
Abstract
Abstract
Background:
End-of-life dreams and visions (ELDVs) have been well documented throughout history and across cultures. The impact of pre-death experiences on dying individuals and their loved ones can be profoundly meaningful.
Objective:
Our aim was to quantify the frequency of dreams/visions experienced by patients nearing the end of life, examine the content and subjective significance of the dreams/visions, and explore the relationship of these factors to time/proximity to death.
Methods:
This mixed-methods study surveyed patients in a hospice inpatient unit using a semi-structured interview. Sixty-six patients admitted to a hospice inpatient unit between January 2011 and July 2012 provided informed consent and participated in the study. The semi-structured interviews contained closed and open-ended questions regarding the content, frequency, and comfort/distress of dreams/visions.
Results:
Fifty-nine participants comprised the final sample. Most participants reported experiencing at least one dream/vision. Almost half of the dreams/visions occurred while asleep, and nearly all patients indicated that they felt real. The most common dreams/visions included deceased friends/relatives and living friends/relatives. Dreams/visions featuring the deceased (friends, relatives, and animals/pets) were significantly more comforting than those of the living, living and deceased combined, and other people and experiences. As participants approached death, comforting dreams/visions of the deceased became more prevalent.
Conclusions:
ELDVs are commonly experienced phenomena during the dying process, characterized by a consistent sense of realism and marked emotional significance. These dreams/visions may be a profound source of potential meaning and comfort for the dying, and therefore warrant clinical attention and further research.
Introduction
“E
Effective palliative medicine encompasses a model of care in which patients are given support in reconciling their death and finding closure. Although there is growing recognition that ELDVs are psychologically and existentially significant, they have rarely been explained in a care-giving framework or presented as being medically relevant. ELDVs are often dismissed as drug-induced hallucinations, dementia, or delirium by medical staff with limited understanding of the dying process. 13 Yet there is a growing body of literature that describes the prevalence and therapeutic value of these experiences. It is estimated that 50% to 60% of conscious dying patients experience ELDVs. 11 It is likely this number is even higher, as research has shown that patients, families and clinicians knowingly under-report ELEs for fear of judgment, ridicule, and embarrassment. 5
The majority of published literature on ELDVs is based on surveys or interviews with families of the deceased or with clinicians who work with the dying.6,10,12,14,15 Present in these reports is the belief among palliative care workers that ELDVs are intrinsic to the dying process. ELDVs can occur in wakeful or sleep states and typically manifest with clear consciousness. A common element reported by bereaved family members and clinical staff is the personal or spiritual solace provided by the dreams/visions for patients at end of life. Clinicians have reported that whereas hallucinations frequently elicit anxiety or perplexity, ELDVs evoke peacefulness, comfort, and a sense of wonder. In addition, ELDVs help patients reconcile past life events and accept death. Barriers to expanding the medical model to capture the importance of ELDVs to the dying patient include the prevailing scientific view that ELDVs have no intrinsic value and are medically explainable. 13 A more complete understanding of ELDVs may also be limited by the current literature, which is based primarily on caregiver or family observations.
There is a scarcity of data addressing the prevalence, content, and significance of ELEs from the patient's perspective. The current study was designed to 1) document ELDV experiences using a longitudinal survey and semi-structured interview format in hospice patients nearing the end of life; 2) examine the content and subjective significance of ELDVs; and 3) relate the prevalence, content, and significance of ELEs over time until death.
Methods
Participants
Patients admitted to the Center for Hospice & Palliative Care Hospice Inpatient Unit in Cheektowaga, New York, January 2011 through July 2012 were screened for eligibility. Those who qualified were invited to participate. Inclusion criteria were: age 18 or older, capacity to provide informed consent, and Palliative Performance Scale (PPS 16 ) score ≤40. Exclusion criteria were: diagnosis of a psychotic disorder per the Diagnostic and Statistical Manual for Mental Disorders, 4th edition (DSM-IV) and a barrier of language or communication. Sixty-six patients agreed to participate in the study.
Procedures
This study was reviewed and approved by the Social and Behavioral Sciences Institutional Review Board of The University at Buffalo (SUNY). Once consent was obtained, patients were interviewed daily by a study investigator using a standard framework of questions. The questionnaire was divided into two parts: Part 1 included closed-ended questions related to the presence or absence of dreams/visions, whether these experiences occurred during sleep or wakefulness, dream/vision content and frequency, degree of realism, and comfort versus discomfort (Table 1). Patients' responses were recorded by investigators, who checked yes/no boxes regarding the presence of dreams, degree of realism of dreams, and whether there was a dream theme of going or preparing to go somewhere. For questions regarding dream content, investigators checked boxes from a list of eight items (deceased friends/relatives, living friends/relatives, other people, deceased pets/animals, living pets/animals, religious figures, past meaningful experiences, other). Patients reported dream frequency by choosing a range of once/day, 2 to 4 times/day, or >4 times/day. Comfort provided by the dream/vision was rated on a 5-point semantic differential scale with 1=Extremely Distressing and 5=Extremely Comforting. Part 2 provided open-ended questions that were used to elicit participant descriptions of the dreams/visions. Part 1 data were the focus of this paper. Investigators also recorded key clinical indicators: PPS score, oral intake, presence/absence of fever, alertness level, as well as medication changes. Any additional pertinent laboratory information, such as albumin level, was also recorded.
Participants were asked about dreams/visions daily while in the Hospice Inpatient Unit, until either death or discharge. When possible, discharged patients were also interviewed at home or at the facility to which they were discharged. Patients were approached each day until death unless they were unable to communicate, or communication proved stressful or was confounded by delirium.
Statistical analysis
The first step in the analysis was to check the database for accuracy of data entry. This was accomplished by comparing the entered values with the original paper survey forms to ensure that data were completely accurate prior to any calculations. The minimum information needed for the primary analysis was dream/vision content and dream/vision comfort rating. Of the 276 instances of a dream/vision report, the minimum data were available in 261 cases (95% complete). Descriptive statistics, graphic analyses, and inferential analyses including multilevel models were examined. Multilevel models were chosen to account for the varying patterns of reports by individual patients, including variation in number of days included, missing days due to patient condition, and the possibility of multiple event reports per day. The minimum sample size was estimated by conducting a simulation study on the primary outcome variable of reported comfort. The goal of this analysis was to estimate the number of dream/vision event observations needed to obtain a standard error of approximately 0.125, which was thought to provide a meaningful confidence interval around the sample statistic. The simulation suggested a minimum of approximately 80 observations would be sufficient. All analyses were completed with SPSS software version 21.0 (IBM Corp., Armonk, NY).
Results
Patient characteristics
A total of 66 patients were enrolled in the study. Fifty-nine were included in the analysis; six were excluded because they were still alive; one was excluded because only a single report was obtained relatively distant from death (115 days). Demographic and diagnostic data are presented in Table 2. The mean age of participants was 74.95 years (standard deviation [SD]=14.3) with a range of 34 to 99 years. Most were Caucasian (n=54, 91.5%) and two-thirds were female (n=40, 67.8%). Delirium (n=28, 47.5%) and pain (n=24, 40.7%) were the most frequent reasons for admission to the Hospice Inpatient Unit. Cancer was the primary diagnosis of 36 patients (61%).
Percentage total >100% due to high comorbidity rate.
CHF, congestive heart failure; CKD, chronic kidney disease; COPD, chronic obstructive pulmonary disease; UTI, urinary tract infection.
Frequency and prevalence of dreams
A total of 453 interviews were conducted with a mean of 7.68 interviews per person. Range of days before death for interviews was 0 to 87, with a mean of 21.58 and median of 15. In addition, there were 90 occurrences in which interviews could not be conducted because patients were nonresponsive. Of the 59 patients who were interviewed, 52 (88.1%) reported experiencing at least one dream or vision. Almost half of the dreams/visions (45.3%) occurred while asleep, 15.7% occurred while awake, and 39.1% occurred while both asleep and awake. Nearly all ELDV events (267/269, 99%) were reported by patients to seem or “feel real.” Most daily reports included a single ELDV event (179, 81.4%) with two (13.2%), three (4.1%), and four events (1.4%) on other days.
Content of dreams
Patients were asked to describe what they had dreamed about. The interviewer coded responses on a checklist with eight categories, noting all that were included. The categories included deceased friends or relatives (46%), living friends or relatives (17%), other people (10%), and deceased pets or animals, living pets or animals, religious figures, past meaningful experiences, and other content not listed (singly and in combinations, 35%). Note that the total percentage is greater than 100% because multiple responses could be recorded for each event (e.g., deceased friend/relative and living friend/relative in the same dream). In addition, 38.9% of all dreams included a theme of going or preparing to go somewhere. Table 3 includes examples of patient ELDVs for each of the eight content categories, as well as examples of the patient-reported theme of “going or preparing to go somewhere.”
Names have been changed.
DBD, days before death.
Comfort and distress associated with dreams and visions
Patients rated the degree of comfort/distress associated with their ELDVs on a 5-point scale ranging from Extremely Comforting (5) to Extremely Distressing (1). The mean comfort rating for all dreams and visions was 3.59 (SD=1.21, 95% confidence interval [CI]=3.44–3.73) with 60.3% rated as comforting or extremely comforting, 18.8% distressing or extremely distressing and 20.7% neither comforting nor distressing. To examine whether comfort was associated with the content of ELDVs, the content categories were recoded to include: 1) Deceased (deceased relatives, friends, or pets, n=136); 2) Living (living friends, relatives, or pets, n=41); 3) Both Living and Deceased (relatives, friends, and pets, n=18); and 4) Other (unfamiliar people, religious figures, past meaningful experiences, n=66). The highest average comfort rating was associated with dreams/visions about the deceased (mean=4.08, SD=1.05), followed by deceased and living (mean=3.61, SD=0.78), living (mean=3.22, SD=1.15), and finally other people and experiences (mean=2.86, SD=1.19). See Figure 1 for a graphic representation. Preliminary examination of main effects of content across all patients (not taking time into account) indicated that comfort ratings differed depending on ELDV content; F (3257)=20.54, p<0.001. Contrasts (Dunnett's T3) showed that dreams/visions about the deceased and about both the deceased and the living were more comforting than dreams about the living (p<0.001 for both contrasts) as well as other people and experiences (p<0.001 for deceased, p=0.02 for deceased and living).
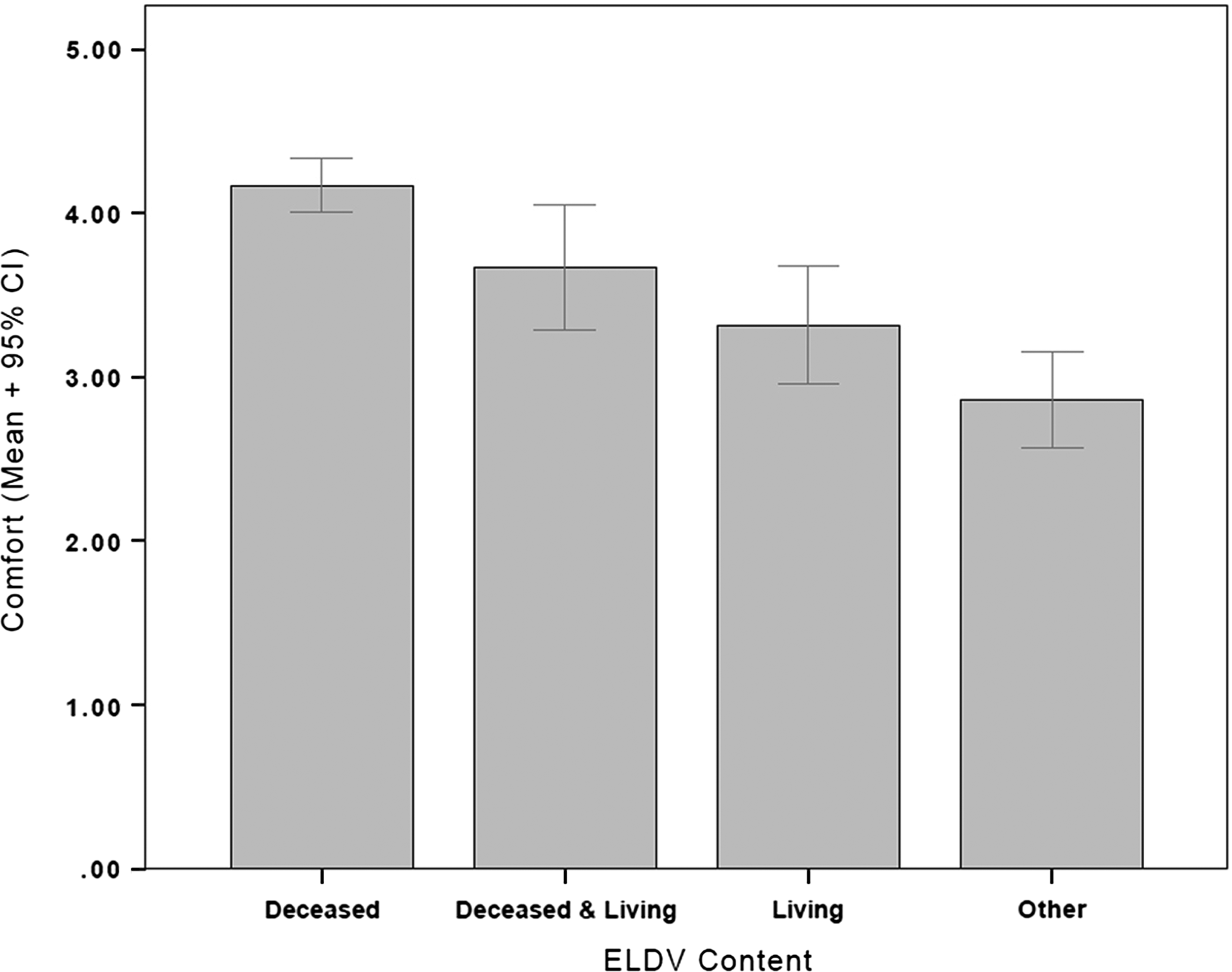
Comfort level and end-of-life dreams and visions. Error bars represent 95% confidence intervals.
Dream/vision content and comfort at daily report level
The relationship of ELDV content and time relative to death on reported comfort was examined in a series of mixed model analyses with an AR-1 covariance structure. The dependent variable in all analyses was comfort associated with the individual dream report. The first set of analyses were based on the individual daily reports with time coded as the number of days before death. These analyses tested linear and nonlinear (cubic and quadratic curves) time trends in comfort associated with ELDVs. There was no significant linear or nonlinear relationship between days before death and comfort. The next model examined the relationship of dream content (deceased, living, deceased and living, other) to comfort. The overall dream/vision content effect on comfort was significant; F(3, 246.95)=17.429, p<0.001. Significant effects were observed for seeing the deceased (b=1.16, t=6.88, p<0.001) and both the deceased and living together (b=0.66, t=2.42, p=0.02). The test of seeing only the living, and the test of seeing other content were not significant. The final model included a test of the interaction between dream/vision content and time on comfort. The interaction was not significant (F(3, 35.76)=1.61, p=.204).
Dream/vision content and comfort at weekly report level
A second set of analyses was performed to amplify effects that may not have been apparent in the daily reports. First, the daily reports were aggregated to weeks. In addition, dreams and visions were considered in categorical terms rather than on the continuous scale used to examine daily reports. This recoding examined three kinds of dreams/visions: 1) Distressing (combining the Extremely Distressing and Distressing ratings); 2) Comforting (combining the Extremely Comforting and Comforting ratings); and 3) Neither Comforting nor Distressing (as originally coded). Because this recoding produced counts of each type of dream/vision, weekly sums were examined.
The weekly sums of each type of dream/vision are plotted in Figure 2. Three content categories are plotted showing the total number of dreams/visions that were comforting, distressing, or neither. The “other” content category was not included because the mix of content was not clearly interpretable. There is one clear pattern evident in the figure: increasing numbers of comforting dreams as end of life approached. In a mixed-model analysis of comforting dreams and visions, the main effect of content was significant, F(1, 25)=16.77, p<.001) as was the effect of time (weeks before death), F(1, 25=13.84, p=.001). In addition the interaction of content and time was significant, F(3, 25=5.77, p=.004). Univariate contrasts between seeing the deceased versus the other two categories were both significant at p<.001.

Weekly sums of each type of dream/vision. There were no dreams/visions reported in the Deceased and Living category at weeks 4, 6, and 8. The line was interpolated around these time points.
Discussion
The current study was designed to quantitatively examine ELDVs from the perspective of the dying patient, and to study the temporal relationship between frequency and content of dreams/visions as patients approached death. The study demonstrates that ELDVs were common, as 87% of study patients reported dreams/visions, nearly double the rate previously reported by Kellehear and colleagues. 10 Asking patients directly about their ELDVs, a largely personal and subjective experience, may account for the higher report rates, whereas in prior studies, experiences were by a family member or a clinical caregiver.6,10,12,14,15 Regardless of whether the experience occurred during waking (19%) or sleep states (46%) or both (35%), the dreams/visions conveyed a sense of realism. Many patients reported dreams/visions of past meaningful experiences (28%) and reunions with deceased loved ones (72%) who often provided reassurance or guidance. Others reported themes of preparing to go somewhere (59%). Moreover, as in other historic and extemporaneous reports,15,17 there was a noted absence of religious content in ELDVs. ELDVs may transcend the ritualistic aspects of religion but not necessarily the existential components.
This study demonstrated a clear pattern of association of ELDVs of the deceased with greater levels of comfort with approaching death. These results were found using weeks before death, not days, as the unit of analysis. This may be due to the nature of data collection with terminally ill people, as data patterns can be difficult to identify from sparse daily reports. Nevertheless, these results are concurrent with previous research that reported patients who experienced ELDVs had peaceful and calm deaths. 12 ELDVs may therefore be prognostically significant based on changes in content and increased frequency as death nears. The descriptions of ELDVs provided by participants were typically vivid with great detail and personal meaning. Several overarching themes emerged, which will be explored and described in a separate paper.
There were several important and unforeseen observations made by the investigators while conducting the study. For example, patients' pre-death dreams were frequently so intense that the dream carried into wakefulness and the dying often experienced them as waking reality. The realism of pre-death dreams/visions is consistent with prior research suggesting that during stages of transition or crisis, dreams become more vivid, intense, and memorable. 18 In addition, despite very little spoken dialogue within the dreams/visions, the circumstances and significance of the experiences were still conveyed. The predominant quality of pre-death dreams/visions was a sense of personal meaning, which frequently carried emotional significance for the patient. This was also true of ELDV's that were not comforting.
Clinicians unfamiliar with ELDVs may discount them as hallucinations caused by medications, fever, or confusional states, 13 thus insinuating that these experiences hold little intrinsic value.8,10 It is common for dying patients to exhibit delirium when transitioning from life to death,19,20 which is marked by disorganized thinking, altered sensorium, agitation, anxiety, or fearfulness.21–23 In the current study, patients frequently experienced ELDVs as well as fluctuating states of delirium, particularly before death. ELDVs, even in the context of episodic delirium, typically contained subjective meaning, provided a source of personal solace, and were mostly characterized as comforting or extremely comforting. In contrast to delirium, ELDVs typically occur in patients who have clear consciousness, heightened acuity, and awareness of their surroundings.6,17 ELDVs are also memorable and recalled with clarity.10,11 ELDVs differ most from hallucinations or delirium by the responses they evoke, including inner peace, acceptance, and the sense of impending death.11,14,24 These distinctions are critical, as medication of ELDVs mistakenly perceived as delirium may remove the dying patient from comforting experiences inherent to the dying process. This approach may further cause isolation, suffering, and impairment in the dying person's ability to experience and communicate meaning at end of life.8,11
There are considerable data regarding the unmet psychological and spiritual needs of the dying. 25 Many physicians avoid addressing death or its spiritual implications with their patients, and this widespread inattention may exacerbate suffering and impede the dying process.26–28 The notion that nothing valuable can come from patients in the final weeks and days of life reflects a limited insight into the totality of the patient's dying experience. In the evolution from coping with illness to dying, the concept of “hope” transitions from a predication on cure to notions of personal meaning. 29 Palliative care workers have reported their belief that ELDVs signify patients' attempts to find meaning, to process or reconcile past life events and therefore come to terms with their death.2,5,6,8,13,14 Despite the value of such experiences, patients, families, and clinicians report their reluctance to openly discuss ELDVs for fear of ridicule and doubts concerning medical legitimacy.2,5,6,8,14
There were some limitations to the current study. Many patients were already experiencing ELDVs at the time of initial enrollment, making it difficult to analyze the time course of this phenomenon. Limited research staff and the dynamic nature of a hospice inpatient unit (e.g., frequent death of potential participants) also made it impossible to approach every eligible patient. A portion of the patients experienced dementia or delirium as well as ELDVs; however, only three dream events were reported by patients with dementia. Future studies should more fully control for delirium, utilize a more comprehensive questionnaire, and interview patients who are less proximate to death to capture the phenomena as they emerge or change. In addition, the interrelation of delirium and ELDVs, especially in the last few weeks of life, should be investigated further.
The results of this study suggest that a person's fear of death often diminishes as a direct result of ELDVs, and what arises is a new insight into mortality. 30 The emotional impact is so frequently positive, comforting, and paradoxically life affirming; the individual is physically dying, but their emotional and spiritual identity remains present as manifested by dreams/visions. In this way, ELDVs do not deny death, but in fact, transcend the dying experience, and present a therapeutic opportunity for clinicians to assist patients and their families in the transition from life to death, thereby providing comfort and closure.
Footnotes
Acknowledgments
James Donnelly, PhD, had full access to all of the data in the study and takes responsibility for the integrity of the data and the accuracy of the data analysis. We would like to thank the Hospice Buffalo Inpatient Unit staff for assisting with patient recruitment and John Tangeman, MD, and Rachel Depner, BA, for editorial review of the manuscript.
Author Disclosure Statement
No competing financial interests exist.