
Abstract
Abstract
Background:
It remains unknown whether the end-of-life (EOL) environment influences survival after anticancer treatment, particularly for gynecologic malignancy.
Objective:
The study's objective was to clarify whether the survival time varied depending on where patients spend the EOL.
Methods:
This retrospective study included patients who received initial oncologic treatment but died due to cancer recurrence and/or progression. The subjects were a cohort of 181 gynecologic malignant tumor cases in a single institution from 2002 to 2008. Measurement was of postcancer treatment survival (PCS), defined as the time interval between the last date of anticancer treatment after recurrence/progression and death from the disease, analyzed on stratification by type of supportive care or where patients spent the EOL.
Results:
The median survival time was 26.1 (1.0–306.4) months. The distribution of the carcinoma type was as follows: 28.7% of patients with cervical (N=52), 27.6% with endometrial (N=50), and 43.1% with ovarian (N=79) cancer. The median PCS was 13.3 weeks. Patients in the hospice/home care group showed a significantly more favorable PCS than those in the hospital group (log rank: P=0.029). On multivariate analysis, the age (<60 versus ≥60) and site of supportive care (hospital versus hospice/home care) retained their significance as independent prognostic factors of poor PCS (age: HR=0.679, 95% CI, 0.496–0.928, P=0.0151; site of supportive care: HR=0.704, 95% CI, 0.511–0.970, P=0.0319).
Conclusions:
Our current data could be hypothesis generating; it is possible that the EOL environment is a crucial prognostic factor for survival after anticancer treatment.
Introduction
G
Methods
Patients
A retrospective review of all gynecologic cancer patient deaths from 2002 to 2008 at Nagoya University Hospital was performed. The study population included patients who received initial oncologic treatment at our institution but died due to cancer recurrence and/or progression. This study was approved by the ethics committee in Nagoya University. Patients were excluded from this study if they had insufficient clinical data, a history of other malignancies, no information on cancer recurrence or death not attributed to gynecologic cancer, or were lost to follow-up immediately after the initial treatment. A variety of clinical records were collected, including demographic data, cancer diagnosis, treatment type, further treatments if there was recurrence or progression at diagnosis, the type of supportive care, where patients spent the EOL, and the date of death. Pelvis invasion was defined as the presence of a deeply invaded tumor in the pelvic organs and/or retroperitoneal cavity, excluding superficial peritoneal dissemination. Maximum opioid use was calculated as the oral morphine intake. The calculation formula of each equianalgesic dose to oral morphine based on 24-hour opioid requirements was as follows: parenteral morphine (1:2), modified-release oxycodone (20:30), transdermal fentanyl (1:30), parenteral fentanyl (0.6:0.60), morphine suppository (40:60).
Survival analysis
Postcancer treatment survival (PCS) was defined as the time interval between the last date of anticancer treatment and death from the disease. Furthermore, intracancer treatment survival (ICS) was defined as the time interval between the date of initial treatment and the last date of anticancer treatment. In this context, “cancer treatment” included initial/cytoreductive/salvage surgery, any chemotherapy, and/or aggressive radiotherapy, but excluded palliative irradiation. Regarding where patients spent the EOL, we divided all patients into four cohorts: university hospital, general hospital, hospice, and home care groups. The university hospital cohort included patients who continuously received anticancer therapy and subsequent palliative care from initial treatment until death in Nagoya University Hospital. Each general hospital, hospice, or home care cohort included those who received primary therapy and thereafter were referred/moved to a neighboring general hospital, hospice, or home care at the cessation of the anticancer treatment, respectively. The survival curves were based on the Kaplan–Meier method and compared employing the log rank test. Furthermore, we analyzed the PCS and ICS on stratification to two subgroups: the hospital group (university/general hospital) and hospice/home care group. Multivariable analysis was carried out with the Cox proportional hazards model to evaluate independent factors affecting survival. A P-value of <0.05 was considered significant.
Results
Patients' characteristics
The clinical characteristics of the 181 patients enrolled are described in Table 1. The median survival time was 26.1 months, range 1.0 to 306.4 months. The median age at the end of aggressive cancer treatment was 58 years old (21–84 years). When we classified patients into the two subgroups on stratification by the age near the median value, <60 years in 98 (54.1%) patients and ≥60 years in 83 (45.9%) patients. The distribution of carcinoma types was as follows: 52 (28.7%) with cervical, 50 (27.6%) with endometrial, and 79 (43.1%) with ovarian carcinomas. Pelvis invasion was positive in 68 (37.6%) and negative in 113 (62.4%) patients. In 152 (84.0%) patients, an opioid was used for pain control. As the converted oral morphine intake, the medium value of maximum opioid use was 24 mg. Thus, when we divided patients into the two subgroups on stratification by the maximum opioid use, the distributions were as follows: ≤25 mg in 63 (34.8%) patients and >25 mg in 89 (49.2%) patients. In addition, regarding where patients received EOL supportive care, 118 were in the hospital group (65.2%) and 63 in the neighboring hospice/home care group (34.8%).
All intakes were converted to oral morphine.
Analyses of intra- and postcancer treatment survival
Figure 1 shows the PCS curve of all patients. The median ICS and PCS were 88.1 and 13.3 weeks, respectively. On stratifying by the maximum opioid intake, the PCS of patients who received ≤25 mg did not significantly differ from those who received >25 mg (log rank: P=0.301) (see Fig. S1). Figures 2 and 3 show ICS and PCS curves, respectively, on stratification by where patients received EOL supportive care. With regard to the ICS, the curves mostly overlapped, and we did not identify a difference between patients in the hospice/home care cohort and those in the hospital cohort (log rank: P=0.6196) (see Fig.2). In contrast, patients in the hospice/home care group showed a more significantly favorable PCS than those in the hospital group (log rank: P=0.029) (see Fig. 1).
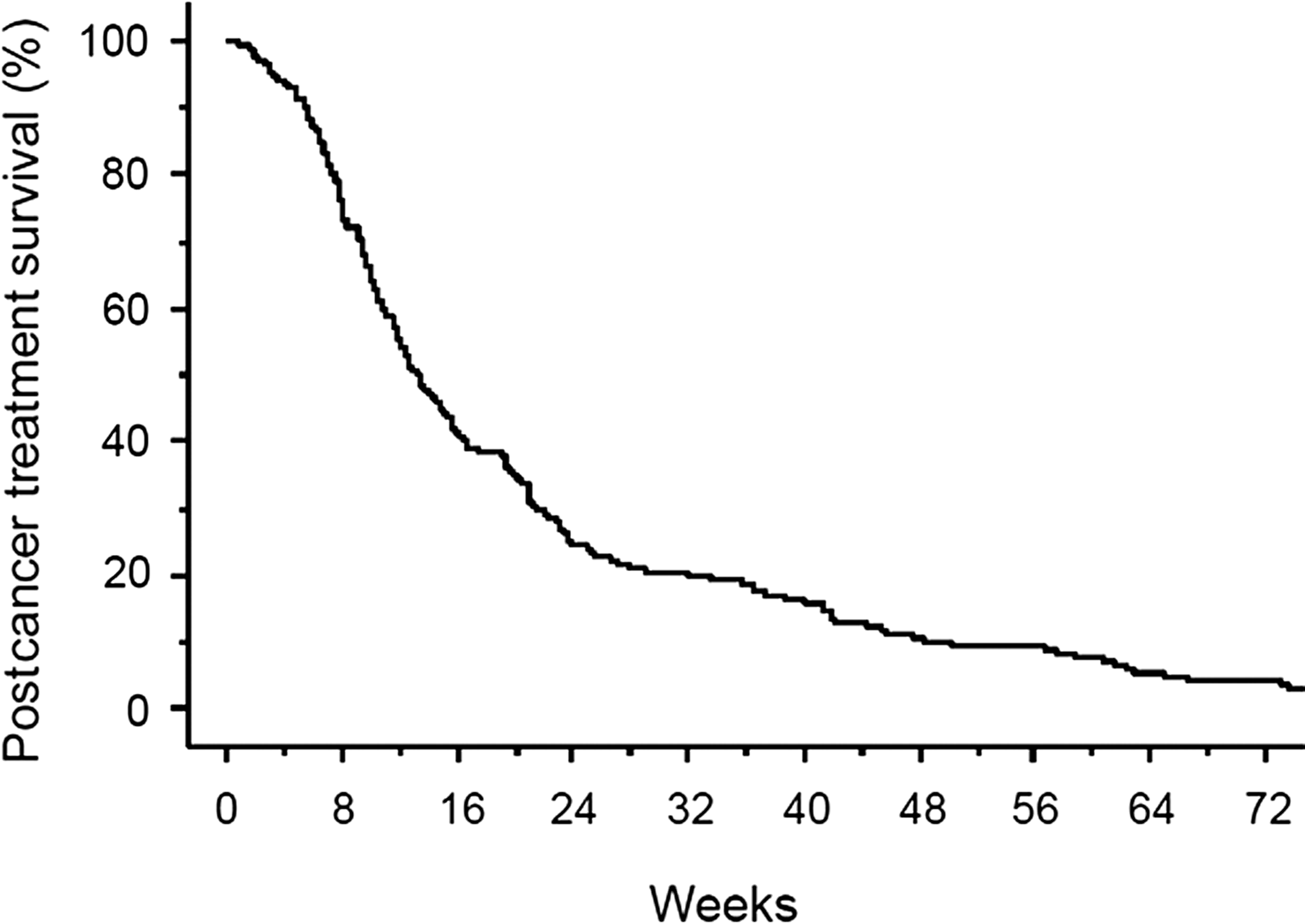
Kaplan-Meier estimated survival after anticancer treatment (PCS) of all 181 patients with gynecologic malignancies.
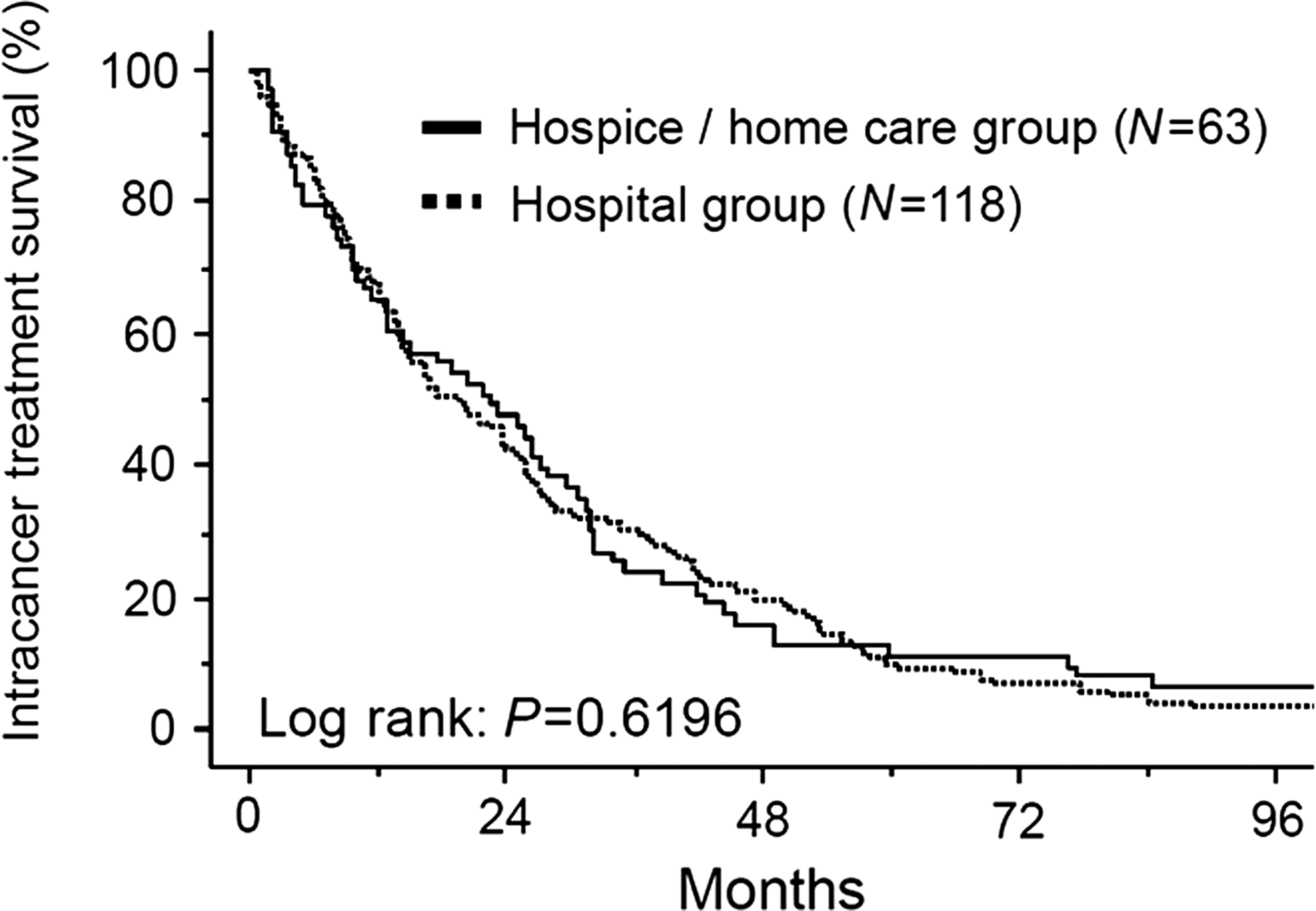
Kaplan-Meier estimated ICS of patients on stratifying by the EOL site.

Kaplan-Meier estimated PCS of patients on stratifying by the EOL site.
Distribution of palliative treatments
We subsequently examined whether EOL medical care differs between the two above-mentioned EOL site cohorts. Table 2 shows the distribution of various palliative applications, including pain control, intravenous hyperalimentation, thoracentesis/paracentesis, nasogastric/ileus tube, ureteral stent/nephrostomy, blood transfusion, oxygen inhalation, sedation, and colostomy/intestinal bypass. On stratification to the two EOL site cohorts, there was no significant difference in the distribution of all palliative treatments excluding colostomy/intestinal bypass (see Table 2).
Multivariable analyses
Cox multivariable analysis was conducted to simultaneously examine the independent effect on PCS and eliminate selection bias from a number of clinicopathologic factors as thoroughly as possible. The age (<60 versus ≥60), carcinoma type (uterine versus ovarian), pelvis invasion (positive versus negative), maximum opioid use (≤25 mg or none versus >25 mg), and site of supportive care (hospital versus hospice/home care) were entered into the analysis (see Table 3). Consistent with the results of univariable analysis, the age and EOL site retained significance as independent prognostic factors in poor PCS in the multivariable model (age: HR=0.679, 95% CI, 0.496–0.928, P=0.0151; EOL site: HR=0.704, 95% CI, 0.511–0.970, P=0.0319) (see Table 3). Therefore, patients who spend the remainder of their lives in a hospice/their own home showed a significantly longer PCS than those at a hospital in both uni- and multivariable analyses.
Cox Hazard Model, bAll intakes were converted to per os morphine. cConverted dose to oral morphine intake
Discussion
Palliative care is an essential approach to cancer care that, along with symptom control, focuses on aspects of life important to patients and their families in an attempt to protect and relieve suffering.8,9 According to a previous report, an earlier introduction of palliative care led to significant improvements in the quality of life (QOL). In the present study, using novel prognostic parameters: ICS and PCS, we revealed that patients in the hospice/home care group show a significantly more favorable prognosis after aggressive anticancer treatment than those in the university/general hospital group. Although this difference may merely reflect disease characteristics rather than an essential survival advantage in the former group, we thought that the quality of the EOL of the former group was inferior to that of the latter. Indeed, there was a likelihood of selection bias and treatment heterogeneity, since our cohort included the limitations associated with any retrospective study. As such, we determined three major causes of bias: (1) duration of aggressive treatment, (2) difference in various accompanying palliative treatments, and (3) multifactorial effect of several clinicopathologic indicators. First, there may be a tendency whereby the therapeutic interval between the initial to final aggressive treatment was longer in the hospital than hospice/home care group. In the current analysis we examined whether there was a difference in the survival duration between the date of initial treatment and the last date of anticancer treatment between the two groups. However, contrary to our expectations, such intervals did not significantly differ between the two EOL site cohorts. Regarding the second possibility, we wondered whether or not hospital patients were more likely to undergo intensive medical care and an invasive procedure based on their inherent disease progression. If so, the remaining oncologic outcome of those patients may become biased, resulting from a poorer and more severe general condition. In this regard we examined the distribution of various medical treatments between the two groups, including palliative surgeries and encompassing best supportive care. Nevertheless, we did not identify any significant difference in the distribution pattern of most palliative interventions, even regarding the amount of opioid use. To eliminate the third possible bias as far as possible, we conducted a multivariable analysis, including the age, carcinoma type, recurrence pattern, maximum opioid use, and EOL site. Consequently, we identified the EOL site as an independent prognostic factor for survival after aggressive cancer treatment.
Despite the fact that the survival duration until the final aggressive treatment and subsequent palliative modality were almost the same, we identified a survival benefit in patients in the hospice/home care group compared to the hospital group. Connor and colleagues retrospectively analyzed the survival of 4493 patients with congestive heart failure and five types of malignancy, including breast, colon, lung, pancreatic, and prostate cancer, on stratification by hospice use/nonuse. For the six patient populations combined, the mean survival was 29 days longer for hospice than for nonhospice patients. 6 Moreover, according to a previous study from Keyser and colleagues, in a subset of 81 patients with recurrent gynecologic malignancies the median overall survival for 29 nonhospice patients was 9 months versus 17 months for 52 hospice patients, and this difference was significant. 10 Neither examination suggested any adverse effect on survival for hospice patients.
In multivariate analysis of our study, the extra-hospital care was an independent prognostic indicator. If the extra-hospital care even partially contributes a survival benefit, what is a possible reason? Assuming that the medical care for terminally ill patients was the same between the two groups, mental QOL was likely to be higher in those in an extra-hospital environment. Indeed, a prior study reported that QOL influences survivorship in cancer patients.11,12 Probably, mental satisfaction and peace of mind related to the extra-hospital care may result in enrichment of patients' lives and may have a positive effect of improving survival, although this is a hypothesis. In this context, we think that further psychosocial factors should be considered in both cohorts, including family accompanying status, religious outlook, and philosophy about death. We hope that these additional factors will be adequately evaluated in a future prospective study. Many patients did not demand the cessation of chemotherapy, even immediately before the worsening of the general condition, either for reassurance or because they and their oncologist believed the continuation of such treatment to be fundamentally beneficial for their remaining life. However, counseling patients on EOL decisions is crucial for both doctors and families, although it involves marked difficulties. Patients who undergo continuous salvage chemotherapy in hospitals immediately before worsening of their general condition may lose a chance to go to a hospice/home. Indeed, the discontinuation of anticancer therapy should be considered if adverse effects surpass the benefits. Therefore, we think that it is important to keep an open mind regarding such transfer and not persist with aggressive treatment if it is harmful.
On the other hand, in the present study we identified that the disadvantage of PCS in elderly patients compared with younger patients remained significant in univariate analysis. Furthermore, age was an independent prognostic indicator in multivariate analysis. According to prior studies, aging was shown to be a poor prognostic factor for patients with gynecologic malignancy. Indeed, chemotherapy-associated toxicities, including a febrile neutropenia, is more frequently observed in elderly patients than in younger patients. In general, elderly cancer patients are likely to show an age-related decline of functional reserve in multiple organs and the higher prevalence of comorbidities. It is likely that our current findings reflect these unstable physical conditions specific to elderly patients.
Limitations of our study include its retrospective nature. The current investigation may also be biased, in that patients were treated by different physicians, and the criteria for the cessation of aggressive chemotherapy and subsequent introduction to extra-hospital care were heterogeneous. In addition, unfortunately, our study lacked information on QOL. QOL assessments are imperative in assessing cancer burden, treatment, and prognosis. 13 According to prior reports, baseline QOL data have been associated with survival in gynecologic cancer.14–16 Thus we must appropriately balance QOL with improvement of survival. If we wish to resolve such bias, a randomized controlled trial offers a solution; however, it is actually very difficult to perform because of ethical aspects and diverse environments of individual patients. At least we would like to examine these factors and reconfirm our current results in a prospective study.
In conclusion, it is possible that the EOL environment is a crucial prognostic factor for survival after anticancer treatment. Our current data could be hypothesis generating for gynecologic oncologists and patients confronted with this crucial issue. To assess the further appropriateness of extra-hospital care, we would like to accumulate more cases and reconfirm the current results in the future.
Footnotes
Author Disclosure Statement
No competing financial interests exist.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.