
Abstract
Abstract
Background:
Major depressive disorder (MDD) is a common and debilitating illness in patients with cancer. However, the optimal treatment of depression in these patients remains uncertain, with limited evidence to support the use of pharmacologic therapy. We conducted a pilot study to evaluate the feasibility of an antidepressant clinical trial in the oncology population and the process of symptom-oriented selection of antidepressants (citalopram or mirtazapine) in patients with cancer and MDD.
Methods:
This was a single center, two-arm, nonrandomized, open-label, nine-week pilot study of mirtazapine or citalopram in cancer patients with MDD. The primary endpoint was the feasibility to recruit and to retain patients. Secondary outcomes included changes in Patient Health Questionnaire-9 (PHQ-9) (depression), Functional Assessment of Cancer Therapy – General (FACT-G) (quality of life), Functional Assessment of Chronic Illness Therapy – Fatigue (FACIT-Fatigue) (fatigue), and Pittsburgh Sleep Quality Index (PSQI) (sleep). We conducted descriptive statistics and responder analyses.
Results:
Of 21 patients, 18 (86%) successfully completed the study. An average of 2.8 subjects were enrolled per month. Mean scores on the PHQ-9 improved overall by 6.4 points (95% confidence interval [CI] 3.6–9.2). Additionally, mean FACT-G, FACIT-Fatigue, and PSQI scores improved in both study arms.
Conclusion:
Conducting antidepressant clinical trials is challenging in the oncology population. We approached but did not meet our feasibility goals. Depression and quality of life (QOL) scores improved with both mirtazapine and citalopram, but evidence-based pharmacologic treatments for depression in cancer patients are needed.
Introduction
D
The optimal therapy for depression in cancer patients remains uncertain, with no uniformly accepted standard of care and limited evidence to support the use of pharmacologic therapy. Few randomized controlled trials have been performed in this population, and their results have been mixed.11–17 Extrapolating from studies in medically healthy patients with depression may not be applicable for patients with cancer, as multiple factors complicate the treatment of depression in this group. For example, simultaneous treatment of the underlying malignancy introduces adverse effects from surgery, chemotherapy, or radiation, as well as an increased likelihood of drug-drug interactions. 18 Many patients also suffer from comorbid conditions such as cancer pain that contribute to the depression and require simultaneous therapy. 12
In the setting of such complexity, a more nuanced treatment approach is necessary. Increasingly, providers are utilizing a clinical strategy of selecting an antidepressant with a side effect profile that is matched to the patient's dominant cancer-related symptoms.19–21 For example, patients with depression and insomnia are often prescribed antidepressants with sedative properties. By assigning patients in this way, providers expect to see improved adherence and more favorable responses in depression ratings and QOL scores than would be found with a one-drug-fits-all approach. In this pilot study, our novel design evaluated the feasibility of a clinical trial utilizing this common prescribing practice.
Methods
Eligibility criteria
The study was reviewed and approved by the Biomedical Institutional Review Board at the University of North Carolina (UNC). Eligible patients were 18 years of age or older, had a confirmed diagnosis of cancer, an estimated life expectancy of at least six months, and a diagnosis of MDD made by a qualified psychiatrist. Patients completed the Patient Health Questionnaire-9 (PHQ-9), a nine-item instrument that has been validated in the outpatient oncology setting, to assess depression severity.22–25 Patients were only considered eligible if they obtained a score of 10 or greater, which corresponds to moderate to severe depression. 22
Patients were excluded if they were unable to complete the self-report instruments due to illiteracy, neurologic illness, visual problems, or inability to speak or read English. Patients were excluded based on psychotic or manic behaviors, active suicidal ideation or plan, current illicit substance abuse, or antidepressant or antipsychotic treatment within the prior three months. Patients were also excluded if they had severe renal or hepatic impairment.
In August of 2011, the FDA released a postmarketing alert for citalopram describing concern regarding risk of QT prolongation. Based on this alert, the eligibility criteria for this study were modified to exclude patients with a history of congenital long QT syndrome, clinically significant congestive heart failure, or bradycardia. Patients assigned to the citalopram stratum required a baseline electrocardiogram (ECG) and correction of any underlying hypomagnesemia or hypokalemia. They were excluded if receiving treatment with a concomitant medication known to have a strong association with QT prolongation or if they had a prolonged QTc interval on ECG.
Interventions
Patients referred to a psychiatrist in the UNC Comprehensive Cancer Support Program for mood or anxiety disorder were screened for the study with the PHQ-9. The psychiatrist confirmed the diagnosis of MDD, assessed eligibility, obtained informed consent, and then assigned the patient to one of two treatment strata, matching the patient's symptoms with the side effect profile of the antidepressant. Patients with insomnia, weight loss, or anxiety were assigned to the mirtazapine stratum, while patients with hypersomnolence, weight gain, or fatigue were assigned to the citalopram stratum. In cases where multiple symptoms were present, the assignment was based on the symptom that the patient deemed most troublesome. In the initial study design, patients were to be randomized within each stratum to active medication versus placebo. However, as described in the discussion section, no participants were accrued with this placebo-controlled design, and the study was modified to remove the placebo randomization.
Medication was provided through the UNC Investigational Drug Pharmacy at no cost to the patients. Patients in the mirtazapine stratum received an initial dose of 7.5mg PO nightly, with dose escalations to 15mg and 30mg. Patients in the citalopram stratum received an initial dose of 10mg PO daily, with dose escalations to 20mg and 40mg. These starting doses were chosen based on clinical experience suggesting that patients with cancer often have difficulty tolerating the higher starting doses recommended in the package inserts.20,26,27 Dosage escalations were considered at two to three week intervals in patients who had not yet achieved a complete response but were tolerating the medication. In accordance with the FDA's postmarketing alert, the study was modified such that the dose of citalopram was capped at 20mg PO daily for patients with hepatic impairment, who were over the age of 60, or who were taking concomitant cimetidine. After enrollment, patients were followed for nine weeks, with evaluations and supportive psychological counseling at weeks one, two, three, four, six, and nine.
Assessments
Assessments were conducted in person or by phone. Depressive symptoms were assessed at each visit with the PHQ-9; the Eastern Cooperative Group (ECOG) performance status was determined at each visit, and weight was measured at each in-person visit. Additional QOL, fatigue, and sleep measures were assessed at the baseline visit, and at weeks three, six, and nine. Overall QOL was assessed with the Functional Assessment of Cancer Therapy – General (FACT-G), a 27-item validated patient administered instrument. 28 Fatigue was assessed with the Functional Assessment of Chronic Illness Therapy – Fatigue (FACIT-Fatigue), a 13-item validated patient administered instrument. 29 Sleep was assessed with the well-validated Pittsburgh Sleep Quality Index (PSQI).30–32 Patients were permitted to complete measurements one week before or after the specified intervals in order to accommodate their complex cancer treatment schedules.
Statistical considerations
Statistical analysis included ascertaining the rate of enrollment and the number of withdrawals to see if the primary goals were met. Due to the change in design and the small sample size, the analysis for the individual study instruments involved primarily descriptive statistics. This included means of several demographic descriptors, standard deviations, mean change in instrument scores for each group over time, confidence intervals, and comparisons of the changes between groups. The depression response rate was also evaluated, defined as a 50% or greater reduction in the PHQ-9 score. 33 The results in this pilot study should be regarded as hypothesis generating and not confirmatory.
Results
Patient characteristics
During the initial enrollment period between January 2011 and June 2011, all eligible patients declined participation in the study in its original design as a randomized placebo controlled trial. Between August 2011 and March 2012, following modification of the trial design to omit the placebo arms, 21 patients were enrolled (see Fig. 1). Patients were predominately female (66.7%) and Caucasian (90.5%), with a level of education beyond high school (81.0%). Most patients had an ECOG performance status of 0 or 1 (95.2%) and were actively receiving chemotherapy at the time of enrollment (66.7%). Fourteen different malignancies were represented. The mirtazapine group differed from the citalopram group in that patients tended to have worse performance status at baseline, were more likely to be on active treatment, and were more likely to have metastatic disease. The final mean dose of citalopram was 27.0mg±11.6mg, and the final mean dose of mirtazapine was 15.7mg±9.8mg. Patients' baseline characteristics are listed in Table 1.
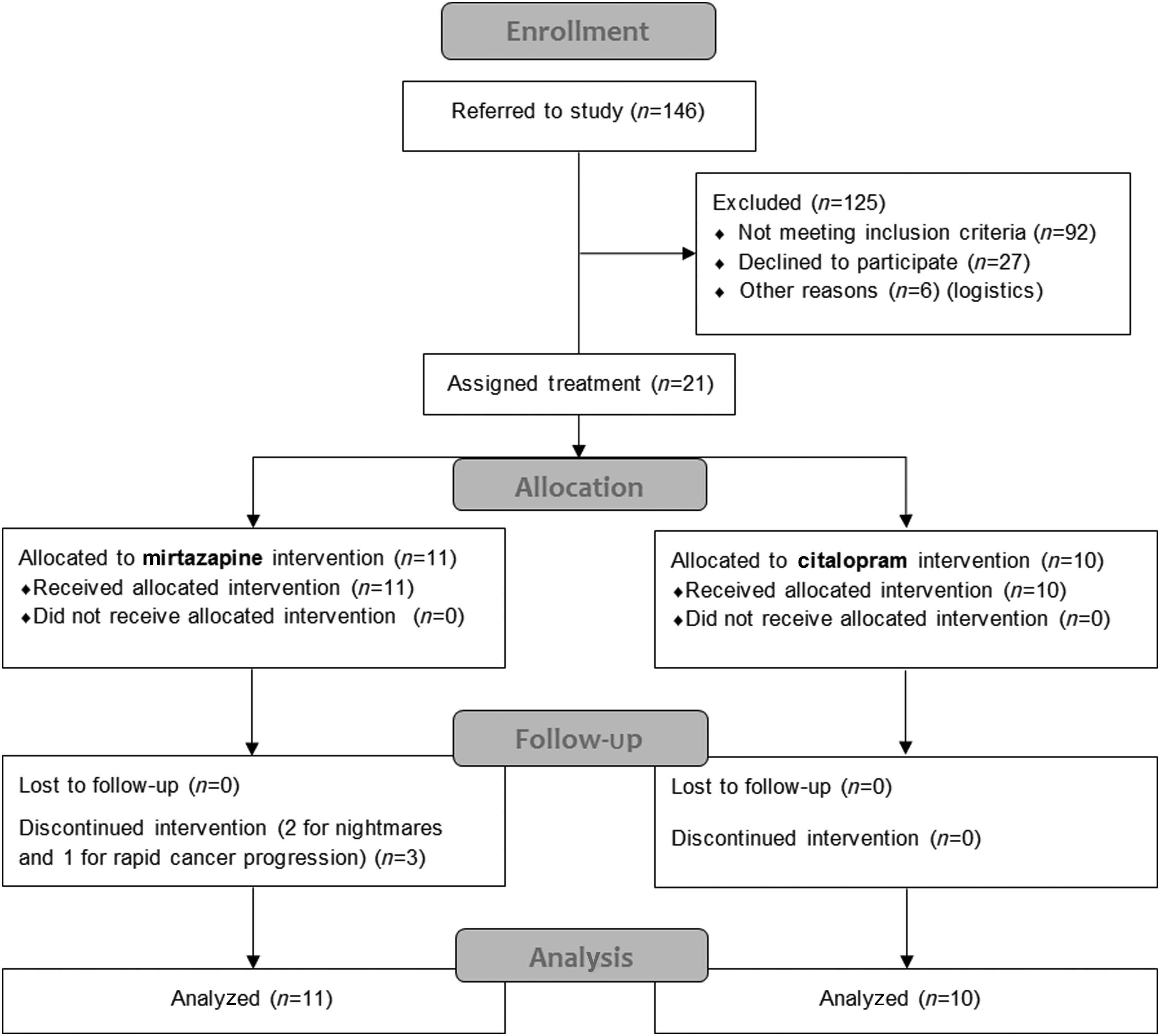
Consolidated Standards of Reporting Trials (CONSORT) flow diagram.
0=Fully active; 1=Restricted, physically strenuous but ambulatory and able to carry out work; 2=Ambulatory and capable of self care but unable to carry out any work activities.
ECOG PS, Eastern Cooperative Group Performance Status.
Feasibility outcomes
The primary objective of this pilot study was to determine the ability to recruit patients, as measured by the number of individuals enrolled per week, as well as the feasibility to retain patients. Following removal of the placebo arm and enrollment of the first patient, patients were enrolled at a rate of 2.8 per month, which was less than our goal of 1 per week. Reasons patients gave for declining participation in the revised trial included the burden of additional visits, not wanting to take an antidepressant, not wanting to see a psychiatrist, not wanting to gain weight, transportation difficulties, not wanting to participate in a clinical trial, and in some cases the denial of the diagnosis of depression. Only three patients (14.3%) withdrew from the study, satisfying our attrition goal of ≤50%. All withdrawals were in the mirtazapine stratum, two due to nightmares and one due to rapid progression of cancer and transition to home hospice. Medication adherence was assessed throughout the study through the use of pill counts.
Efficacy outcomes
The secondary objective of this trial was to assess the efficacy of the selected medications in managing depressive symptoms and QOL in patients with cancer (see Table 2). A significant improvement in PHQ-9 depression scores was seen in both the citalopram and mirtazapine groups (see Fig. 2). The depression response rate was 60% in the citalopram stratum, 36.4% in the mirtazapine stratum, and 47.6% overall. While we attempted to exclude patients with a life expectancy of <6 months, the inability to fully predict disease behavior led to the enrollment of three patients in the mirtazapine stratum who experienced significant progression of their cancer and who were actively dying during their final study visit. In examining their data, we saw an initial improvement in their PHQ-9 depression scores after enrollment, followed by a significant worsening at the time of their last visit. If these terminally ill patients are excluded from our analysis, we observe an even greater improvement in depression scores, with an overall depression response rate of 55.6%.
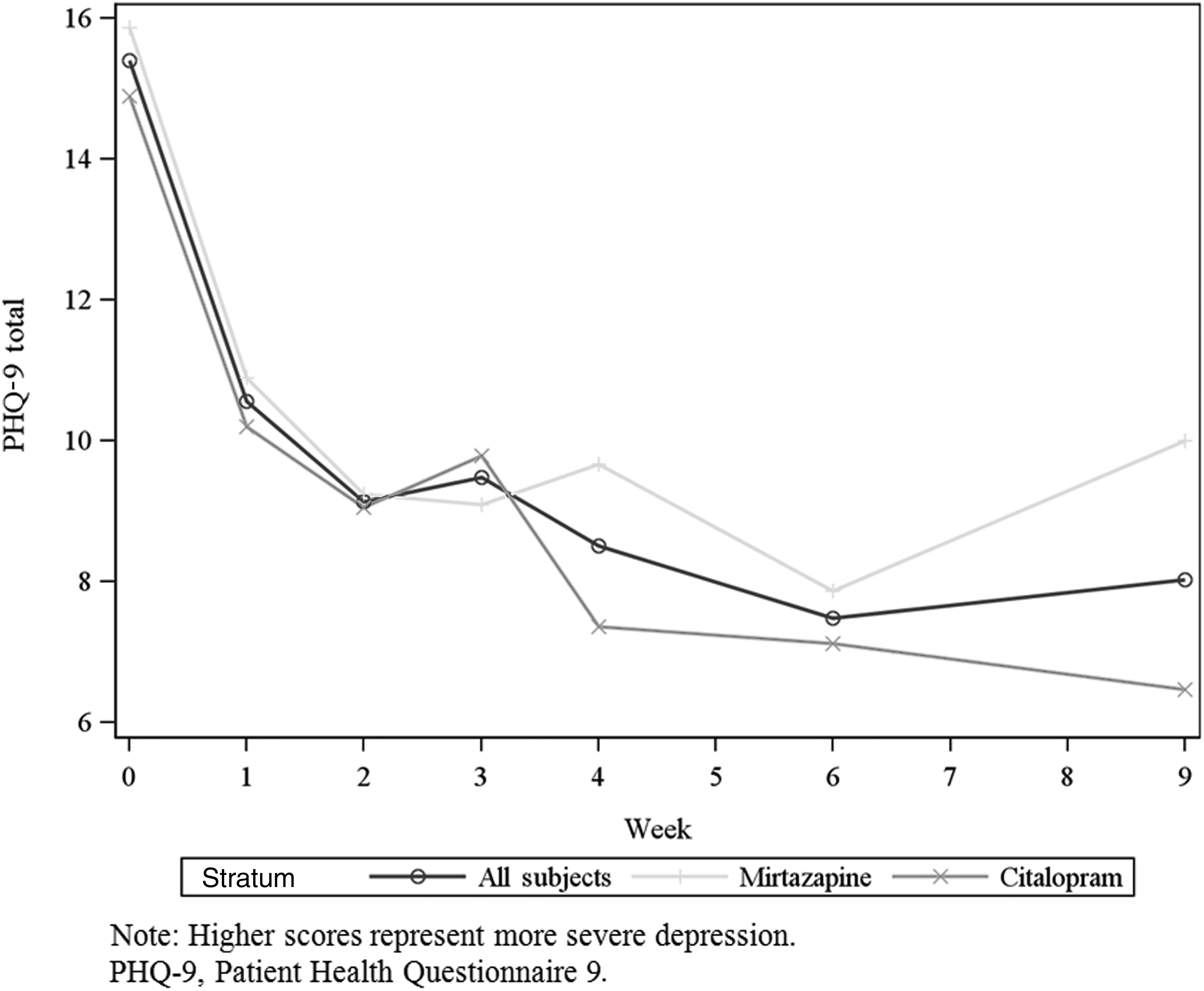
Depression scores over time (mean PHQ-9 score).
Change scores could only be calculated when there was an endpoint, so that some patients were left out of the analyses of change score.
Higher scores represent more severe depression.
Higher scores represent better quality of life.
Higher scores represent less fatigue.
Higher scores represent poorer sleep quality.
FACIT-Fatigue, Functional Assessment of Chronic Illness Therapy – Fatigue; FACT-G, Functional Assessment of Cancer Therapy – General; PHQ-9, Patient Health Questionnaire 9; PSQI, Pittsburgh Sleep Quality Index.
QOL scores, as measured by the FACT-G, improved from a mean of 57.4 to 73.0 for all patients (see Fig. 3). With the three actively dying patients excluded, the mean FACT-G improved from 58.4 to 77.2. Fatigue scores, as measured by the FACIT-Fatigue, improved from a mean of 23.3 to 31.0 for all patients (see Fig. 4). Sleep quality scores, as measured by the PSQI, improved from a mean of 10.7 to 7.7 (see Fig. 5). Self-reported sleep on the PSQI improved from a mean of 6.1 hours to 7.4 hours. The mean weight for all patients decreased by 1.2 kilograms.

Quality of life scores over time (mean FACT-G score).

Fatigue scores over time (mean FACIT-Fatigue score).

Sleep quality scores over time (PSQI).
Adverse events
Adverse events were evaluated at each encounter. There were a total of four serious adverse events, in which patients were admitted to the hospital for reasons that were determined to be unrelated to the study medication. Only two patients withdrew due to study medication-related adverse events, both experiencing nightmares while taking mirtazapine. Side effects were otherwise mild, as expected and previously reported for these two medications. The most common adverse events observed, in order of frequency, were fatigue, nausea, decreased appetite, diarrhea, insomnia, and dry mouth. Many of the reported adverse events may have been directly related to the patient's underlying malignancy and oncologic therapy, rather than to the study medication.
Discussion
Conducting antidepressant clinical trials in the oncology population is challenging. In this pilot study, our novel design attempted to overcome some of these challenges by using the increasingly common clinical strategy of selecting an antidepressant with a side effect profile tailored to a patient's dominant cancer-related symptoms. For this purpose, we chose two very different FDA-approved antidepressants with properties that make them particularly attractive for use in cancer patients. Mirtazapine is a tetracyclic antidepressant that is also a powerful antiemetic, an effective therapy for insomnia in cancer patients, and a known appetite stimulant that commonly causes weight gain.27,34–38 Citalopram, a selective serotonin reuptake inhibitor (SSRI), is preferred over other SSRI medications for patients with cancer due to its excellent tolerability and relative lack of drug interactions.26,33,39,40
Our original trial design involved the use of a placebo control. Randomized double-blind placebo controlled trials are preferred for antidepressant medications due, in part, to their historically high and variable placebo response rates.41–46 Unfortunately, we found the use of a placebo to be a major barrier to accrual. Of the eligible patients who initially met with the research team, all declined participation, and with few exceptions, the reasons were directly related to the use of a placebo. Some patients declined due to what they perceived were unacceptable risks involved in receiving a placebo, others were excluded due to their inability to swallow the large capsules necessary for the placebo blinding process, and many declined due to the burden of frequent visits, which was considered a necessary safety feature in the setting of placebo use.
Our experience suggests that patients with cancer who have clinical depression and qualify for antidepressant trials are reluctant to accept a placebo arm regardless of assurances of careful monitoring and crossover designs. For this reason we redesigned the trial to remove the placebo arm, as well as to permit more flexibility in patient scheduling and to allow for some evaluations to be done over the phone. However, while we were successful at accruing patients with this modified design, recruitment remained a challenge for several reasons, including patients' competing priorities, given the demands and complexity of concomitant oncology care, the lack of a systematized depression screening and referral mechanism, and the widespread use of antidepressants in standard practice by many oncologists at our institution. We were successful at retaining patients, with a retention rate that is consistent with other antidepressant trials. 33
As a feasibility and nonrandomized study, this trial was not designed to directly compare the efficacy of mirtazapine and citalopram in cancer patients. However, descriptive statistics were performed and revealed significant improvements in depression and QOL scores in both medication arms as well as the study group as a whole. Due to the lack of placebo control, we cannot attribute these improvements to the antidepressant. However, these results do suggest that our intervention, whether due to the medication, the effects of time, or the psychosocial support, was associated with clinically significant improvements in our study patients, with an overall reduction in mean depressive scores from “moderately severe” to “mild.” 22 We additionally saw an overall depression response rate (47.6%) that is comparable to historical controls in patients without cancer.33,41,46 QOL and fatigue scores (as measured by the FACT-G and FACIT-Fatigue respectively) improved by 15.6 and 7.8 points, while prior studies indicate that changes as small as four points and three points in these respective instruments represent clinically significant improvement. 47 Global improvements in sleep quality and duration were also noted.
This trial also examined the overall approach of stratifying cancer patients to different antidepressants based on their symptom profile. As one would expect, the patient characteristics in each of these groups differed considerably, with anorexia as a criterion for selection of mirtazapine, resulting in a sicker population of patients assigned to this stratum. These differences in baseline characteristics had a clear impact on depression and QOL outcomes, as patients with more advanced illness were less likely to have a clinically significant response to antidepressant therapy in our trial. The effects of stratification may have also affected responses to sleep quality and weight gain, as patients with self-reported insomnia and weight loss were preferentially assigned to the mirtazapine stratum. We had anticipated that patients receiving mirtazapine would experience weight gain given the results of previous studies with this medication in cancer patients.37,38 To the contrary, we observed that these patients actually lost a small amount of weight over the study. These results suggest that, in cancer patients with significant anorexia at baseline, the appetite stimulant effects of mirtazapine may not be sufficient to overcome the progressive cancer-induced weight loss. Similarly, the sleep-promoting effects of mirtazapine may be attenuated in cancer patients with more severe sleep problems.
There are several limitations to this study. As a feasibility trial, one of our primary objectives was to uncover these limitations and to learn from them. As previously mentioned, this trial lacked a placebo control, and recruitment numbers were lower than anticipated due to a variety of challenges. There was also an inherent referral bias, as only patients referred to the psychiatry team were evaluated for eligibility. Perhaps the most significant limitation of this study was the lack of objectivity within our stratification process, which was determined by patient prioritization of target symptoms rather than the use of formal symptom assessment instruments. In this medically ill population, it is more challenging to apply the symptom matching approach, as patients present with an array of complex clinical symptoms that fluctuate over time with management of their underlying malignancy.
In a recent evidence-based review, only half of studies showed efficacy in treating MDD in patients with cancer. 19 There is a need to identify and study medications that have consistent benefit and are well tolerated in this population where depression is interrelated with anxiety, nausea, and other symptoms. This small feasibility trial has demonstrated that investigation of antidepressants in patients with cancer can be done, albeit with some difficulty. Despite these challenges, additional research is warranted given the burden of depression in cancer. Future trials will need to have a homogeneous population that is well balanced between treatment arms and adequate power to ensure the validity and reproducibility of results. Investigators should additionally consider alternative stratification approaches when studying the management of depression in patients with cancer.
Footnotes
Acknowledgments
This research was supported in part by a grant from the Lineberger Comprehensive Cancer Center University Cancer Research Fund.
The authors would like to acknowledge Hillary Little, our research assistant, who was instrumental in the initial development and planning of this trial. We would additionally like to acknowledge the patients who volunteered their time to participate in this study.
Author Disclosure Statement
No competing financial interests exist.