
Abstract
Abstract
Background:
Lung cancer is the leading cause of cancer-related death.1 Accurate prediction of survival in the terminal stage is important, because it may help patients make a rational decision. Although several prognostic scores have been described as effective indicators of outcome, these scores were intended for patients with other types of cancers. There is no prognostic score for patients with terminal-stage lung cancer.
Objective:
The aim of this study was to determine prognostic factors for patients with terminal-stage lung cancer.
Setting/Subjects:
Patients in our palliative care unit (PCU) were selected retrospectively and divided into two independent groups, training and testing. Univariate and multivariate analyses were performed on data from the training group to detect independent prognostic factors, while data from patients in the testing group were analyzed to validate whether these prognostic factors predicted near-term death.
Results:
Ninety-three patients (69 in the training group and 24 in the testing group) were included in the analyses. Multivariate analysis showed that fatigue, anorexia, desaturation, hyponatremia, and hypoalbuminemia were independent prognostic factors in the training group. Mean survival time in patients who had more than three of these five factors was 9.2±2.6 days (p=0.012). In the testing group, the presence of more than three of these five factors predicted death within two weeks, with a sensitivity of 100% and specificity of 75%.
Conclusions:
This study revealed that fatigue, anorexia, desaturation, hyponatremia, and hypoalbuminemia may be short-term prognostic factors in terminally ill lung cancer patients. In particular, the presence of more than three of these factors predicted death within two weeks.
Introduction
L
Accurate prediction of survival in terminally ill lung cancer patients is important for physicians, since it may help them make a rational decision about the best location for care (i.e., home care, hospice, or PCU). Several studies have suggested that dyspnea, malnutrition, weight loss, 6 delirium, 7 treatment with opioids and/or glucocorticoids, 6 poor Karnofsky performance status (KPS), 7 and poor Eastern Cooperative Oncology Group (ECOG) performance status (EPS)8,9 are factors that can predict the prognosis of oncology patients. In particular, general symptoms, psychosocial well-being, 10 and quality of life11–14 have been suggested as prognostic factors in patients with lung cancer. Moreover, prognostic scores such as the palliative prognostic score (PaP) 15 and the palliative prognostic index (PPI) 16 have been reported to be effective indicators of prognosis. These studies included patients with a variety of cancers and focused on determining appropriate prognostic factors for cancer patients on their first visit or before treatment, not for terminally ill cancer patients. However, there are no predictive prognostic scores for patients with lung cancer in the terminal stage.
Therefore, the aim of this study was to investigate factors in patients with lung cancer in the terminal stage in order to establish lung cancer specific prognostic factors.
Methods
Patient population
This retrospective study was performed at Komatsu Municipal Hospital, a 364-bed community hospital in Komatsu City, Ishikawa, Japan. This hospital is the only facility treating lung cancer in this area of 230,000 people. In 2012, 367 patients were newly diagnosed with lung cancer at this hospital, while only 31 patients (8.4%) were admitted to the PCU. Patients who met the following inclusion criteria were included in the study: (1) lung cancer confirmed pathologically or clinically and (2) admission to the PCU in the hospital from April 2009 to June 2012 (training group) and from July 2012 to June 2013 (testing group). In our PCU, patients with malignancy who had not received any specific anticancer therapy at the time of admission except for palliative chemotherapy and radiation therapy were admitted voluntarily. This study protocol was approved by the institutional review board of Komatsu Municipal Hospital.
Factors of analysis
Clinical data were collected by review of electronic medical records. Twenty-six candidate predictors were chosen from published clinical studies as potential predictive factors.6–9,15,16 All of the patients were examined at the time of admission to the PCU. In addition to laboratory parameters, several scales designed specifically for measurement of physical status were measured. The EPS uses a scale from 0 to 5, with 0 denoting perfect health and 5 death. 17 The KPS is assessed from 100 to 0, where 100 is “perfect” health and 0 is death. 18 In addition, two major scoring systems for predicting prognosis in the PCU were calculated: the PaP score and the PPI score. The PaP score includes anorexia, dyspnea, total white blood count, and lymphocyte percentage in conjunction with the KPS and expert clinical prediction of survival. 15 The PPI, originally defined by the Palliative Performance Scale (PPS), also includes measurements of oral intake, edema, dyspnea at rest, and delirium. 16 Blood examination data were collected within one week from the registration. Continuous variables of the factors were divided into two categories as follows: age (<70, ≥70); KPS (<50, ≥50); EPS 17 (<4, ≥4); PaP (<11, ≥11); PPI (<6, ≥6); body temperature (BT) (<37.1, ≥37.1°C); oxygen saturation (SpO2; <93%, ≥93%); white blood cell (WBC) (<8500, ≥8500 cells/μL); lymphocyte (Lym) (<20%, ≥20%); C-reactive protein (CRP) (<0.03, ≥0.03 mg/dL); lactase dehydrogenase (LDH) (<230, ≥230 IU); sodium (Na; <135, ≥135 mEq/L); calcium (Ca; <8.6, ≥8.6 mg/dL); blood urea nitrogen (BUN; <17, ≥17 mg/dL); and albumin (Alb; <2.7, ≥2.7 g/dL). The cut-off points for BT, SpO2, WBC, CRP, LDH, Na, Ca, and BUN were set at the value that demarcated the normal and abnormal ranges, whereas Alb was based on the median value.
Statistical analysis
To identify factors correlated with survival, the log rank test was performed using the 26 candidate predictors in the training set. Factors that were significantly related with survival were extracted, and multivariate analysis was performed for these factors using the Cox proportional hazards regression model. Finally, to determine the number of factors predicting short-term death, patients were divided into groups categorized by the number of factors that were estimated to be independent prognostic factors in multivariate analysis. The appropriate number of the factors was defined as the cut-off point in our study. The validity of the prediction was then examined on all assessments in the testing set. In addition, to determine sensitivity and specificity, and the positive predictive value (PPV) and negative predictive value (NPV) in this study, the PaP and PPI scores were compared in order to measure the accuracy of predicting short-term death.
Differences were assumed to be significant when the p-value was <0.05. Continuous variables with a normal distribution were compared using Student's t-test and the Wilcoxon rank-sum test for nonnormally distributed variables. The χ2 statistic or Fisher's exact test were used to compare categorical variables. Survival rates were analyzed using the Kaplan-Meier method. Overall survival time (OS) was calculated from admission until death and included data from other facilities. All the analyses were performed using SPSS 20.0.0 (SPSS, Armonk, NY).
Results
Patient characteristics
Patient characteristics are shown in Table 1. A total of 69 patients were eligible for participation in the training group and included 38 men (51%) and 31 women (49%). Twenty-two of the 69 patients (32%) died within two weeks, and the remaining 47 (68%) survived for longer than two weeks. The mean age of patients in the training group was 75±10 years. Fifty-one (74%) patients had received antitumor therapy prior to admission to the PCU. Adenocarcinoma was the most common histologic type (n=35, 51%). The median overall survival for all 69 patients was 30 days. The characteristics of the patients in the testing group are summarized in Table 1. This shows that the mean age of the patients was 73±7.9 years, 8 patients (33%) were female, and 17 patients (71%) had received antitumor therapy. The median survival time of patients in the testing group was 26 days. The patient characteristics in the two groups were not significantly different (see Table 1).
EPS, Eastern Cooperative Oncology Group performance status; KPS, Karnofsky performance status; LCNEC, large cell neuroendocrine carcinoma; SD, standard deviation.
Analysis of prognostic factors
The results of univariate analysis using the log rank test in patients in the training group are shown in Table 2. Eight of 26 parameters were associated significantly with survival, namely the PaP (p<0.0001), desaturation (p<0.0001), supplemental oxygen (p=0.002), anorexia (p=0.002), fatigue (p=0.003), dyspnea (p=0.031), hypoalbuminemia (p=0.0015), and hyponatremia (p=0.014). Multivariate analysis was then used to analyze the prognostic significance of these eight factors (see Table 3). Multivariate analysis showed that fatigue (p=0.001, hazard ratio [HR]: 5.90, 95% confidence interval [CI]: 2.04–17.0); anorexia (p=0.023, HR: 2.57, 95% CI: 1.14–5.88); desaturation (p=0.005, HR: 3.30, 95% CI: 1.42–7.65); hyponatremia (p=0.049, HR: 2.17, 95% CI: 1.01–4.68); and hypoalbuminemia (p=0.037, HR: 2.37, 95% CI: 1.05–5.36) were considered independent factors predicting short-term prognosis.
Alb, albumin; BT, body temperature; BUN, blood urea nitrogen; CRP, C-reactive protein; EPS, Eastern Cooperative Oncology Group performance status; KPS, Karnofsky performance status; LDH, lactate dehydrogenase; Lym, lymphocytes; PPI, palliative prognostic index; PPS, palliative prognostic score; WBC, white blood cells.
CI, confidence interval.
We divided the patients into two groups having either 0–2 of these factors (0–2 group) or >3 of these factors (3–5 group). The mean survival time of the two groups was analyzed using the Kaplan-Meier method. As shown in Figure 1, the mean survival time was 48±5.1 days in the 0–2 group and 9.2±2.6 days in the 3–5 group.
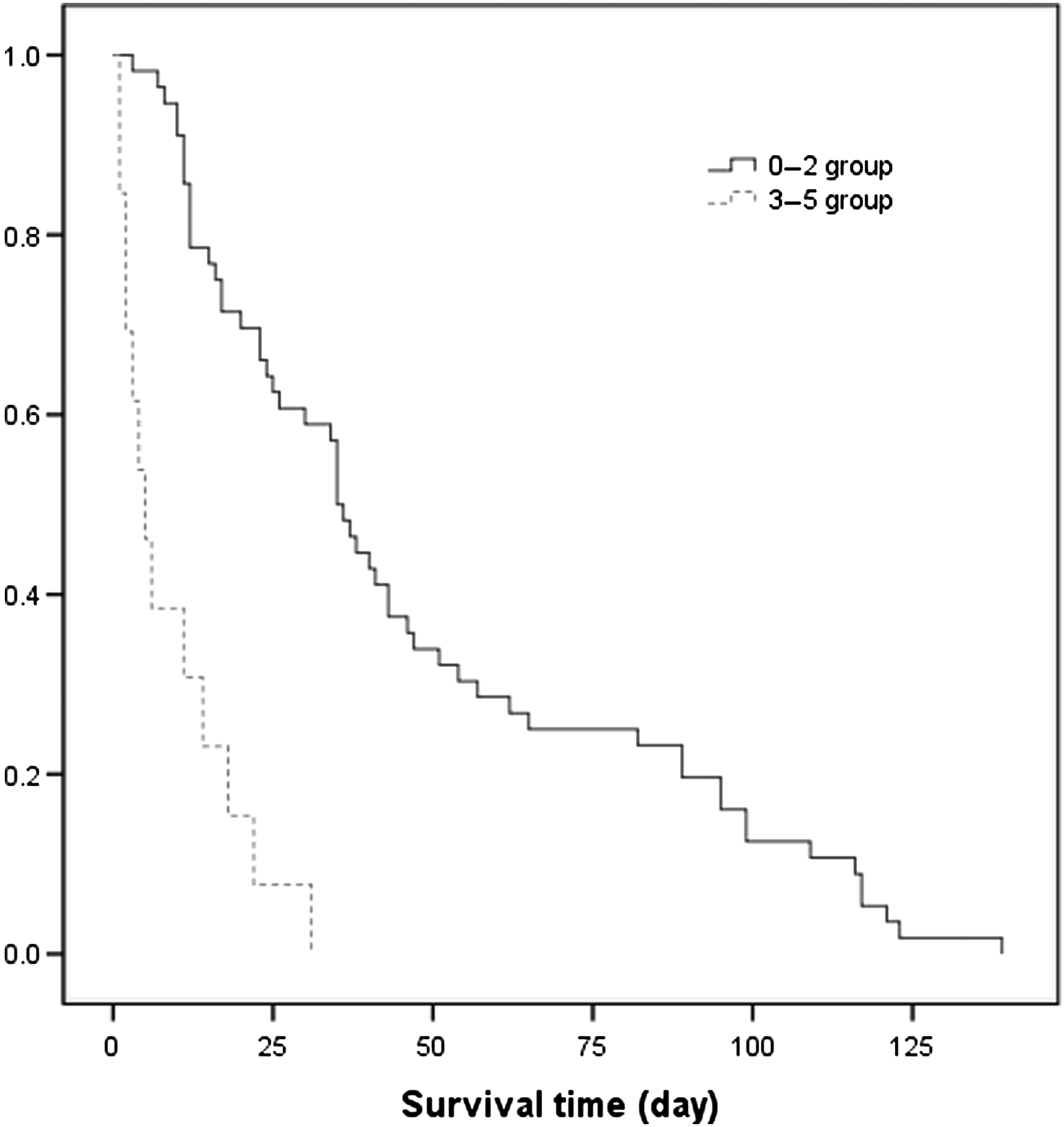
Survival curves of the 0–2 and 3–5 groups in the training group.
These results indicate clearly that more than three of these five factors predicted death within two weeks in patients with terminal lung cancer. We then analyzed the sensitivity, specificity, PPV, and NPV to predict death within two weeks in the training group. When more than three items were used, the sensitivity was 59%, specificity 94%, PPV 77%, and NPV 87%.
In the testing group, the presence of more than three of the five factors predicted death within two weeks with a sensitivity of 100% and specificity of 75%. In comparison, the PaP predicted death within three weeks with a sensitivity of 21% and specificity of 100%, while the PPI predicted death within four weeks with a sensitivity of 66% and specificity of 100% (see Table 4).
PaP, palliative prognostic score; PPI, palliative prognostic index.
Discussion
This study revealed that suffering from fatigue, anorexia, desaturation, hyponatremia, and hypoalbuminemia may be prognostic factors in terminally ill lung cancer patients. In particular, the presence of more than three of these factors could be used to predict death within two weeks. These factors may also be useful for untrained personnel in PCUs because the factors were either categorical variables (i.e., positive or negative) or continuous measured values.
MacEachern and colleagues stated that experienced physicians generally predict four-week survival with a sensitivity of 48%–64% and a specificity of 73%–91%. 19 Therefore, the values obtained in the present study (100% sensitivity and 75% specificity in the testing group) were acceptable for predicting death within two weeks using a cut-off point of three of the identified factors.
Desaturation, i.e., low blood oxygen concentrations, was also correlated with prognosis in this study. Generally, patients with chronic hypoxia, such as those with chronic obstructive pulmonary disease (COPD), suffer from anorexia. 20 Adaptation to low oxygen tension (hypoxia) in cells and tissues is regulated by hypoxia-inducible factor-1 (HIF-1) and leads to the transcriptional induction of a series of genes that participate in angiogenesis, iron metabolism, glucose metabolism, and cell proliferation/survival.20,21 HIF-1 induced by hypoxia in COPD patients is assumed to be responsible for changes in various metabolism factors that result in anorexia and body weight loss. This suggests that hypoxemia could be correlated to anorexia in terminally ill lung cancer patients as well, although the relationship between anorexia and HIF-1 in these patients is not yet clear.
Hypoalbuminemia was also related to mortality in our study. Hypoalbuminemia is generally seen in terminal cancer patients due to the presence of anorexia and chronic inflammation in association with cachexia. In addition, hypoalbuminemia is related to malnutrition, and both of these characteristics are common in patients with lung cancer. 22 Malnutrition has been associated with a number of clinical consequences, including deteriorated quality of life, decreased response to treatment, increased risk of chemotherapy-induced toxicity, and a reduced survival.23–25 Moreover, several studies have found that higher serum albumin levels are associated with better survival in multivariate analyses.26,27 In this study, anorexia was an independent predictor of death within two weeks; indeed, the presence of anorexia may be related to hypoalbuminemia. In a similar fashion, malnutrition and anorexia were correlated with hyponatremia, also an independent prognostic factor for survival. Deficiencies in sodium intake caused by anorexia seem to bring about hyponatremia. Similarly, Castillo and colleagues demonstrated that hyponatremia is an independent risk factor for poor outcomes in patients with small-cell lung cancer. 28
The PaP 15 and the PPI 16 are prognostic predicting scores used in terminally ill patients. In contrast to our study, which only investigated lung cancer patients, studies describing the PaP and PPI15,16 have included patients with various types of cancer, such as lung, stomach, breast, pancreas, colorectal, and bladder cancer, among others. Moreover, anorexia is common to the PPS and the PPI, while fatigue, hyponatremia, and hypoalbuminemia are not included in the PPS and PPI. Morita and colleagues suggested that although the effects of disease-related pathology and psychosocial factors on survival are controversial, some clinical symptoms, such as performance status, nutritional disturbance (e.g., anorexia, lowered oral intake, weight loss, edema, dysphagia), dyspnea especially at rest, and delirium are useful prognostic indicators. Therefore, lowered oral intake, edema, dyspnea, and delirium were included in the PPI. 16 Although that study did not state in detail, these clinical factors (lowered oral intake, edema, dyspnea) may be appropriate symptoms due to their association with cachexia in prognostic scores. Similarly in our study, the presence of cachexia indicated a poor prognosis and predicted short-term survival. Unlike anorexia, desaturation differed between the PaP and PPI. Hypoxemia is a common symptom in patients with advanced cancer, estimated as a moderate or severe problem in 46% of those admitted to a palliative care program, and is thought to affect 70% of hospice inpatients. 29 This hypoxemia is likely due to the presence of pleural effusion, constriction of trachea, atelectasis, lymphangitis, pulmonary embolism, and pneumonia, which could lead to dyspnea, a condition commonly seen in advanced cancer patients.30,31 In particular, most terminally ill lung cancer patients need oxygen supplementation due to their desaturation. 2 Therefore, desaturation is a characteristic factor in terminal patients with lung cancer, and oncologists and pulmonary physicians should estimate desaturation in terminal stages of the disease to give insight into predicted survival.
Our study has some limitations. First, it was a retrospective analysis that included a very small population. Second, we did not use an objective tool to evaluate the symptoms of terminally ill cancer patients. Third, only patients who were admitted to our PCU were evaluated in our study. In the real world, many terminal lung cancer patients die in hospitals, nursing homes, and their own homes in Japan. Finally, since this was a retrospective study, it is possible that some selection bias was present. Therefore, further prospective studies using objective tools and more patients will be required to confirm and expand upon these results.
Conclusions
This study revealed that fatigue, anorexia, desaturation, hyponatremia, and hypoalbuminemia may be factors predicting prognosis in terminally ill lung cancer patients. In particular, the presence of more than three of these factors predicted death within two weeks with a high degree of specificity and sensitivity. Since the number of lung cancer patients is estimated to increase year by year, clinicians who do not specialize in oncology or pulmonology will be required to treat these terminally ill patients. Therefore, these findings may be helpful for clinicians to make decisions. Further prospective studies to confirm the significance of these results are warranted.
Footnotes
Acknowledgments
We are grateful for the diligent and thorough critical reading of our manuscript by John Wocher, executive vice president and director, International Affairs/International Patient Services, Kameda Medical Center (Japan). We also appreciate the expert assistance with the statistical analyses in the study provided by Kazuki Yoshida, research fellow, Division of Rheumatology, Immunology and Allergy, Brigham and Women's Hospital (United States).
Author Disclosure Statement
No competing financial interests exist.