
Abstract
Abstract
Background:
Over the last 20 years, multiple interventions to better integrate palliative care and intensive care unit (ICU) care have been evaluated. This systematic review summarizes these studies and their outcomes.
Methods:
We searched MEDLINE, Embase, Cumulative Index to Nursing and Allied Health Literature (CINAHL), the Cochrane Library, and the Web of Science; performed a search of articles published by opinion leaders in the field; and reviewed hand-search articles as of August 13, 2012. The terms “palliative care” and “intensive care unit” were mapped to MeSH subject headings and “exploded.” We included trials of adult patients that evaluated an ICU intervention and addressed Robert Wood Johnson group-identified domains of high-quality end-of-life care in the ICU. We excluded case series, editorials, and review articles. We compared two types of interventions, integrative and consultative, focusing on the outcomes of patient and family satisfaction, mortality, and ICU and hospital length of stay (LOS), because these were most prevalent among studies.
Results:
Our search strategy yielded 3328 references, of which we included 37 publications detailing 30 unique interventions. Interventions and outcome measures were heterogeneous, and many studies were underpowered and/or subject to multiple biases. Most of the interventions resulted in a decrease in hospital and ICU LOS. Few interventions significantly affected satisfaction. With one exception, the interventions decreased or had no effect on mortality. There was no evidence of harm from any intervention.
Conclusions:
Heterogeneity of interventions made comparison of ICU-based palliative care interventions difficult. However, existing evidence suggests proactive palliative care in the ICU, using either consultative or integrative palliative care interventions, decrease hospital and ICU LOS, do not affect satisfaction, and either decrease or do not affect mortality.
Introduction
T
Patients in an ICU have a high symptom burden and frequently experience functional impairments both in the ICU and after discharge. Evidence shows that patients experience difficulty communicating, pain, dyspnea, hunger, and drowsiness while in the ICU.3–5 Following ICU discharge, these patients often have poor health-related quality of life with significant functional limitations and higher mortality.6–9 The term “post–intensive care syndrome” refers to a constellation of impairments in both ICU survivors and their family members including persistent physical, cognitive, and psychological impairments in survivors and psychological impairments in family members of ICU patients. 10 Thus, providing effective and high-quality palliative care to improve end-of-life care and to better mitigate short- and long-term physical and psychological burdens and functional impairments has the potential to benefit all ICU patients and their families.
The literature includes several consensus statements and professional society clinical guidelines recommending ways to improve the delivery of palliative care in the ICU.10–17 Included in these guidelines are recommendations for patient- and family-centered care and shared decision making. A consensus group, funded by the Robert Wood Johnson Foundation, included seven domains for equality care in the ICU 15 and these include: (1) patient- and family-centered decision making, (2) communication, (3) continuity of care, (4) emotional and practical support of patients and families, (5) symptom management and comfort care, (6) spiritual support, and (7) emotional and organizational support for ICU clinicians. Of note, all of these domains are inherent to palliative care and are likely to benefit both dying and surviving ICU patients and their families.
Interventions to improve palliative medicine in the ICU have been evaluated by two recent literature reviews. The first was a systematic review by Scheuneman and colleagues, which included a search of the literature from 1995 to 2010 using MEDLINE, PsychInfo, Cochrane, and Cumulative Index to Nursing and Allied Health Literature (CINAHL) databases. 18 However, the search included only communication-related interventions. The second review was conducted by the Improving Palliative Care in the ICU (IPAL-ICU) consensus group. 19 This review was not systematic and included only the MEDLINE database. The IPAL-ICU group suggested that the type of palliative care intervention—integrated into standard ICU care, consultative to that care, or a combination of both—might impact efficacy. 19 To capture articles published prior to 1995, to include interventions that involve palliative medicine related concepts beyond communication, to search a wider breadth of databases, and to contrast the efficacy of consultative versus integrative interventions, we conducted a systematic review of the literature to identify evidence-based interventions that improve the delivery of palliative care in the adult ICU. To more clearly interpret the data, we further defined “integrative” and “consultative” into two mutually exclusive categories and thus eliminated designation of an intervention as “both.”
Methods
The systematic review
We conducted a systematic review of the literature to identify evidence-based interventions that improve the delivery of palliative care in the adult ICU. We searched MEDLINE (1949–2011), Embase (1974–2011), CINAHL (1982–2011), the Cochrane Library (2005–2011), and the Web of Science (1956–2011) as of August 13, 2012. A detailed and systematic search strategy was used, with the terms “palliative care” and “intensive care unit” mapped to the appropriate MeSH subject headings and “exploded” (see Appendix 1 for specific search terms). We did not limit by language or publication type. As MeSH terms for palliative care are relatively immature, we also completed an ancillary search where articles published by 15 prominent researchers and thought leaders in the field of palliative care in the ICU (see Appendix 2) were identified and reviewed. In addition, we hand searched both personal files and the reference lists of review articles, consensus guidelines, professional society statements, and articles included in the final review.
Study selection
Exclusion criteria were (1) case series, (2) commentary or editorial, (3) review article, (4) lack of measurements or lack of novel data, (5) fewer than 20 patients enrolled in the study, and (6) publication only as abstract or nonpeer reviewed dissertation.
Inclusion criteria were (1) study of adults (age 18 or over), (2) study must involve evaluation of an intervention, and (3) intervention must involve both ICU patients and any of the seven domains identified by the Robert Wood Johnson consensus panel. For each eligible study, two authors (JC, DV, DG, and/or RA) used standardized abstraction sheets, and discrepancies were resolved by discussion between abstractors. Abstracted evidence was graded for the strength of the best available evidence, including the risk of bias in relevant studies, using a system based on the Grading of Recommendations, Assessment, Development, and Evaluation (GRADE) Working Group criteria adopted by the Agency for Healthcare Research and Quality (AHRQ).20,21
Categorization of study
We placed each study intervention into one of two categories, integrative or consultative. These categories were first generally described by the Improving Palliative Care in the ICU (IPAL-ICU) team. 19 Because the field lacks formal definitions of integrative and consultative palliative care, we developed the following definitions. “Consultative” described an intervention that enabled a non-ICU person—one who would not otherwise be involved in ICU patient care—to interact with the patient and/or patient family. “Integrative” described an intervention that only had ICU personnel interacting with patients and families. Interventions involving palliative care or ethics consults were classified as consultative. Interventions were classified as integrative that involved (1) a non-ICU clinician teaching ICU personnel how to better provide palliative care, (2) an order set or standardized pamphlet for families, and/or (3) standardization or triggering of ICU family meetings. For clarity, we made these definitions mutually exclusive, thus avoiding the concept of a “mixed intervention.” We carefully read each study, including the discussion section, to determine which category most closely represented the study purpose and design.
Results
Our search strategy yielded 3328 references (see Fig. 1). Deletion of duplicates and screening of titles recovered 1746 references. Further abstract screening yielded 144 articles. Full review of complete articles yielded 33 studies. Our ancillary search strategies recovered 45 articles for full review and 4 articles for final inclusion. In total, 37 publications met our inclusion and exclusion criteria (see Table 2).22–58 Some interventions were evaluated multiple times in multiple single- or multicenter studies yielding multiple publications.22,24,28,29,34,35,45,49,50,54 One study of one intervention yielded multiple publications.39–41 One publication 24 contrasted two different interventions—one consultative and the other integrative—against a single control; for this review, the two interventions were divided and analyzed separately. Thus, though there were 37 publications, there were 36 interventions to analyze.
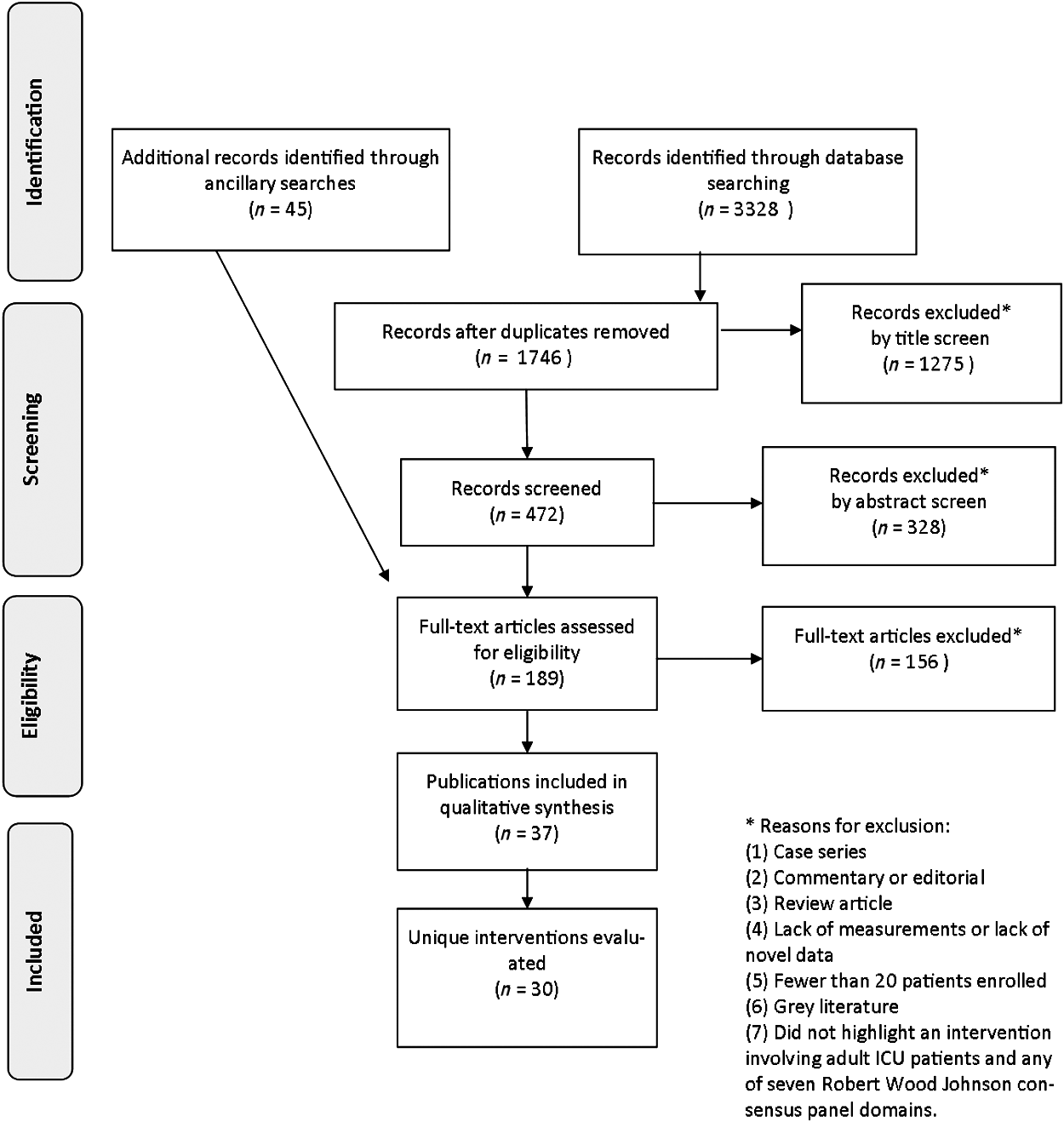
Flow diagram of search strategy.
All studies are nonrandomized, unblinded trials unless specified otherwise.
APNs, advanced practice nurses; CCFNI, Critical Care Family Needs Inventory; FS-ICU, Family Satisfaction in the ICU; GCI, global cerebral ischemia; HAD, Hospital Anxiety and Depression score; ICU, intensive care unit; IES, Impact of Event Scale; LOS, length-of-stay; LT, liver transplant recipients or candidates; MICU, medical intensive care unit; MSOF, multisystem organ failure; PC, palliative care; pts, patients; PTSD, posttraumatic stress disorder; QODD, Quality of Death and Dying score; SICU, surgical intensive care unit; TISS, therapeutic intervention scoring system; VALUE, Validate, Acknowledge, Listen, Understand, Elicit mnemonic; 55 WOLS, withdrawal of life support.
Because of wide heterogeneity in interventions evaluated and outcomes measured, we could not assess overall study quality using criteria adapted from the U.S. Preventive Services Task Force. 59
Types of studies, interventions, and ICUs
The studies were heterogeneous both in design and in types of interventions. Five studies were prospective randomized controlled trials (RCTs), one of which was blinded. There was a single matched case-control study. The remaining studies were either pre-test/posttest or longitudinal cohort studies and were unblinded.
The types of consultative interventions included ethics consultations,26,29,35 palliative care or comprehensive care consultations,22,23,36,43,46,47,51,58 trigger systems indicating a patient to be appropriate for palliative care consult,33,36,48,56 family coordinator involvement, 52 and a palliative care team member rounding with the ICU team. 55 Integrative interventions included intensive multidisciplinary communication with ICU team members,28,31,34,42,44,49 informational brochures/booklets,24,30,42 palliative care related clinician education,25,37,42,45,50,54 structured communication with either an ICU nurse or social worker,27,32 use of local champions,45,50,54 family presence on rounds, 53 individual clinician feedback,45,50,54 and standardized palliative care related order sets or symptom scoring.37,38,45,50,54 Several of the interventions were comprised of multiple components.39,54,57
Two studies were completed in France,30,42 whereas the remainder were completed in the United States. Three studies were completed in surgical ICUs,47,48,58 with the remainder in medical ICUs or mixed med-surg ICUs.
Study quality was moderate. Many studies were small (<100 participants) and conducted at a single center. Studies generally accounted well for incomplete outcome data and did not have selective outcome reporting. However, sequence generation and allocation concealment were inadequate in many studies, and relatively few studies incorporated blinding of involved personal and/or outcome assessors. Most studies did not perform prospective power analyses, and, thus were potentially underpowered to detect differences.
Outcome measures
Outcome measures were heterogeneous among study designs, with over 40 different validated and unvalidated metrics used (see Appendix 3). Many studies utilized multiple outcome measures. Outcomes were sometimes stratified between decedents and survivors. The four most frequently used outcome measures were ICU length of stay (LOS), hospital LOS, family satisfaction, and mortality. Because of the wide variation in study outcome measures, study comparison was challenging. However, using the four most frequent measures allowed limited but meaningful comparison among the studies.
Study findings
The study findings were also heterogeneous. Most resulted in decreased ICU and hospital LOS without affecting mortality (see Table 2). Family satisfaction was not affected in most of the studies. Of the 21 interventions that measured ICU LOS, 13 found a decrease in ICU LOS associated with the palliative care related intervention. Of 14 interventions that measured hospital LOS, 8 found a decrease in hospital LOS associated with the intervention. Some interventions29,35 decreased only decedent LOS, while others28,34 decreased LOS for all ICU patients, including those who survived.
Of the 16 interventions that measured mortality, only one (n=99) 26 found an increase in mortality. One larger study (n=2495) 34 found a decrease in mortality, and the remaining studies (n=3375)22,23,28–31,35,36,42,43,47,49,51,58 showed no significant change in mortality.
Of the 14 interventions that measured family satisfaction,24,27,29,30,32,39–41,44–46,50,52–54 only 1 46 found a significant increase in overall satisfaction. Other significant findings included decreases in: nonconsensus between families and providers or between provider groups,28,47 family member PTSD and anxiety, 42 use of ventilators,29,35,51 and use of artificial nutrition and hydration. 29 Other significant findings included an increase in the number of family meetings42,49 and the percentage of patient status changes to DNR. 36
Integrative versus consultative
Of the 18 studies that were classified as consultative 12 measured ICU LOS (see Table 3). Of those 12, 9 equating to 79% of subjects, found a decrease in ICU LOS in at least one measured subgroup. Of the 19 integrative studies, 9 measured ICU LOS (see Table 4). Four of those 9, equating to 52% of subjects, found a decrease in ICU LOS. Similarly, of the 18 consultative studies, 9 measured hospital LOS. Six of those 9, equating to 79% of subjects, found a decrease in hospital LOS in at least one measured subgroup. Of the 18 integrative interventions, 5 measured hospital LOS; 2 of those studies, equating to 25% of subjects, found a decrease in hospital LOS.
Study had two separately analyzed components—one integrative, one consultative; study results divided for this review.
Discussion
Overall results suggest that despite heterogeneity, ICU-based, palliative care interventions decreased hospital and ICU LOS while changing neither hospital mortality nor family satisfaction. Interventions also improved the quality, quantity, and content of communication and decreased symptoms of distress and anxiety in family members. Interventions also decreased the use of procedures and decreased the time between admission and comfort measures only, withdrawal of life-sustaining treatments, and do-not-resuscitate orders. We found no evidence of harm in any study.
The consultative group had a higher percentage of participants with a decrease in hospital and ICU LOS than the integrative group. However, because of the heterogeneity in design and outcome measures, it is impossible to infer that one is superior to the other. Several of the studies did not measure LOS, and it is possible that these interventions would have had an impact on LOS, if it had been measured. Several of the integrative interventions did show a decrease in LOS25,28,34 as well as improvement in other equally important outcomes (such as family anxiety and distress).
Two of the integrative studies30,42 were completed in France, where, at the time of the intervention, ICU attending physicians did not routinely involve the family members in the decision to withdraw life support.42,60 Thus, these interventions were targeted at family member anxiety and distress rather than LOS. Only one of the French studies measured ICU LOS and found no change. 42 Both French trials were well conducted, high-quality studies with significant findings, published in high-impact journals. Cultural differences present a challenge to the generalizability of these findings to the United States, where decision making is shared and interventions are expected to also have an effect on health care utilization and cost. However, the impact of these interventions on the well-being of family members is important.
Neither the integrative nor the consultative interventions appeared to impact family member satisfaction. The reasons for this apparent lack of effect are multifaceted. Firstly, baseline family satisfaction is relatively high (approximately 70%); only large studies would be powered to detect statistically significant changes, particularly if effect size is small. This ceiling effect could be a result of metrics that are not sensitive or calibrated to actual family satisfaction. Further, regardless of whether a patient actually receives “good” care (however that might be defined), patients and families might be invested in believing that they receive “good” care and reticent to criticize caregivers—if stranded in an allegorical lifeboat with few to no alternative options, patients and families may be understandably slow to question whether the boat is sound or the boat's crew seaworthy. In addition, because patients and families might only experience one ICU, they may be ill equipped to give informed appraisals that inherently involve comparison or evaluation of ICU quality. It is also possible that patients and families are educated consumers aware of all potential possibilities for ICU care and are still highly satisfied with the delivered care. Ultimately, satisfaction is a multifaceted, complex phenomenon that is difficult to meaningfully measure and interpret
One might expect that proactive palliative care in the ICU would increase mortality by potentially causing patients and/or family members to value “comfort over cure” and choose noncurative, life-limiting care options. In our experience, this preconception tends to delay consulting a palliative care professional, because the ICU provider notes he or she is not yet ready to “give up” or to “send that message” to the patient and family. However, the evidence does not support this preconception. The reviewed studies found that palliative care in the ICU was not associated with an increased likelihood of patient death or with any other harm. Rather, the literature demonstrates that better palliative care in the ICU benefits patients, families, and health care systems without increasing mortality.
Although consultative interventions appeared to be more efficacious in reducing ICU and hospital LOS, each approach has benefits and drawbacks. Integrative interventions inherently involve extra duties allocated to ICU teams, who already balance multiple tasks imperative to safe and effective ICU care. Adding more, often time-intensive, tasks (such as communication exploring patient and family care goals) may be burdensome. In contrast, a consultative approach allows one provider or provider group to deliver standardized and/or evidence-based palliative care. Consultative approaches might be especially effective in ICUs with open or semi-open administration models, where integrative approaches must involve training of multiple providers of disparate disciplines and specialties. The drawback to the consultative approach is that it requires hiring, training, and paying new personnel for whom reimbursement may not cover expenses. 61 Thus, as ICU leaders and policy makers plan potential future interventions, the benefits and drawbacks of both approaches should be considered.
Limitations
Threats to validity and limitations of this systematic review include that the title, abstract, and study screening were completed by a single author (RA), and thus we cannot assess kappa or inter-reviewer reliability of study selection. In addition, the rationale for exclusion of each article was not specifically tracked and counted. As mentioned, there are also potential gaps in the search strategy because of immature MeSH terms, although the authors attempted to counteract this through the use of the ancillary search strategy. Moreover, lacking prior precedent, the definitions of consultative and integrative were formalized by study authors; their generalizability and utility are untested and unclear. Finally, the heterogeneity of studies complicates our ability to summarize results and to use outside metrics to compare study quality.
Directions for future research
These findings highlight multiple avenues for future research. First, the field could benefit from a definitive, well-powered, well-designed, multicenter controlled trial evaluating proactive palliative care in the ICU as compared to usual ICU care. By definition, such a trial would utilize meaningful, multifaceted outcomes; stakeholders are not likely to value an intervention that decreased ICU LOS while concurrently increasing patient suffering or family anxiety levels. As exemplified by the diversity and heterogeneity of the outcomes in previously published studies (see Appendix 3), such meaningful, multifaceted palliative care related outcomes do not currently exist, and the development and validation of such metrics is a critical area for future research. 62 Future ICU-based palliative care studies should also incorporate patient-centered outcomes, such as health-related quality of life and symptom scores, to ensure that interventions are reducing suffering (the core mission of palliative care) and meaningfully impacting patient and family experience. Finally, good palliative care requires that the care provided enables a patient and their family to set meaningful, and obtainable, health care related goals. Future studies could benefit through better capture of patient and family care goals and whether or not the palliative care related intervention better ensures achievement of those goals.
Summary
This review identified 37 highly heterogeneous studies of ICU-based palliative care and palliative care related interventions. Studies were often small, single-center, of “before-and-after” study design, and underpowered. However, this data supports that palliative care in the ICU is likely to decrease ICU and/or hospital LOS, increase the quality and/or quantity of communication and consensus around patient care, and not affect mortality. No studies showed harm to patients, families, or ICU providers. In general, evidence supports that proactive ICU-based palliative care does not hurt and is more likely to help patients and families. Moreover, though many integrative interventions showed statistically significant impacts in a variety of meaningful outcomes (such as family anxiety and depression), a higher proportion of consultative interventions evidenced statistical benefit concerning ICU and hospital LOS.
Footnotes
Acknowledgments
RA was salary supported throughout completion of this study by a T32 National Institutes of Health grant, a Foundation for Education and Research Mentored Research Training Grant, and a Johns Hopkins School of Medicine Clinician Scientist award.
Author Disclosure Statement
No competing financial interests exist.
Appendix 1
Search strategies for:
(“palliative care”[MeSH Terms] OR (“palliative”[All Fields] AND “care”[All Fields]) OR “palliative care”[All Fields] OR palliation[All Fields] OR (“palliative care”[MeSH Terms] OR (“palliative”[All Fields] AND “care”[All Fields]) OR “palliative care”[All Fields] OR (“palliative”[All Fields] AND “medicine”[All Fields]) OR “palliative medicine”[All Fields])) AND ((“intensive care units”[MeSH Terms] OR (“intensive”[All Fields] AND “care”[All Fields] AND “units”[All Fields]) OR “intensive care units”[All Fields] OR (“intensive”[All Fields] AND “care”[All Fields] AND “unit”[All Fields]) OR “intensive care unit”[All Fields]) OR “respiratory care unit”[All Fields] OR “respiratory care units”[All Fields] OR “coronary care units”[All Fields] OR “coronary care unit”[All Fields] OR “burn unit”[All Fields] OR “burn units”[All Fields] OR “recovery room”[All Fields] OR “recovery rooms”[All Fields])
‘intensive care unit’/exp OR ‘intensive care unit’ OR ‘intensive care units’/exp OR ‘intensive care units’ OR ‘close attention unit’/exp OR ‘close attention unit’ OR ‘intensive care department’/exp OR ‘intensive care department’ OR ‘close attention units’ OR ‘intensive care departments’ OR ‘respiratory care unit’/exp OR ‘respiratory care unit’ OR ‘respiratory care units’/exp OR ‘respiratory care units’ OR ‘special care unit’/exp OR ‘special care unit’ OR ‘special care units’ AND ‘palliative therapy’/exp OR ‘palliative therapy’ OR ‘palliative care’/exp OR ‘palliative care’ OR ‘palliative medicine’/exp OR ‘palliative medicine’ OR ‘palliation’/exp OR ‘palliation’ OR ‘palliative treatment’/exp OR ‘palliative treatment’ OR ‘palliative surgery’/exp OR ‘palliative surgery’ OR ‘symptomatic treatment’/exp OR ‘symptomatic treatment’
((MH “Palliative Care”) OR “palliative care” OR “palliation” OR “palliative medicine” OR “palliative nursing” OR “palliative therapy” OR “palliative treatment”) AND (((MH “Intensive Care Units”) or (MH “Coronary Care Units”) or (MH “Oncology Care Units”) or (MH “Post Anesthesia Care Units”)) or “intensive care unit” or “intensive care units” OR “coronary care units” OR “coronary care unit” OR “oncology care units” OR “oncology care unit” OR “post anesthesia care unit” OR “post anesthesia care units”)
((palliation) or (palliative therapy) or (palliative care) or (palliative medicine) or (palliative treatment) or (palliative surgery)) AND ((intensive care unit) or (intensive care units) or (close attention unit) or (close attention units) or (intensive care department) or (intensive care departments) or (respiratory care unit) or (respiratory care units) or (special care unit) or (special care units))
(Topic=(palliation) OR Topic=(palliative care) OR Topic=(palliative medicine) OR Topic=(palliative therapy) OR Topic=(palliative surgery) OR Topic=(palliative treatment) ) AND (Topic=(intensive care unit) OR Topic=(close attention unit) OR Topic=(intensive care department) OR Topic=(respiratory care unit) OR Topic=(special care unit) )
Appendix 2
List of researchers and thought leaders whose publications were reviewed via Web of Science:
Azoulay, Elie Curtis, J Randall Engelberg, Ruth A Levy, Mitchell Mularski, Robert Nelson, Judith Prendergast, Thomas J Puntillo, Kathleen Rubenfeld, Gordon D Sprung, Charles Truog, Robert D Wall, Richard Weissman, David White, Douglas
| System-related | Content-related |
|---|---|
| In-hospital mortality | ICU length of stay |
| Frequency of CPR at time of patient death | Hospital length-of-stay |
| Frequency of ethics-related discussions | Cost (fixed and variable) |
| Tracheostomy rates | Content of communication |
| Involvement of doctors in WOLS discussions | |
| % of patients with DNR orders | Participation of social workers |
| % of patients with WOLS orders | Participation of chaplains |
| % of patients receiving aggressive treatments | Participation of care coordinators |
| Time between WOLS and patient death | |
| Time between admission and DNR orders | |
| Time between admission and CMO orders | |
| Days receiving artificial ventilation | |
| Therapeutic Intervention Scoring | |
| System score | |
| Days receiving dialysis | |
| Time that family speak during a meeting | |
| # of laboratory draws | |
| Benzodiazepine administration | |
| Narcotic administration | |
| Discussions of goals of care by doctor on rounds |
| Clinician-related | Family-related |
|---|---|
| Health-care provider satisfaction | Quality of communication |
| Social worker satisfaction concerning family needs | Critical Care Family Satisfaction Survey |
| Nurse QODD score | Family satisfaction – non-validated metrics |
| Number of calls to family at home | |
| Consensus between family and clinician team | |
| Critical Care Family Needs Index score | |
| Family QODD score | |
| Family Satisfaction with Care | |
| Questionnaire | |
| Family Hospital Anxiety and Distress | |
| Scale score | |
| Family Impact of Even score | |
| Family Satisfaction in the ICU score | |
| Family feelings concerning being accepted by staff | |
| Social worker reported family activities | |
| Family satisfaction with social work | |
| Family satisfaction with decision making | |
| Critical Care Family Satisfaction | |
| Survey | |
| Family satisfaction regarding discussions of diagnosis, prognosis, and treatments |