
Abstract
Abstract
Background:
Methadone is a useful analgesic for neuropathic and nociceptive pain. However, there is little information about the use of methadone in the final days of life when a patient cannot swallow, discouraging its use by many palliative care physicians.
Objective:
The purpose of this study was to investigate the effectiveness of switching patients on oral methadone at the end of life to methadone by the buccal mucosa route.
Methods:
This is a case series comprising 36 patients on the Toronto Grace Palliative Care Unit (PCU) who took methadone between 2010 and 2012. Their health records were retrospectively reviewed. When patients could no longer swallow at the end of life, oral methadone was replaced with methadone solution in a concentration of 10 mg/mL, placed in the space between the buccal mucosa and lower molars.
Results:
Twenty-five patients met inclusion criteria for the series. Twenty-four (96%) of the patients tolerated methadone by the buccal route and were able to continue receiving it that way until they died. Methadone was discontinued by the buccal route in one case (4%) because of intolerance to having medication placed in the oral cavity. Of the patients who remained on buccal methadone, there was a need to increase the dose in two patients with the remaining patients taking the same dose of buccal methadone until they died.
Conclusion:
The cases reviewed suggest that methadone is well tolerated and effective when switched to the buccal route in patients at the end of life on a palliative care unit.
Introduction
M
Methadone is typically administered orally and is well absorbed in the gastrointestinal tract with an oral bioavailability of 80%. 5 Although effective and safe to administer by the rectal route, rectal methadone may not be acceptable to all patients. 7 Methadone is rarely administered intravenously in palliative care settings. When administered subcutaneously, methadone has been reported to cause local toxicity. 6
When a patient on established oral methadone enters the terminal phase of illness, he or she may lose the ability to swallow oral medications, which presents a challenge. Rotation to a parenteral opioid may be attempted but is difficult because the dose equivalencies for rotation from methadone to another opioid are not definitively known.8,9 The rectal route may not be feasible for an actively dying patient. For the imminently dying patient who is no longer able to swallow oral methadone, the buccal route of administration may be a more viable alternative. Important advantages of the buccal and sublingual routes of medication administration in palliative care are the noninvasiveness, simplicity, and ease of administration for the patient and the caregiver. 10
Methadone is highly lipophilic and has good bioavailability by the sublingual route.11,12 In one study using healthy volunteers, sublingual methadone absorption was found to be 35% at pH of 3.5 and 75% at pH of 8.5. 12 Results of a feasibility study using sublingual methadone for breakthrough cancer pain in a small number of patients suggested sublingual methadone was effective and well tolerated. 13 Although the sublingual route is often not feasible in the final days of life because of the patient's inability to hold a solution in the sublingual space long enough for absorption to occur, the buccal mucosa is. The buccal mucosa, although less permeable than the sublingual space, may offer an effective site for transmucosal absorption of methadone. The practice on our palliative care unit (PCU) is to use 10 mg/mL methadone solution and limit the volume to 1.5 mL in each buccal space, where the buccal space is defined as the area of the oral cavity between the lower molars and buccal mucosa. Patients need to be able to hold the solution in their mouths for several minutes for transmucosal absorption to occur. For the patient with a low level of consciousness, using the buccal space opposite the lower molars offers a natural pocket where the methadone solution is in prolonged contact with the buccal mucosa without risk of aspiration.
Given the increasingly frequent use of methadone for analgesia in palliative care, more clarity is needed about the use of buccal methadone near end of life. The purpose of this study was to investigate the effectiveness of using buccal methadone in patients established on oral methadone who could no longer swallow at the end of life.
Methods
Participants
The hospital pharmacy database was used to generate a list of patients taking methadone on the PCU between November 2010 and October 2012. Patients taking methadone during this time frame were added consecutively to the case series.
Inclusion criteria included the following:
• Inpatients on the PCU • Presence of a life-limiting illness • Buccal methadone taken after an established course of oral methadone where methadone may have been the primary opioid, an adjuvant opioid, or a combination opioid • Methadone taken for pain
Patients were excluded from the case series if they took methadone for reasons other than pain or if they were discharged from the palliative care unit prior to death. Patients who took oral methadone but were never switched to the buccal route were also excluded.
Procedure
Ethics approval was obtained from the Joint Bridgepoint-WestPark-Toronto Central CCAC-Toronto Grace Research Ethics Board prior to beginning the case series. Health records of patients admitted to the PCU who were either admitted on methadone or rotated to methadone during admission were retrospectively reviewed. Demographic data about participants as well as data regarding methadone use was collected from the health record. The progress notes were reviewed for information about pain management while patients were on methadone. The medication administration records (MARs) were reviewed in each chart to collect information about opioid dose changes and duration of buccal methadone.
When a patient's condition had deteriorated to the point they were no longer able to swallow, oral methadone—whether taken in tablet or solution form—was switched exclusively to methadone solution by the buccal route. Methadone solution was used in a concentration of 10 mg/mL for placement in the buccal space with up to 1.5 mL placed in each buccal space. The cheek was then gently massaged presumably to increase contact with the buccal mucosa. A 1:1 ratio of oral to buccal methadone was used.
Results
Thirty-six patients took methadone on the PCU between November 2010 and October 2012. Eleven were excluded from the case series. The most common reasons for exclusion were transfer to other facilities or home (5), patient being on a feeding tube (2), patient being on oral methadone until time of death (2), or methadone being discontinued (1). Twenty-five patients met criteria for inclusion in the case series. All patients included in the series died on the PCU. Demographic information about the patients is presented in Table 1.
Three of the patients were admitted to the PCU on methadone. The rest were rotated to methadone at various points during their stay on the PCU, varying from the day of admission up to 87 days after admission. Reasons for rotation to methadone are displayed in Figure 1.
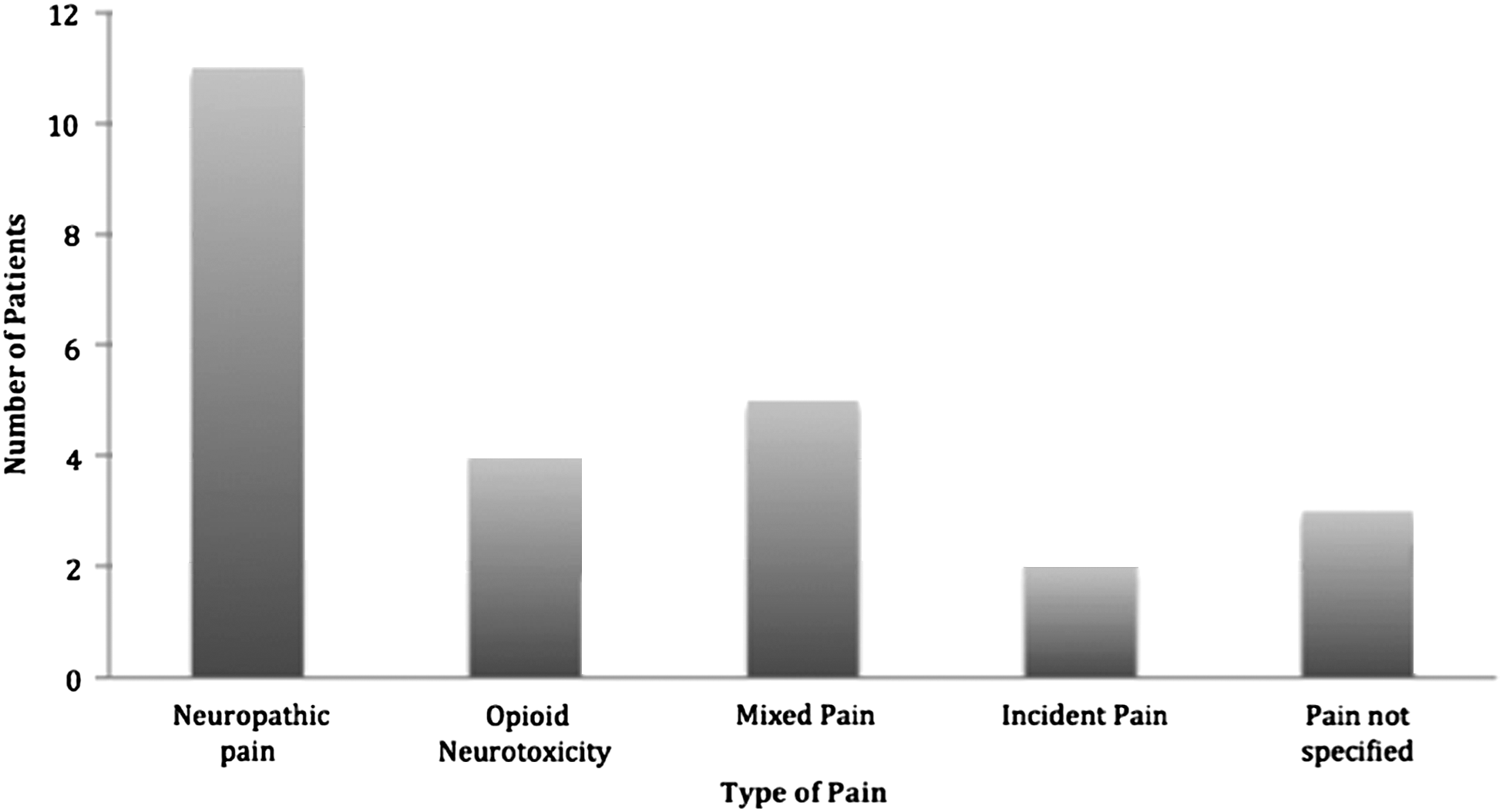
Reasons for rotation to methadone.
Patients received buccal methadone for a median duration of 3 days with use ranging from 1 day to 10 days. Most patients received the buccal methadone either two or three times a day. Methadone was only increased to four times daily if the volume required was greater than 1.5 mL (15 mg) in each buccal space.
The primary outcome measures used in the study were tolerability and effectiveness of buccal methadone. Tolerability was determined by whether or not the patient remained on buccal methadone till the end of life. To determine the effectiveness of buccal methadone in patients unable to communicate at the end of life, the MARs were reviewed for evidence of opioid rotation, opioid dose changes, and use of breakthrough analgesia.
Of 25 cases, buccal methadone was discontinued in one case because of the patient's frequent vomiting. The patient became unable to tolerate anything placed in the oral cavity due to vomiting caused by a bowel obstruction from a gastrointestinal malignancy. Therefore, methadone was rotated to a subcutaneous opioid. No patients had buccal methadone discontinued because of increased pain. The MARs were reviewed for escalation or modification of buccal methadone dose. In one case, the dose of buccal methadone was changed from 40 mg (4 mL) three times per day to 30 mg (3 mL) four times per day to facilitate buccal administration of methadone. In two other cases, the dose of buccal methadone was increased because of ongoing pain at the end of life that had started prior to the patient being placed on buccal methadone. In the remainder of cases, the dose of buccal methadone was unchanged.
The use of breakthrough medication in the last 3 days of life was also reviewed. Twenty-two of the patients used three or fewer breakthrough doses per 24-hours while three used more than three breakthrough doses per 24 hours. Buccal methadone was used for breakthrough pain in 11 patients whereas a parenteral opioid, usually subcutaneous hydromorphone, was used in the remainder of patients.
Discussion
The results of this study indicate that patients tolerate a switch from oral to buccal methadone when they can no longer swallow at the end of life. One advantage of switching oral methadone to the buccal route is that it precludes having to do an opioid rotation near the end of life. Rotation from methadone to another opioid is complicated, lengthy and may result in loss of earlier achieved pain control.8,14
This case series also highlights the ease of switching oral methadone to buccal methadone in patients with low levels of consciousness at the end of life. The practice on our PCU for patients who can no longer swallow is to place up to 1.5 mL of methadone solution in a 10 mg/mL concentration in each buccal space for 2 minutes or more. Although the practice appears to be effective, there is no evidence to support the use of this particular volume of buccal methadone. It is possible a higher volume would be tolerated. However, the primary concern with higher volumes in a patient with diminished level of consciousness near the end of life is the risk of aspiration.
Should a patient require more than 30 mg or 3 mL of methadone per dose for pain control, our practice has been to change the frequency of the methadone, usually from three times daily to four or more times daily with methadone administered at up to 1.5 mL volume in each buccal space. Another option, which we have not tried, would be to instill a higher dose over a longer period of time; for example, 60 mg could be administered in four 15 mg (1.5 mL) aliquots over 10 to 15 minutes. One limitation in using methadone bucally is that it is more difficult to administer at doses higher than 180 mg per 24 hours. In the patient who requires larger doses of methadone near the end of life, it may be necessary to add another opioid or to increase the dose of coanalgesic if the patient is already on another opioid.
Data from this study suggest that pain is managed effectively in the final days of life when methadone is administered by the buccal route. Of the 25 patients who took buccal methadone, 22 (88%) remained on the same dose after the switch from oral, and 22 (88%) required three or fewer breakthroughs per 24 hours. One of the limitations of this case series, however, was that the patients could not directly report on pain control. Because patients at the end of life are often unable to communicate, pain control was inferred through review of health records for evidence of opioid rotation, dose changes or use of breakthrough analgesia. Accuracy of pain assessment cannot be assured in these circumstances and external validity of the series is decreased. Another limitation is the small sample size, which is limited to inpatients on a palliative care unit.
Of interest, however, is that the cases suggest that buccal methadone may represent a simple and effective alternative to further opioid rotation at the end of life for patients already on established oral methadone who can no longer swallow especially when the patient is on relatively low doses of methadone. Further study to describe the characteristics of buccal methadone absorption, particularly the optimal time needed for buccal absorption and the maximal volume tolerated for buccal absorption, would be useful.
Footnotes
Author Disclosure Statement
No competing financial interests exist.