
Abstract
Abstract
Objective:
We report the indications, methods, and complications of percutaneous gastrostomy/gastrojejunostomy (G/GJ) in patients with voluminous ascites.
Methods:
Following institutional review board approval, 69 patients (14 male, 55 female, mean age 58±12 years, range 32–89 years) who underwent percutaneous G/GJ with paracentesis were identified from a prospectively acquired database. Electronic medical record data extracted included diagnosis, method of G/GJ insertion, clinical course, and complications, which were graded by The Society of Interventional Radiology (SIR) criteria. Statistics were performed using Graphpad Instat.
Results:
Sixty-six G and three GJ catheters were placed in 62 patients with malignant and 7 patients with benign disease; 47 procedures were conducted using fluoroscopy and 22 using computed tomography (CT; 10 patients had failed fluoroscopy). Sixty-six patients had 1980±1371 mL (range, 20–5000 mL) ascites drained (more in males, p=0.01) 0.8±1.6 days (range, 0–5 days) prior to placement. Forty-one patients had significantly less ascites (1895±1426 mL; range, 100–5400 mL) drained after G/GJ (p>0.0.5). Mean survival after insertion was 43±57 days (range, 1–252 days) among 38 patients for whom data were available. Fifty-six patients had a mean postprocedure hospital stay of 8.6±8.4 days (range, 0–45 days); 3 were outpatients and 10 patients died in the hospital. Successful gastropexy was confirmed on subsequent cross-sectional imaging in 22 of 25 patients. There were 25 tube maintenance issues that included catheter displacement and leakage, one patient experienced hemorrhage, and there were two deaths. All except one patient had satisfactory gastrostomy function.
Conclusion:
Effective G/GJ placement is possible in most patients with voluminous ascites provided ascites is drained and gastrocutaneous fistula formation occurs. Caution is advised; placement is generally for fragile terminal patients, and fluoroscopy or CT guidance is required.
Introduction
G
Although data are sparse, it appears that only a minority of patients presenting for G/GJ insertion have ascites. Percutaneous G/GJ requires development of a well-formed tissue tract to avoid leaks after insertion. This is usually accomplished by gastropexy, forming an adhesion of the anterior gastric wall to the anterior abdominal wall. In patients with ascites, however, development of adequate gastropexy requires special considerations, such as repeated periprocedural paracentesis. This topic has received little recent attention in the literature. 8 We hypothesized that percutaneous G/GJ insertion can be performed safely in patients with ascites, permitting effective gastric access, for what are often very ill patients. The purposes of this study were to (1) describe our methods of G tube insertion in patients with ascites; (2) report the demographics of the patient population that requires this procedure; and (3) document the complications encountered following G/GJ insertion in the presence of ascites. These were believed to be important for patient and physician education purposes.
Methods
Institutional review board approval was obtained from the regional ethical committee. A retrospective review of electronic medical and imaging data was performed to identify patients who had G/GJ insertion and paracentesis >300 mL within 5 days of insertion between June 2000 and June 2010. The following data were retrieved from medical records: patient demographics, indication for tube insertion, technique, pre- and postprocedural orders, time to patient discharge, complications, tube-related complications, and patient survival.
Oral antiplatelet agents or warfarin were stopped 5 to 7 days prior to G insertion and subcutaneous anticoagulants were held on the day of procedure. Preprocedural coagulopathy such as international normalized ratio >1.6 or platelet count <50×103 μL were corrected. The colon was identified at fluoroscopy using either barium (E-Z EM, Westbury, NY) administered orally the night before the procedure, or using an on-table enema of either positive contrast or air. Patients fasted for a minimum of 8 hours prior to gastrostomy insertion and received conscious sedation or a general anesthetic depending on clinical need. Ascitic drainage was performed with ultrasound guidance using local anesthesia and a 7 French (7F) pigtail catheter inserted over a trochar. Antibiotic prophylaxis was administered only for patients with head and neck cancer. G/GJ insertion was performed with patients placed supine under fluoroscopic or CT guidance. The stomach was inflated with air using a nasogastric tube or following 5F Kumphe catheter (Cook, Bloomingdale, IN) placement under fluoroscopic guidance through the nose into the stomach. A safe access window to the stomach was identified, and in most cases, a section of the anterior gastric wall was fixed to the anterior abdominal wall using up to four gastropexy sutures. G catheters were placed in the stomach between the gastropexy sutures over a wire placed through an 18-gauge hollow needle. A 14F Dawson-Mueller (Cook, Bloomingdale, IN) G/GJ catheter with a locking loop was typically used.
Following G/GJ catheter insertion, crushed medications were permitted through the G/GJ from the time of insertion. Tube feedings were permitted from 24 hours after insertion. G/GJ catheters were flushed with 20 mL to 30 mL of normal saline after feeds or medications were administered to maintain tubal patency. Gastropexy sutures were removed 2 weeks following gastrostomy insertion.
Values were depicted as means and standard deviations. Data were compared using Student's t test. Statistical analyses were performed using Graphpad Prism version 5.00 (Graphpad Instat Software, San Diego, CA). A P value<0.05 was considered statistically significant.
Results
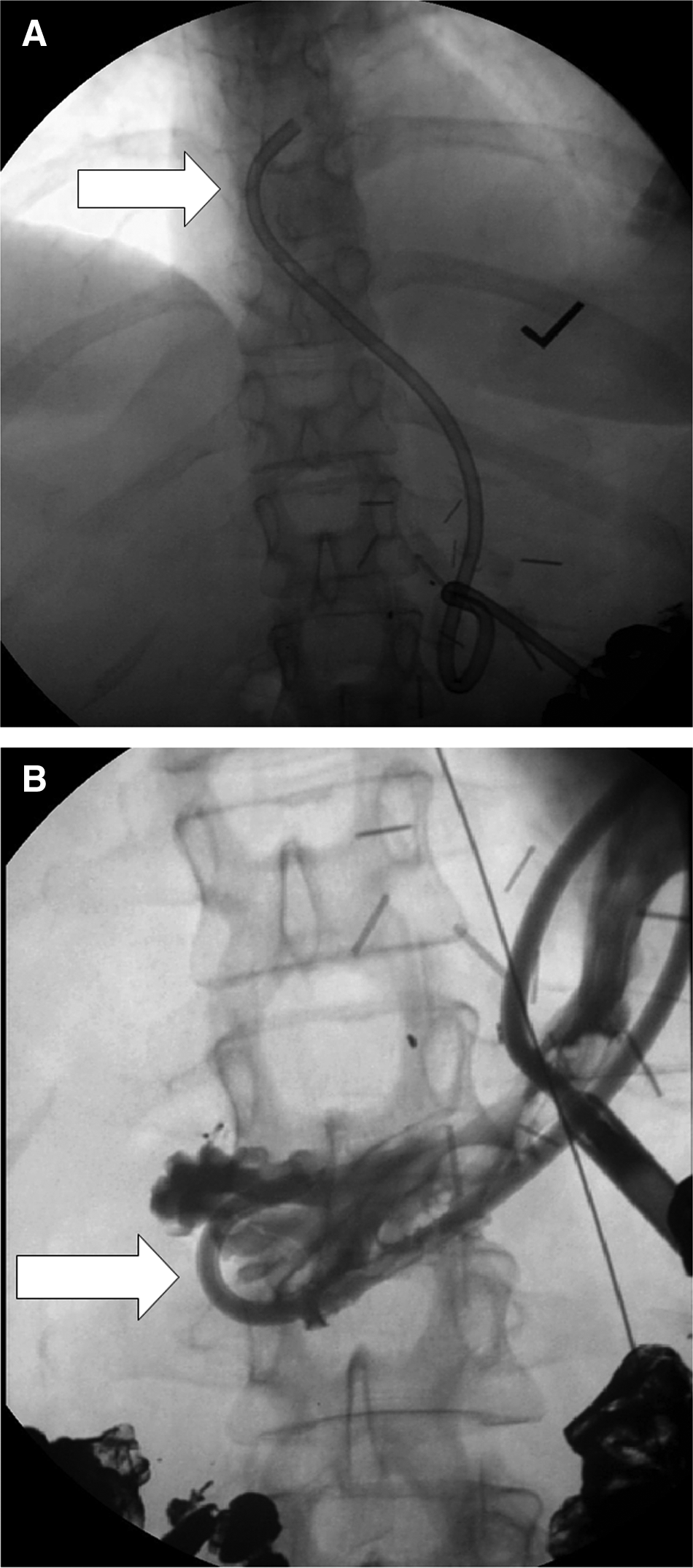
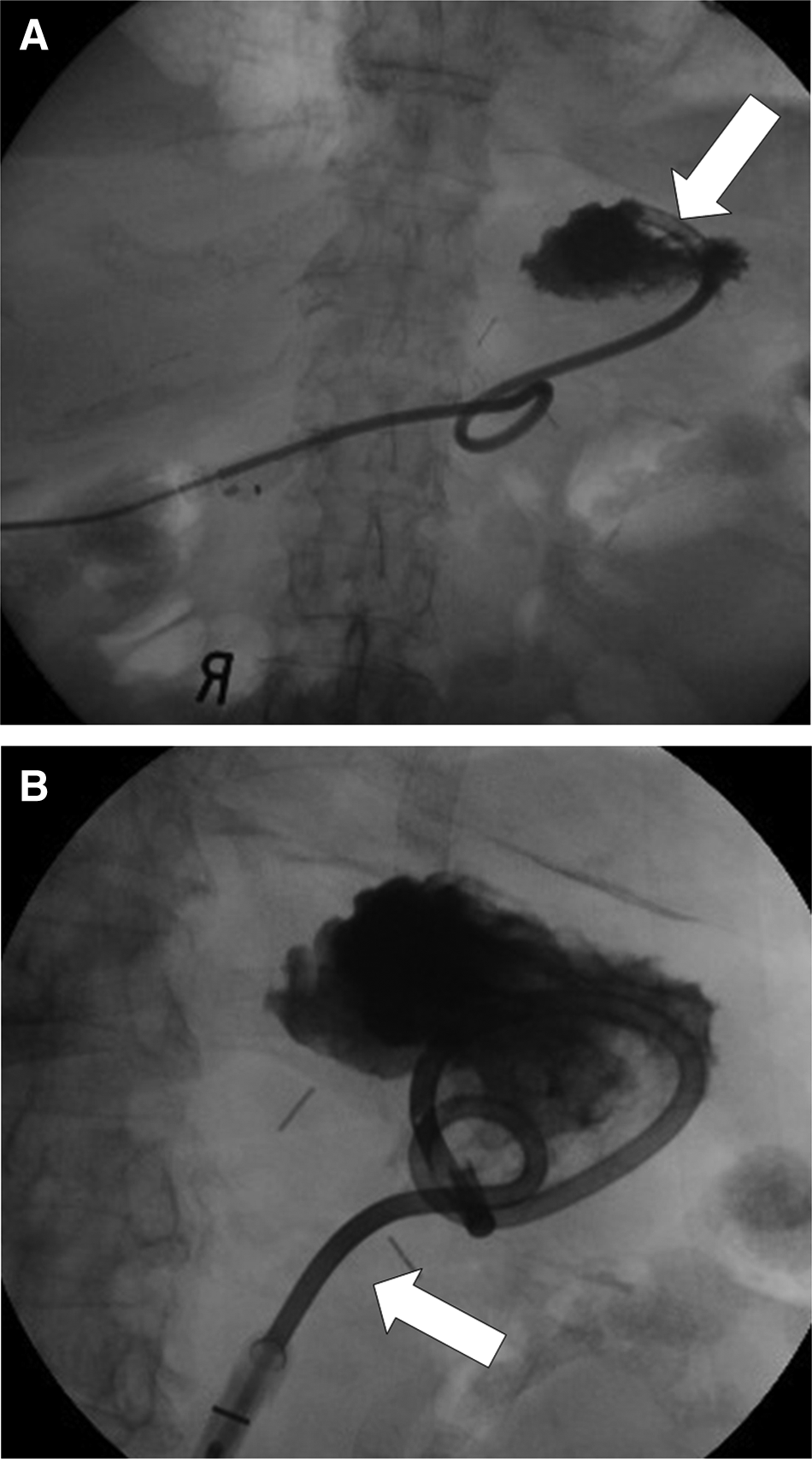
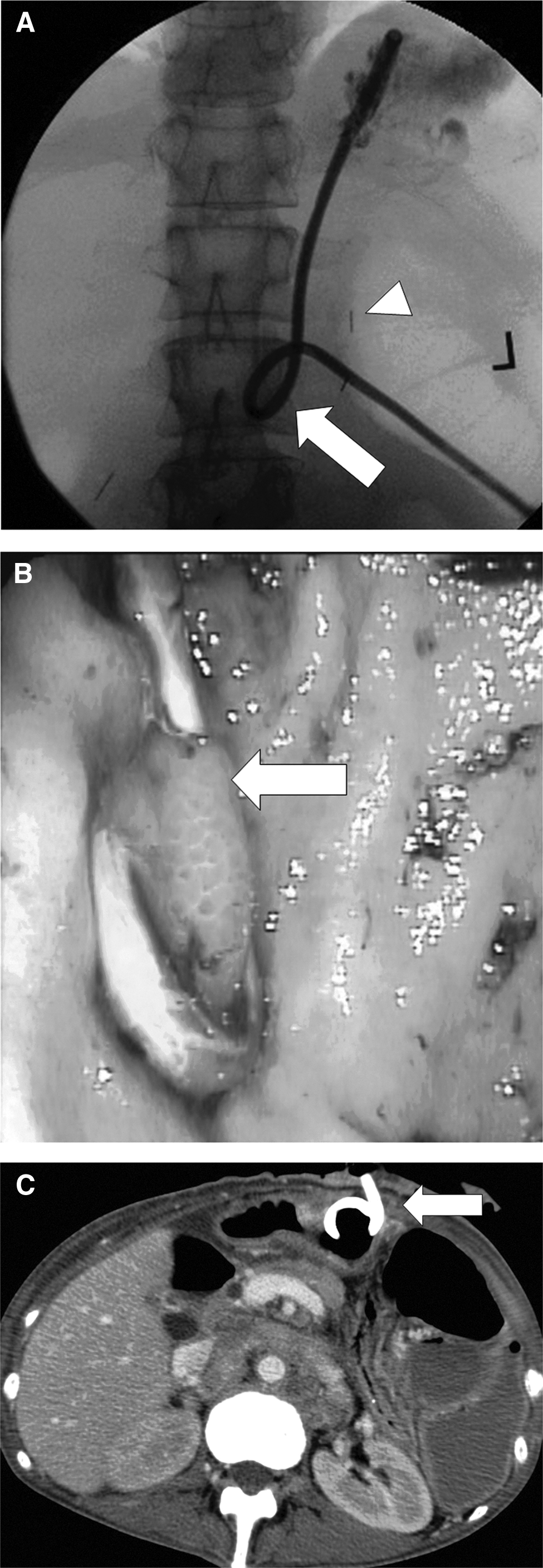
Sixty-six primary G and three primary GJ insertions were performed during the study period in 55 females and 14 males with an average age of 58 years (Table 1). Almost 90% of patients had G/GJ insertion performed in the presence of ascites due to malignant disease. Insertion was performed for gastric decompression to relieve small bowel obstruction in the majority of these cases. Ovarian cancer was the most common malignancy associated with G/GJ; it was present in 36 of 62 patients with malignancy. Remaining patients with malignancy had gastrointestinal cancer (9), other gynecologic cancers (7), pancreatic cancer (6), hematologic malignancies (2), lung cancer (1), and breast cancer (1). G/GJ insertion was performed for feeding in all cases of benign disease. Cirrhosis combined with neurological impairment was the most common reason for G/GJ insertion in the presence of ascites in patients with benign disease (5), one patient had dialysis-related peritonitis, and one had pancreatitis. Fifty-seven G/GJ tubes were placed using fluoroscopic guidance (Fig. 1) and 22 using CT guidance (Fig. 2). Ten patients failed initial attempted fluoroscopic-guided insertion, and these patients had catheters placed using CT guidance (Figs. 3 and 4).
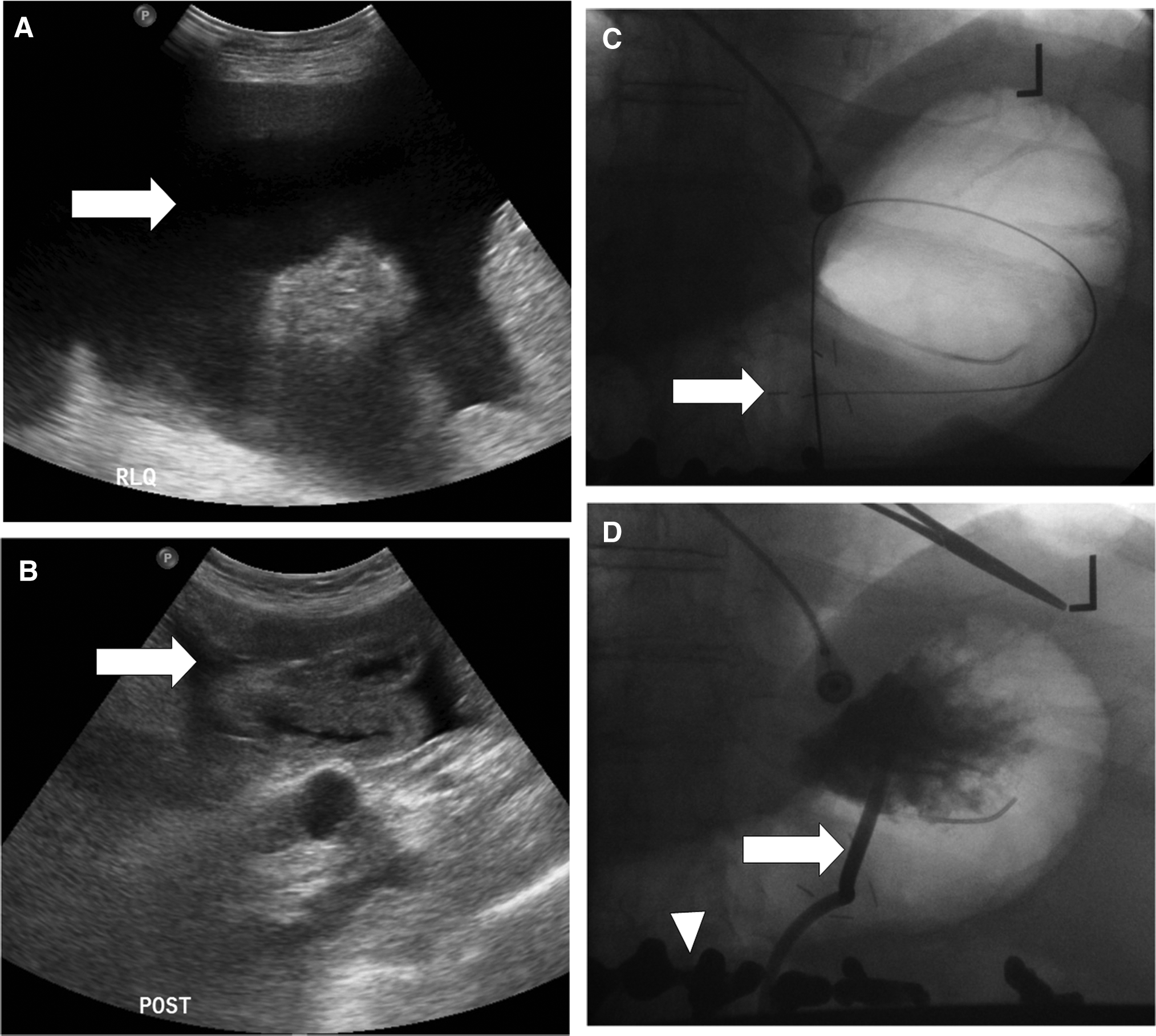
G tube placement by fluoroscopy in a 60-year-old male with laryngeal carcinoma and cirrhotic liver disease with ascites. (
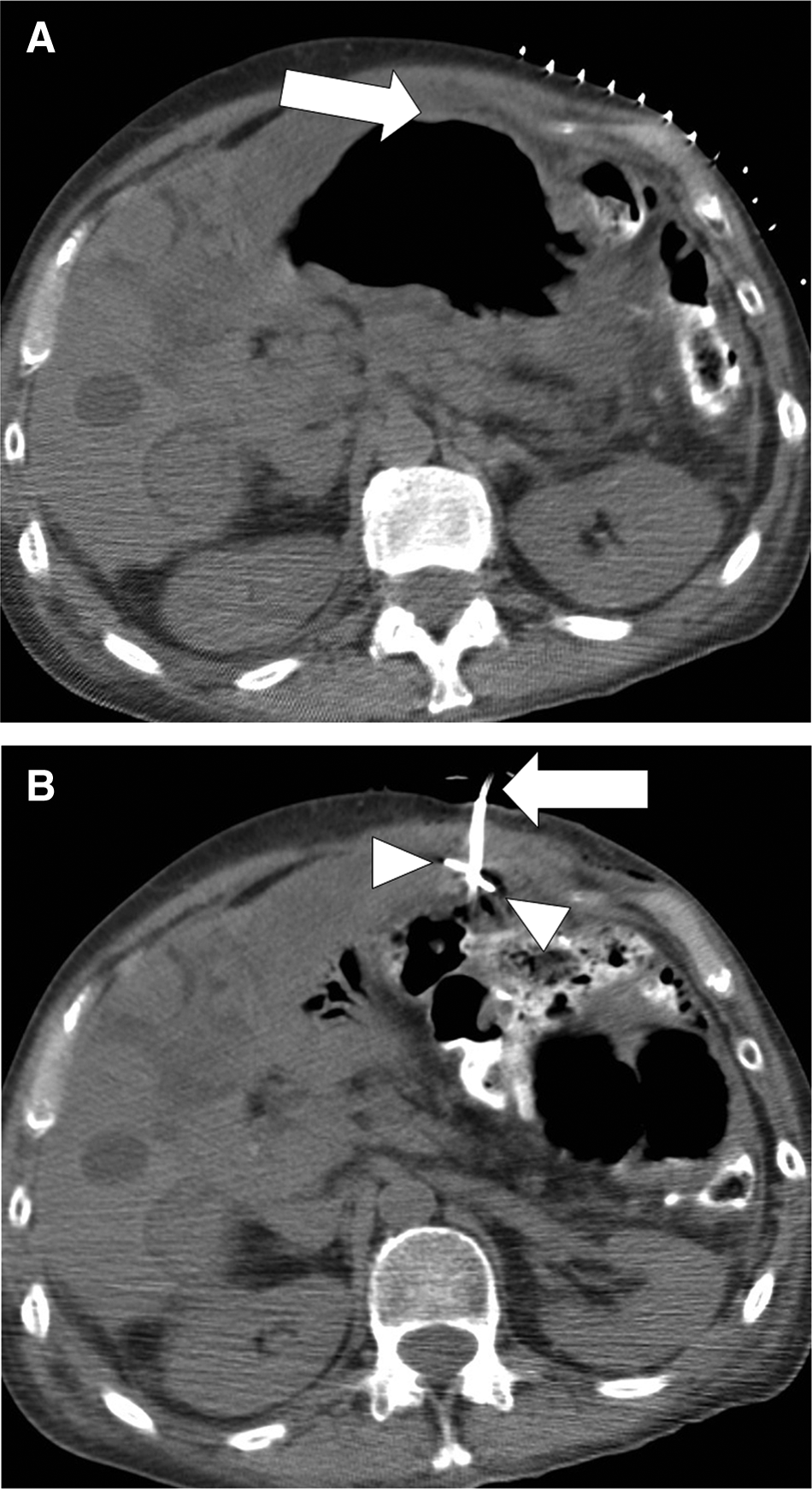
CT-guided G insertion in a 55-year-old female with ovarian carcinoma and small bowel obstruction. (
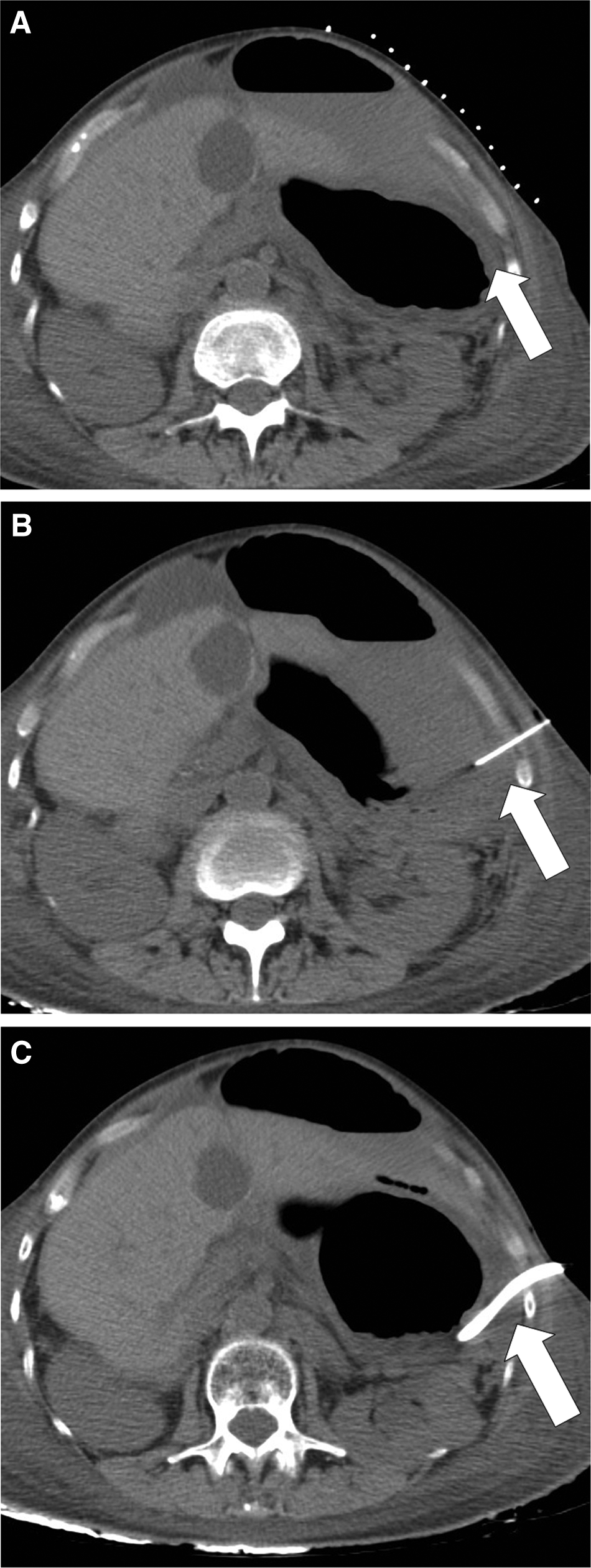
G tube insertion by CT after failed attempt by fluoroscopy due to large left lobe of liver in a 64-year-old female with endometrial carcinoma, ascites, and small bowel obstruction. (

G tube insertion by CT after failed attempt by fluoroscopy due to poor access in a 66-year-old female with peritoneal carcinomatosis, ascites, and small bowel obstruction due to ovarian carcinoma. (
Values presented are means±standard deviation where applicable.
NS, not significant; G/GJ, gastrostomy/gastrojejunostomy; CT, computed tomography.
Only three G/GJ catheters were placed on an outpatient basis (Table 2). Ten of the 66 inpatients who had insertion performed died in the hospital. The average time to discharge for the remaining 56 patients was 9 days. Data pertaining to the time of insertion to time of death available for 38 patients showed an average survival of 43 days following insertion. Patients had an average of 11 imaging examinations performed within the month prior to G/GJ insertion and six imaging studies within a month after insertion.
Values presented are means±standard deviation where applicable.
NS, not significant; G/GJ, gastrostomy/gastrojejunostomy; CT, computed tomography.
Gastropexy sutures were used in almost all cases (67/69) with an average of three sutures being used. Evidence of adequate gastropexy was sought on CT performed after G/GJ insertion (Table 1). Review of relevant studies in 25 patients performed on average 41 days after insertion confirmed satisfactory adherence of the stomach to the anterior abdominal wall in 22 cases. The stomach was remote from the abdominal wall in three patients. In two cases this was due to unfavorable anatomy: the presence of loculated ascites and omental disease between the stomach and anterior abdominal wall in one case (Fig. 5) and prior gastric bypass that precluded traction of the stomach anteriorly in the second case (Fig. 6). These catheters functioned normally, however, and no complications occurred. One patient was found to have infected ascites 8 days after G insertion. A microbiology sample had confirmed absence of infection at the time of G insertion. When the gastropexy sutures were removed 14 days after G tube placement, the stomach retracted from the anterior abdominal wall and peritoneal contamination occurred (Fig. 7). The patient subsequently succumbed to sepsis.

A 41-year-old female with ovarian carcinoma. G tube was placed under CT guidance 5 days previously after failed fluoroscopic attempt at insertion. There is displacement of the stomach from the anterior abdominal wall by ascites (arrow). The ascites was drained and tube injection showed no leakage.

A 55-year-old female with gastric cancer and status post Billroth II subtotal gastrectomy. G was placed into the afferent loop for decompression. CT 2 months after insertion shows that the stomach was not pulled up to the anterior abdominal wall (arrow). The tube functioned normally.

A 78-year-old male with diffuse, large B-cell lymphoma, portal hypertension, acute renal insufficiency, watershed cerebral infarcts, and cirrhosis of unclear etiology. (
Patients had a total of 192 ascitic drainages prior to G/GJ insertion, averaging 2.9 drainages per patient and 2649 mL per drainage (Table 3). Ascitic drainages for the purpose of G/GJ insertion were performed in 66 of 69 patients on average 0.8 days prior to G/GJ insertion, yielding an average of almost 2 L of ascites per patient. Patients who did not have drainage prior to insertion had early drainages after G/GJ insertion. Forty-one patients had 80 ascitic drainages performed on average 4.8 days after G/GJ insertion and an average volume of 1937 mL was taken (Table 4). The average volume of ascites drained on the first drainage after G/GJ insertion was 1895 mL. Twenty-eight patients did not have ascites drained after G/GJ insertion. Ten of these patients had ultrasound after insertion that showed insufficient ascites to justify drainage.
Values presented are means±standard deviation where applicable.
NS, not significant; G/GJ, gastrostomy/gastrojejunostomy.
Values presented are means±standard deviation where applicable.
NS, not significant; G/GJ, gastrostomy/gastrojejunostomy.
There were 28 major complications after G/GJ insertion. Twenty-five patients encountered tube maintenance issues (SIR grade C complications) after G/GJ insertion. These consisted of 13 tubes that fell out (Fig. 8), four tubes that required repositioning within the stomach (Fig. 9), six patients who experienced leakage, one tube that became blocked (Fig. 10), and one patient who developed skin excoriation that required direct treatment following leakage. There was one SIR grade D complication due to hematemesis from a small ischemic ulcer that occurred in a fold of mucosa that was trapped by the locking loop of a G tube and required endoscopy (Fig. 11). Two patients died as a result of SIR Grade F complications. One, described above, had failed gastropexy and peritoneal leakage (Fig. 8). The second patient had small bowel obstruction due to ovarian carcinoma and died as a result of aspiration that occurred during attempted re-insertion of a G tube that fell out the night after primary insertion.

G tube reinsertion following dislodgement in a 75-year-old female with ovarian carcinoma, ascites, and small bowel obstruction. (
G tube repositioning 12 days after insertion due to leakage in a 44-year-old woman with gastric obstruction and ascites due to pancreatic carcinoma.
G exchange in a 70-year-old female with ovarian carcinoma, 10 days after gastrostomy insertion. (
Hematemesis in a 50-year-old female following G insertion for treatment of small bowel obstruction, ascites, and peritoneal carcinomatosis due to colon carcinoma. (
Discussion
G/GJ placement in the presence of ascites is a challenging procedure. Surgical and endoscopic G placement in patients with ascites is associated with potential greater morbidity and mortality compared with radiologic insertion.9,10 Ascites potentially displaces the stomach away from the anterior abdominal wall, which renders percutaneous gastric puncture more difficult. Ascites accumulation after G placement can withdraw a G from the gastric lumen into the peritoneal cavity with detrimental consequences. 11 In addition, G placement in the presence of ascites is associated with an increased risk of infection and leakage of ascites or gastric contents, which can cause skin breakdown at the percutaneous puncture site.12,13 Therefore, ascites is currently considered a relative contraindication to G placement.
The present study is one of the largest studies conducted assessing G/GJ insertion in the presence of voluminous ascites. G/GJ insertion was performed in the same manner to that of a routine G/GJ except for the additional step of paracentesis. Paracentesis increases time and resources that are required for placement of G/GJ; however, this step is necessary to ensure adequate gastropexy, gastrocutaneous fistula formation, and prevent G leakage. Paracentesis helped ensure adequate G/GJ function in all but one patient in our series. In that case, ascitic infection developed after G placement and inadequate gastrocutaneous fistula formation occurred after 14 days. We suspect that infection was responsible for suboptimal gastropexy, which resulted in retraction of the stomach from the anterior abdominal wall when the gastropexy sutures were removed, despite drainage of considerable volumes of ascites after G placement. This finding suggests that ascitic fluid drained in the periprocedural period should be assessed for infection. Gastropexy sutures should remain in place for longer in the presence of infection because these patients are quite ill and probably require longer than normal for adequate gastropexy to occur.
Results from the present studyindicate that the majority of patients requiring G placement in the presence of voluminous ascites suffer from stage IV cancer and chronic small bowel obstruction. These patients are usually in the late stages of disease and are quite ill and fragile. Therefore, intervention should be reserved for patients who do not respond or cope with nasogastric tube placement and where surgery is not feasible for relief of obstruction. First-line management for these patients should entail wide-bore nasogastric tube placement. G placement, if required in this setting, is for palliative purposes, to drain the stomach thereby relieving bowel obstruction and facilitating nasogastric tube removal. The second patient who died following G insertion did so after an episode of on-table aspiration during attempted G re-insertion the day after primary placement. In addition to fasting for a minimum of 8 hours prior to the procedure, it may be advantageous that patients with bowel obstruction have a wide-bore nasogastric tube placed overnight prior to venting G placement to ensure that the stomach is empty in advance of supine placement and conscious sedation for G/GJ placement. Only five patients had benign disease with GJ/G placed for feeding purposes not possible for prolonged periods using a feeding tube placed via the nasal passages. Nonenteral (total parenteral nutrition [TPN]) feeding is an option for patients with bowel obstruction. TPN administration in tandem with G tube placement due to bowel obstruction (with or without ascites) from gynecologic cancer has a 5-week survival benefit. 14 GJ tubes were placed for one patient with hepatic encephalopathy, and two patients with peritoneal carcinomatosis.
There were many tube maintenance issues. These are often considered separate from complications of G/GJ insertion, but for the purposes of the present study it was deemed appropriate that these be labeled as major complications. These issues resulted in additional procedures such as catheter replacement, or repositioning, and increased the level of care that the patients required, therefore meriting consideration as major complications (SIR grade C). The incidence of major and minor complications appears to be higher compared with that of patients without ascites. For example, a review of 254 new Gs and 275 replacement procedures in patients without ascites had a major complication rate of 1.3% (no deaths) and a minor complication rate (including tube blockages) of 4.5%. 15 These differences are likely a reflection of the clinical condition of the patients requiring G/GJ placement in the presence of considerable ascites. The mean survival of 38 patients after G/GJ insertion in the present study was only 43 days. The tertiary and quaternary nature of our institution meant that many patients were discharged to another hospital or nursing or hospice facilities and although lost to follow-up, were likely to have a short survival after G/GJ placement due underlying disease. Patient discharge and patient death due to underlying malignancy probably explain the reduced number of ascitic drainages and radiologic studies observed after G/GJ insertion. Once it was established that G/GJ function was adequate and the gastropexy sutures were removed, paracentesis was only performed for symptomatic or diagnostic purposes.
The present study also highlights the need for radiologists to be prepared to use CT for G/GJ placement in patients with voluminous ascites if the majority of patients are to be treated because there was an 18% failure rate of initial attempts of fluoroscopic insertion. This was due to unfavorable anatomy at fluoroscopic insertion such as subcostal gastric position. The presence of omental, peritoneal, and hepatic metastases can also render fluoroscopic insertion unsafe. Inspection of preprocedure CT imaging helped identify 12 of 22 patients unsuitable for fluoroscopic-guided insertion with a further 10 patients deemed unsuitable on the fluoroscopy table. The vast majority of patients with voluminous ascites requiring G/GJ will have cross-sectional imaging available, and we recommend close evaluation of this imaging to plan the procedure.
There are limitations to the present study including the absence of a control group for comparison and an objective assessment of quality of life following G/GJ placement, which would help confirm justification of the procedure over simply placement of a nasogastric decompression tube. This is a potential avenue of future research on this topic particularly because survival was very short and one has to question whether patients sufficiently benefit from a procedure with a high complication rate in their last remaining days (43 days on average). The tertiary nature of our hospital and the terminal state of so many of our patients resulted in many patients being lost to follow-up. G/GJ placement in the presence of voluminous ascites was performed roughly once every 2 months during the 10-year study period. During this time period we placed approximately 1600 routine G/GJ tubes. Therefore G/GJ placement in the presence of voluminous ascites is a relatively uncommon procedure and many different operators were involved in catheter placement. Eighteen patients had neither paracentesis nor ultrasound evaluation for ascites performed in our hospital after G/GJ placement. Many of these patients either died as a result of their disease or were transferred out of the hospital. Ten patients did have early postprocedure ultrasound that confirmed that there was insufficient ascites to merit paracentesis. Where possible, ultrasound was performed to assess for ascites following G/GJ placement. Outside care facilities to which patients were transferred soon after G/GJ insertion were instructed to monitor for ascites re-accumulation and to remove gastropexy sutures after 2 weeks. Compliance with these instructions cannot be assessed. Other authors advocate tunneled peritoneal catheter placement to ensure adequate ascitic drainage and obviate the need for surveillance ultrasound. 16 We believe that this would add further to the complexity, although this may be useful for patients who are discharged home.
Conclusion
The findings of this study indicate that G/GJ placement can be performed safely in the majority of patients with voluminous ascites, but there is a high incidence of complications. Patients generally require G/GJ placement in this setting for palliative purposes; these patients are generally very ill and have terminal disease with short life expectancy. Compared with routine G/GJ placement, extra precautions are required to ensure adequate gastropexy and gastrocutaneous fistula formation. Based on the results of this study we recommend review of preprocedure cross-sectional imaging prior to G/GJ placement in the presence of voluminous ascites, gastric decompression if there is small bowel obstruction, drainage of ascites before and after catheter placement, assessment for ascitic infection at the time of insertion, and a low threshold for the use of CT guidance. Justification, effects on quality of life, and risk-benefit ratio should be assessed in future research.
Footnotes
Acknowledgments
This research paper was presented as an oral presentation at the Society of Interventional Radiology Annual Meeting in San Francisco in March 2012.
Author Disclosure Statement
No competing financial interests exist.