognition, and adaptation were a series of subthemes: (1) the impact of caring, (2) recognizing the role of the carer, and (3) the needs of carers in order to continue caring including their needs of palliative care (see Table 2).
Study sample.
The personal impact of being a carer
Both current and bereaved carers described how their role had evolved gradually. They had begun doing small tasks such as driving to appointments, but over time the tasks became progressively and inexorably more time consuming, onerous, and intimate in nature. This evolution occurred over many years. Coupled with this increase of time and energy devoted to caring, a series of social changes occurred for the carers. These were changes in the nature of the relationship with the patient who at times became irritable and demanding, and also in the carers' relationships outside the household, since the carer had less time to pursue interests outside the house. These social changes appeared to be related to the degree of the patient's dependency and the length of time caring had been required.
It got to the stage where I would have to get her out of bed, take her to the toilet…and I hated doing that.…I'd never thought I'd be…doing anything like that. (Bereaved Carer 10=BC#10)
I used to embroider, I used to do family trees…but that has fallen absolutely apart.…At night I have been so tired I could hardly read the paper. (C#9)
You know I want to listen to the radio but he doesn't. I haven't got a life. It's not my life. It's living for him really. (C#4)
The responses of the carers to these changes were ambiguous and complex. The carers reported honoring the patients' endeavours to maintain independence, but were mindful that this often had a negative impact upon their own lives and their capacity to care. They juggled competing emotions of loyalty, resentment, guilt, and exhaustion.
It is very frustrating, and you know I don't know if the government realizes how hard it is for carers.…It's a full-time job. It's work isn't it? It's not something you do because you like it. I mean I care for my Dad, I love him and I want to look after him, but I also need my own time. (C#4)
Recognizing the role of the carer
The role of carer developed by default as the progressive changes and increasing disability occurred for the patient. Carers described a lack of choice, even for some, a lack of awareness, until they suddenly realized they were fulfilling a significant caring role. In addition to providing daily physical assistance to the patient, some carers described being the ‘keeper’ of the patient's medical history, being an advocate for the patient particularly at times of acute illness, and being the main decision maker particularly around when to go to hospital for an acute exacerbation. For some, recognizing and embracing these roles was a source of pride.
They ask her questions and she's struggling for breath, and she doesn't remember dates and…I do. (C#2)
I said she's not improving much, doctor.…She had the bipap here before when she was about this stage and the nurse said, Yeah that might be a good idea, and the doctor put the bipap on.…You feel as if you're interfering but you know you've got an opinion, give it. (C#2)
The needs of carers in order to continue caring
The carers readily detailed a number of areas of need which, if addressed, would have assisted care provision. Some of these needs were for equipment, some for disease-specific information, and some were relevant to care towards the end of life—what may be considered aspects of palliative care.
As carers recognized the changes that had occurred, they detailed practical aids that would have assisted them. These practical responses assisted with adapting to the role of caring. These included equipment to assist mobility, showering, and outings. They suggested that ‘outside’ people to assist with household tasks, shopping, and nursing tasks were helpful but were usually only acceptable to the patients if provided by consistent personnel and preferably a single person. Therefore the patients often declined available assistance, which the carers would have embraced. The carers also emphasized the value of a response plan in the event of an acute exacerbation, including at what point hospitalization should be sought.
As I say, you don't know, do you?…You've probably got to talk about it. What if a decision had to be made?…At the moment he's very lucky, but if we had an emergency and…it's life threatening, well that would have to be my decision. I'm not sure what I would say. I don't know. We haven't talked about it. (C#7)
Information was highlighted by both current and bereaved carers as a practical way of assisting carers in their role. This information was required from medical staff and preferably senior medical staff whom they knew and trusted. The carers understood this required some commitment of time but felt that priority should be given to communication tasks with carers, since such information was necessary to continue care. They detailed that such information must include education about the disease and its treatment and prognostic and future planning information (though this had not occurred for any of the bereaved carers except in the final few days of life). A number of the bereaved carers described their surprise when told their loved one was close to death.
Yeah that was what surprised us. How the guy…talked to us as if he thought that we knew that this was, you know…he was coming to an end. And we didn't. (BC#1)
For medical staff to be providing information reduced the pressure on the carer to be raising negative information such as need for additional help or need to plan for the future. Importantly, carers believed that their needs for information may differ from the patients' needs for information, but nevertheless they saw their need as important in their own right. It appeared that information was essential to plan and in effect to adapt to the changes being negotiated.
It's [information] got to come from the doctor attending. He's the one that's made the decisions, made the examination.…He's the one that should be telling the patient this sort of information. (BC#6)
I'd love you to raise [discussions about prognosis, care preferences] with her.…I feel sometimes she feels that I'm pressuring her…I think coming from someone else. It might be a little different. (C#8)
What would have been helpful and comforting for me [is] to have been fully informed. [The patient] didn't always want to think about it, but I needed to so I could work out what to do. (BC#1)
Carers were mostly unfamiliar with the term palliative care, but expressed interest in components of the approach, most particularly open communication, discussions around prognosis, goals of care, as well as support for the family in addition to the patient. They reported quality of life as the important goal of therapy. Some differences did however emerge between current and bereaved carers. Bereaved carers strongly indicated that all components of palliative care had relevance in their caring experience. Current carers were generally more circumspect in their support for components of palliative care, wishing for additional information but nevertheless remaining keen to uphold the stance of optimism that patients reported. 11 It appeared that bereaved carers saw palliative care as part of an adaptive response to caring, but this was not the case for those currently immersed in the imperatives of day-to-day caring.
I don't know much about it [palliative care]. I've had nothing to do with it but…I just don't like the idea of those places myself. (C#6)
I think it really again focuses down to the palliative care aspects, to…just be informed so he can try and get a better handle on the situation. (C#3)
Discussion
This study provides insights into the experiences and perceived burden of those providing care to people with severe COPD in Australia. The findings evoke the burden borne by the informal carers of patients with COPD who take on substantial physical, emotional, and social tasks often over many years. This lengthy period of caregiving has been described by Currow and colleagues who determined the average length of informal caring for those with end-stage lung disease was 40 months. 13 The carers in this current study simply took on what were initially small tasks but which over time became more onerous, until ultimately the patients were fully reliant upon carers to remain home. While the carers frequently did not choose to provide care, for many there was no alternative. The health system relies heavily upon carers adopting this role.18–20
Provision of such care does not come without considerable personal cost. This study confirms the findings of others that carers of patients with COPD, similar to carers of cancer patients, feel anxious, fatigued, frustrated, isolated, and unprepared for their role and the decisions they must make.15,21–24
The study revealed an important dynamic that evolves for carers, consisting of changes occurring during the COPD illness, the explicit recognition by the carer of such changes, and for some, a subsequent adaptive response. The possibility of adaptation appears to be important to the ability to provide care over the long term. Such adaptation may be practical in nature, such as the use of equipment, or may be psychological, such as planning for the future, engaging in decision making, or developing a plan for emergency responses. Others have similarly highlighted adaptive responses of carers of those with COPD to include sharing the responsibility for caring with the patient, ‘getting on with it,’ and using information and supports;10,14 while resonances of an adaptive response are evident in reports of ‘acceptance’ and a ‘way of life’ when describing the debilitating symptoms of a long-term condition. 9
While caring was clearly burdensome, satisfaction in the role was also evident, such as when a clear direction or role was successfully fulfilled. Janssen and colleagues have described the positive aspects of family members providing care for patients with advanced organ failure, including a subset with COPD. 25 While they determined that overall appraisals for caregiving and family well-being were positive, those caring for someone with COPD were more likely to have carer strain than other groups. 25
It may be that a positive caregiving experience is more likely for those carers who had explicitly recognized that changes have occurred, acknowledged their likely irreversible nature, and subsequently adapted their thinking and behavior. Hudson has highlighted the applicability of the modified stress-coping model to describe the experience of family carers. 26 In this conceptual model, positive emotions were possible despite an ongoing stressful event. These positive psychological states were noted to be achieved by finding a sense of meaning, by developing goal-directed problem-based coping, and through spiritual belief. 26 It is with use of this conceptual stress-coping model that the possibility emerges of enhancing adaptive coping and therefore adaptive caregiving. 26 Specifically, by providing adequate information for carers, anticipating problems including emergencies, developing responses to such problems, and providing carers with emotional and psychological support, the task of caregiving may be enhanced.
A series of interventions have been developed to assist the adaptation of family carers of cancer patients, including enhancing problem solving and coping skills, 27 education and support,28,29 cognitive behavioral and symptom management approaches, 30 relaxation techniques, 31 and self-care strategies. 32 Each of these interventions implicitly recognizes the important role that the carer plays, their legitimate needs to undertake that role, and attempts to provide strategies and support to address such needs that have arisen due to the changed circumstances. 33 Importantly, formal evaluation of family carers following the various interventions suggests improved quality of life, mood, self-efficacy, and greater rewards associated with providing care. 33 Most intervention studies in this area have been undertaken with family carers of people with cancer, with very limited data available for carers of people with COPD. While substantial similarities exist in terms of needs, 34 there are also important differences, such as the nature and chronicity of the COPD illness and hence the caregiving task. Interventions to assist family carers of COPD must be nuanced and responsive to the particularities of the suffering entailed.
Outside of formal intervention studies and programs, this study holds implications for health care professionals caring for those with COPD. Health care professionals have a role in the act of recognition of the needs of family carers, and thereby facilitating an adaptive response. Such recognition may take a number of forms: simple verbal acknowledgement of their role and tasks, inclusion within the consultation as a partner in care provision, direct inquiry into carers' needs, and more formal interventions to assist family carers. 33 Carer recognition, identification of needs, and a response to address such needs will facilitate adaptation. The carers in this study have described a number of means, including practical, information based, and psychological by which they may be assisted in adaptation within routine clinical care.
There are limitations to this study. Carer identification was based on patient and physician report, and it is possible that not all relevant carers may have been sampled. Further, this study is limited to reporting the views of those interviewed, which may not represent the wider community of carers. The methodology, however, was designed to explore a range of views and determine the possibilities without preconceived ideas. Ascertaining the generalizability of these data should be the subject of future research employing different, quantitative methods.
Conclusion
The experience of caring for someone with COPD has profound implications for the well-being and relationships of those providing the care. The caring experience is rarely chosen, and the carer often neither acknowledged nor supported by health systems. The dynamic of experiencing change, recognizing such change, and developing an adaptive response is important for family carers. Physicians need to actively acknowledge and engage with carers alongside patients with COPD, proactively identifying and responding to needs, providing support, and facilitating adaptive caregiving. To fail to do so not only increases the burden upon the individuals involved, but also, given our dependency upon these carers continuing their task, for the broader health system.
Footnotes
Acknowledgments
This research project was funded by a project grant from the Bethlehem Griffiths Research Foundation. The authors wish to acknowledge the contributions of Anne Harbison and Suzanne Graham to this project.
Author Disclosure Statement
No competing financial interests exist.