
Abstract
Abstract
Background:
Hospice and palliative care are underutilized among patients at the end of their lives despite evidence that they improve patient satisfaction and reduce costs.
Objective:
To synthesize evidence regarding interventions to increase hospice referral/enrollment.
Design and Measurements:
We conducted a systematic review of the literature and selected studies that evaluated interventions aimed at increasing hospice use. We performed a MEDLINE search (1979 to April 2013) supplemented by manual searches of bibliographies of key articles. Study design, quality criteria, population, interventions, and outcomes for each study were extracted. The main outcome evaluated was hospice referral/enrollment.
Results:
Our search strategy yielded 419 studies, of which only 6 met our eligibility criteria. Three studies included nursing home populations; 1 included home care patients, 1 targeted care managers, and 1 reported on heart failure patients. Three studies had a cohort design, 2 were pre–post, and only 1 was randomized. Two studies evaluated a process to identify eligible subjects. Two evaluated the impact of advance care planning programs and 2 only provided education. Interventions that only provided education showed a median increase in referral of 5% (2.8%–17%) while interventions that identified hospice candidates showed a median increase in hospice referral of 19.5 % (19%–20%).
Conclusions:
Interventions of different levels of complexity can improve the use of hospice services among subjects with high mortality risk. An approach that allows the medical team to assess patients' treatment goals and that engages the treating physician seems to be the most successful one.
Introduction
A
However, hospice care is underused or used so late in the course of the illness that the efficacy of the program and satisfaction with hospice services are reduced. 11 The SUPPORT trial found that among noncancer patients who survived a hospitalization only 5.1% of those referred to hospice lived beyond the estimated 6 months while 99% of the patients who died within 6 months were not enrolled in hospice. 12 These findings highlight the challenges we face in achieving timely identification of hospice eligible subjects.
In fact, only 20%–25% of people who die in the United States utilize hospice services and 50% of those referred spend 22 days or less in hospice care. 13 Ten percent of hospice patients are enrolled during the last 24 hours of their life. 14 This underutilization is likely due to misunderstanding of aspects of hospice care by both physicians and patients. 15 Among physicians, referral to hospice may be perceived as a professional failure that can dissuade them to withdraw curative attempts. 16 In addition, physicians receive little training in the compassionate discussion of bad news 15 and prognostication, 12 particularly among ethnic minorities. 17
In light of these data, a number of health systems and investigators have attempted to improve the process of hospice referral among the patients they serve. This study aims to systematically review data on interventions that attempted to improve hospice referral and enrollment and identify characteristics of the interventions that seem to address barriers to referral successfully.
Methods
Search strategy
We conducted a MEDLINE database search in April 2013 that was supplemented by a manual search of bibliographies of key relevant articles that had no electronic published version. Our window period was 1979 to 2013. We initially conducted a comprehensive search using multiple terms, which did not yield enough articles for the needed purpose, therefore, another search was done using the more general terms: “intervention” and “hospice.” Our search terms were as follows: (“Intervention” [Journal] OR “Interv Sch Clin”[Journal] OR “intervention”[All Fields]) AND (“hospices”[MeSH Terms] OR “hospices”[All Fields] OR “hospice”[All Fields] OR “hospice care”[MeSH Terms] OR (“hospice”[All Fields] AND “care”[All Fields]) OR “hospice care”[All Fields]). We then conducted a search using all the MESH terms present on the identified articles but no additional articles were found. The final literature search included only articles in English.
Inclusion criteria
We screened abstracts for interventions intended to improve hospice referral or enrollment. To be included, the studies had to fulfill the following criteria: have a well-defined intervention, identify as outcome either hospice referral or hospice enrollment, and quantitatively compare the outcome variable between the intervention group and a control group, or between time periods before and after the intervention was implemented.
Data abstraction
Two investigators (I.K.) and (L.T.) completed the evidence tables. Differences between the two reviewers were resolved by consensus among four of the investigators (I.K., L.T., A.P., and E.S.).
Exposure variable
The key exposure variable was the intervention to improve hospice referral or enrollment.
Outcomes
Primary outcome
The primary outcome of interest was the rate of either hospice referral or enrollment, defined as the number of patients that were either referred or enrolled in hospice during the evaluation period. We used the Medicare benefit definition of hospice, namely a program “that provides interdisciplinary care to patients with a terminal illness and a prognosis of <6 months and to their families. Hospice services range from symptom management to bereavement care.” 18 We did not include palliative care referrals in our outcome of interest.
Secondary outcomes
We evaluated two additional outcomes when data were available for comparison: the presence of a health advance directive and the presence of a do-not-resuscitate (DNR) order.
Qualitative evaluation
We used the Jadad et al. 19 and STROBE checklists 20 to assess the quality of the studies reviewed. The Jadad et al. 19 checklist was used for the randomized clinical trial and evaluated items such as randomization, blinding, and dropouts. In this checklist, a maximum score of 5 can be obtained by a rigorous study and a study is considered low quality if the score is between 0–2. The STROBE checklist 20 was used for the observational studies to assess if items that should be included in an observational study are present. The items evaluated in the article are found in the title, abstract (item 1), the introduction (items 2 and 3), methods (items 4–12), results (items 13–17), discussion sections (items 18–21), and other information (item 22 on funding). We used the twenty-second item for our evaluation since we included both cohort and cross-sectional studies. We used 18 items that are common to the 2 designs, while 4 (items 6, 12, 14, and 15) are design specific, with different versions for all or part of the item. We assigned a score of 1 to each item if the item had been met appropriately or 0 if not and then summed the individual scores with a maximum possible score of 22. Two investigators were responsible for completing the quality evaluation (I.K./L.T.). Differences between the two reviewers (I.K./L.T.) were resolved by consensus that was done by I.K., L.T., A.P., and E.S.
Results
Our search strategy identified 419 articles; we excluded 391 at the title and abstract level due to irrelevance to the subject. Twenty-eight articles included a palliative care/hospice intervention, 11 of these were excluded because they discussed only interventions to improve quality of care and/or services offered by hospice to their patients and caregivers. Two studies were excluded because they did not include any numerical data for hospice referral or enrollment. Of 15 articles that included numerical data on the number of patients referred to and enrolled in hospice, 9 were excluded because the numerical data were not enough to conduct a statistical comparison between the groups. In conclusion only 6 studies provided the number of referrals before and after intervention or for the control and intervention groups. These 6 articles were included in this study. Figure 1 depicts the inclusion and exclusion of studies.

Search strategy and choice of included studies.
Description of study design and population of the included studies
Six studies met the inclusion criteria (Table 1); the studies were published between 2005 and 2013.21–26 The median follow up time was 1.5 years and range from 1 to 2 years. We identified one randomized control trial, 21 two pre–post studies,23,26 and three retrospective cohort studies.22,24,25 Three of the six studies reported on intervention among nursing home patients.21,23,25 The other three reported on home care patients, 24 heart failure patients, 22 and Medicaid care managers. 26 All studies evaluated a total of 3559 patients. The mean ages of participants ranged from 65 to 86 years old. The number of females exceeded the number of males in almost all studies except in one study in which the numbers were equal. The percentage of white subjects ranged from 63% to 87% of all included subjects.
RCT, randomized controlled trial.
Qualitative results
We included one randomized trial in our systematic review. The JADAD scale assigned a low quality score to the study due to the fact that the trial was not blinded. Nevertheless, blinding in this type of intervention is probably not feasible because it was evident to the study team where the patient was going to receive care at the end of life. For three of the four observational studies the major quality concern was the lack of multivariate analysis to adjust for important confounders like insurance and comorbidities. Another concern was the lack of reporting on how loss to follow-up and missing data was handled.
Description of the intervention
All interventions attempted to facilitate the process of hospice referral; however the actual interventions varied slightly from study to study (Table 2). All six interventions implemented staff training of end-of-life care issues. Two of these interventions added a process by which physicians interacted with staff to facilitate the identification of eligible subjects.21,25 Two evaluated the impact of advance care planning programs on hospice referral or enrollment22,24 and two studies focused on quality improvement by providing educational sessions to the nurses staff/case managers.23,26 The education process was focused on advanced care planning, goal clarification, education on the disease and symptoms management. Hospice providers and palliative care experts such as physicians, nurses, social workers, and physical therapists conducted most of the educational sessions.23,24,26 In more detail, in Casarett et al. 21 and Levy et al. 25 the intervention attempted to help physicians identify patients in need of hospice care through either patient interviews or the use of a mortality prediction tool.
RCT, randomized controlled trial.
Schellinger et al. 22 evaluated the impact that a disease-specific advance care planning had on hospice referral or enrollment among congestive heart failure patients.
Similarly Ciemins et al. 24 evaluated the impact of Advanced Illness Management (AIM), a home-based program established to ease the transition between curative and comfort care for seriously ill patients. Ciemins et al. 24 compared hospice enrollment among AIM subjects and those with similar symptom burden and prognosis receiving regular home health services.
Two of the interventions,23,26 evaluated the impact of quality improvement programs that focused on the appropriate training of nursing staff or the care managers. In Beyea et al. 26 the intervention targeted Medicaid case managers from a primary care network. In Hanson et al., 23 participating nursing homes developed palliative care teams that received monthly onsite educational sessions and strategy meetings aimed at improving end-of-life care. Table 2, has detailed descriptions for all interventions.
Primary outcome: rate of referral to hospice
Five studies showed a statistically significant increase in hospice referral (Fig. 2). The increase in referral rates ranged from 2.8% to 20%. Interventions that focused on education of personnel23,24,26 in contact with patients eligible for hospice care showed a median increase in referral of 5% (range, 2.8%–17%). Interventions that tested processes of identifying hospice candidates21,22,25 showed a median increase in hospice referral of 19.5% (range, 19%– 20%)21,22 with the exception of the study by Levy et al., 25 which showed no increase in the rate of hospice referral. However, Levy et al. 25 did show an increase in palliative care referrals of 23.7%.
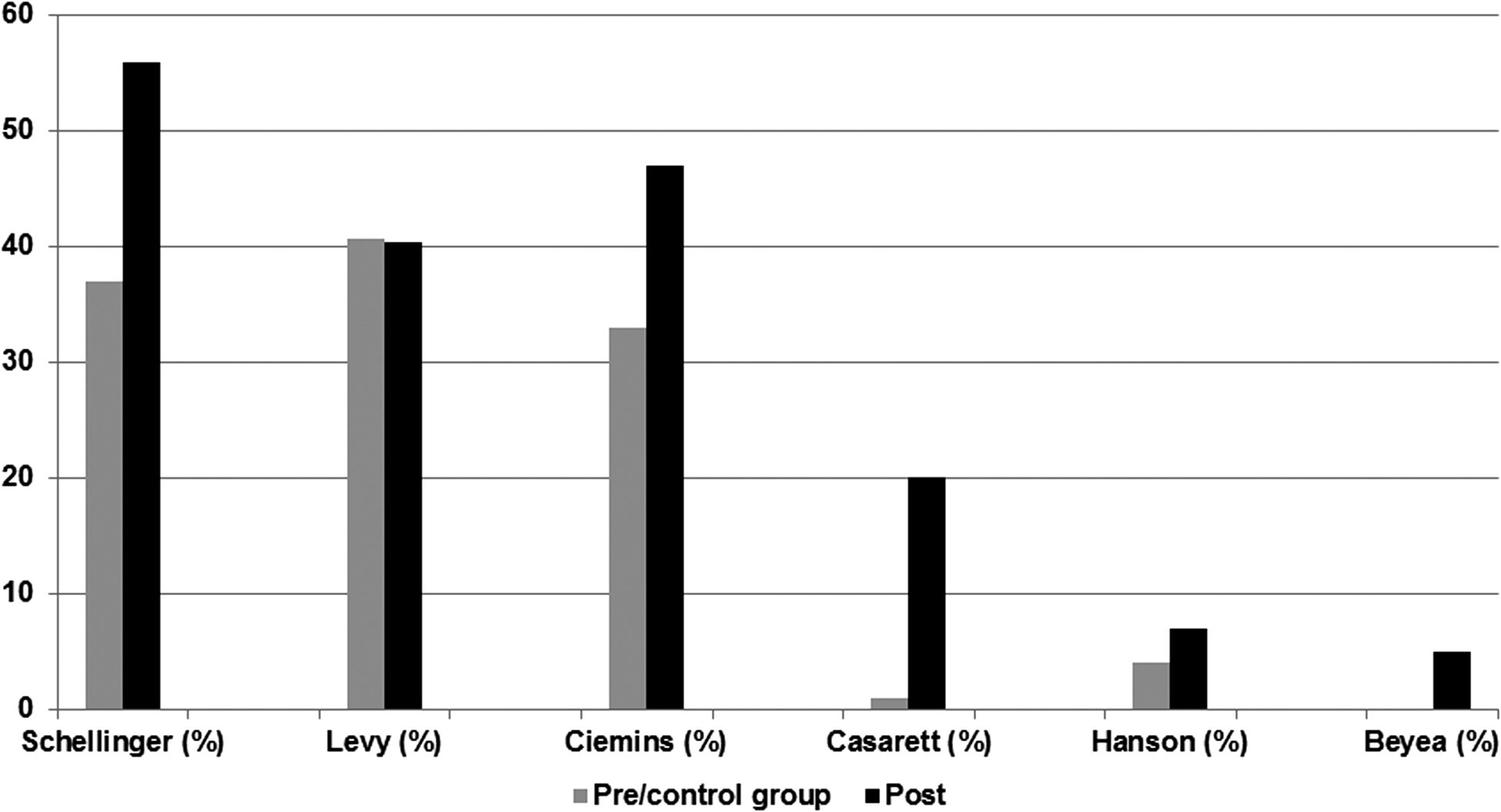
Rates of referral to hospice care in included studies.
Ciemins et al. 24 offered stratified analyses by race and showed significantly higher impact among African Americans. The absolute differences in percent of patients referred to hospice in the entire cohort ranged from 13% when AIM was compared to within branch controls and 31.4% when compared to external branch controls. Among African Americans these absolute differences were 28% and 34.5%, respectively. 24
Secondary outcomes
Presence of health directives was measured in two studies: Schellinger and colleagues 22 and Levy and colleagues. 25 In both studies, a statistically significant increase in the number of patients with a documented advance directive was observed after the intervention. According to Schellinger et al., 22 94% of intervention patients had an advance health directive; compared to 24% in the control group (p<0.001). 22 Similarly in Levy et al., 25 before the intervention, 88% of residents had advance directives; this percentage had increased to 100% after the intervention was implemented (p=0.03). The presence of a DNR order was reported by two of the studies.23,25 According to Hanson et al., 23 the use of DNR orders increased from (58% to 65%, p=0.04). In Levy et al., 25 the presence of a DNR order increased by 20% after program implementation (63% versus 84%, p=0.003).
Discussion
Our study found that only six studies objectively evaluated the impact of interventions on hospice use. Five of the six studies were successful in increasing hospice referral or enrollment and two successfully increased the presence of advanced directives in the medical record. These studies used two distinct strategies: identification of appropriate hospice candidates and a process of referral that was feasible in the context of each health system. All of the successful interventions seemed to focus initially on creating opportunities or processes to identify patients with needs and goals of care compatible with hospice care rather than to identify subjects with a prognosis of less than 6 months of life. Moreover, the only study that used a mortality prediction tool as the initial identification step failed to show an increase in hospice referral although it showed an increase on palliative care referral. Addressing the patients' needs in the last 6 months of their lives has become a major concern in the medical field. 27 This has prompted a variety of strategies to improve end-of-life care. In this review, we found that the three studies that involved the patients' physicians in the process of referral to either hospice or to palliative care,21,22,25 had higher rates of referral compared to the studies that only used education of staff members as the main strategy to increase referral.23,24,26 A clinically relevant improvement in hospice referral requires the presence of clear processes of care that create time and space to discuss end of life options with patients. These results suggest that better prognostication although an important factor for timely participation in hospice, it may not be easily modifiable whereas a process to identify subjects with needs and goals that could be filled by hospice care can facilitate a transition from curative to palliative care. Casarett et al., 21 demonstrated that a very brief questionnaire to patients to identify appropriateness of hospice without taking into account the prognosis, was a successful initial strategy to trigger the hospice referral process. All the other studies that showed increased hospice use had processes that focused on hospice awareness, goal clarification, symptom control, quality of life, and care as the initial strategy and prognostication was done only after subjects were already considered palliative care/home care candidates. In fact Ciemins et al. 25 used a very broad and nonspecific question such as “Would you be surprised if this patient died within 6–12 months” as a mechanism to identify subjects, rather than requesting an accurate survival estimation. Interestingly, the only study that used objective prognostication as the initial step, also offered physicians the option of referring to either palliative care or hospice care (if survival was estimated to be less than 6 months). This study showed an increase in palliative care referrals but a small decrease in hospice care referrals. The tendency of providers to overestimate survival, 28 may have encouraged physicians to refer preferentially to palliative care instead of hospice care when given the option. Alternatively, not knowing the patients' preferences and goals may bias physicians toward a less drastic approach. In this sense, the results by Levy et al. 25 allow us to reflect on the fact that prognostication tools are better used after patients' needs and goals have been addressed.
A concern regarding the data in the studies included was the limited representation of minority populations.29–31 It is known that African American and Hispanics are less likely to use hospice services at the end of their lives. 31 Possible barriers to hospice referral in African American populations include lack of awareness, misconceptions regarding hospice being associated with withdrawal of all treatments, mistrust, 32 or a preference for the use of life-prolonging treatment, despite the presence of a poor prognosis 33 This may be considered a sign of respect for their loved ones. In addition, the lack of racial diversity among hospice staff represents another barrier for referral of minority populations. 33 This systematic review showed that even though most patients included were white, the impact of the intervention may be differentially higher among African American patients. 24 This demonstrates that advanced care planning interventions could benefit populations that are otherwise disenfranchised from the regular process of referral. This may be due to the fact that the AIM intervention was designed to address barriers rather than just identify subjects with poor prognosis. 24 Therefore, having teams with the necessary training to address a variety of multidimensional needs may be an important strategy to close a disparity gap in end-of-life care. One of the main limitations encountered in this systematic review is the small number of studies identified in the literature evaluating hospice referral or enrollment rates. The second limitation is the heterogeneity of the data available in the 6 studies which did not allow for calculating a summary statistic or for reporting in detail the components of each intervention.
The increase in hospice or palliative care referral shown in these studies seems to be due to two main reasons. First, all six studies created awareness regarding Hospice services and end-of-life care through structured training of health care personnel and developed a process to initiate a discussion regarding wishes, preferences, and goals of care.21–26 Second, those studies with the highest impact created a strategy to engage the patient's physician in the referral process or to connect him/her with the palliative care team.21,22,25
Health systems interested in improving the use of hospice/palliative care services should consider a wider involvement of palliative care teams with different departments within hospitals or nursing homes. Such an involvement could be accomplished through the creation of automatic processes to address patients' preferences or for consultation to the palliative team based on meeting predefined eligibility criteria such as having an end-stage condition and having goals of care that may be compatible with hospice care. Relying on receiving a prognosis of 6 months or less of remaining life from physicians as a trigger for hospice consultation may not be successful at increasing the number of referrals or the number of subjects interested in hospice care. Further clinician education on how to help patients and their families' transition from curative to palliative care is needed.
Conclusion
Hospice care referral can be significantly increased even among minorities by establishing clear processes of screening and identification that are sustainable within each specific health system and that focus primarily on identifying subjects with goals and preferences aligned with hospice care. Interdisciplinary collaborative work between all stakeholders should occur to develop feasible interventions that are likely to be successful.
Footnotes
Author Disclosure Statement
No competing financial interests exist.