
Abstract
Abstract
Background:
Systemic administration of dexmedetomidine has been shown to reduce opioid consumption and improve analgesia satisfaction. The purpose of this study was to investigate the effect of intrathecal dexmedetomidine on spinal morphine analgesia in patients with refractory cancer pain.
Methods:
A double-blinded crossover study was designed and performed. Patients were randomly allocated in one of the two phases. Phase M received intrathecal morphine administration. Phase M+D received intrathecal morphine plus dexmedetomidine administration. All patients were monitored for 7 days and crossed over to alternate phase for another 1-week observation. Daily average visual analog scale (VAS) pain score, pain frequency, sleep deprivation, daily morphine consumption, bolus dose injection times, and side effects were all recorded.
Results:
Pain intensity and frequency were significantly decreased in both phases compared with baseline. Daily morphine consumption and bolus dose injection times during phase M+D were significantly decreased compared with phase M. The incidences of constipation were significantly reduced in both phases compared with baseline administration, but nausea and vomiting were significantly increased. No serious side effects such as respiratory inhibition were observed in this study.
Conclusions:
Intrathecal administration of dexmedetomidine and morphine reduced the morphine consumption in patients with refractory cancer pain. There were no serious side effects.
Introduction
I
There is a high density of α2-adrenoceptors in the superficial dorsal horn of the spinal cord. 6 Intrathecal and epidural administration of α2-agonist clonidine have been demonstrated to provide analgesia by both presynaptic and postsynaptic mechanisms, 7 and α2-adrenoceptor agonists were also reported to offer specific advantages in neuropathic pain. 8 Recent studies have shown that refractory cancer pain was often combined with neuropathic pain. 9 Therefore, we postulated that intrathecal administration of α2-adrenoceptor agonist with morphine might provide improved effects in patients with refractory cancer pain than intrathecal morphine alone.
Dexmedetomitine, a selective α2-adrenergic receptor agonist, exhibits sympatholytic, sedative, and analgesic effects. It is eight times more potent for the α2-receptor than clonidine. 10 It is widely used in postoperative sedation and analgesia. In previous clinical studies, intravenous dexmedetomidine resulted in a significant opioid-sparing effect as well as a decrease in inhalational anesthetic requirements. 11 Moreover, Gursoy et al. 12 reported that systemic administration of α2-adrenergic receptor agonists (dexmedetomidine or guanfacine) with morphine attenuated the expression of tolerance to the analgesic effect of morphine and enhanced the morphine analgesia in rats. However, administration of intrathecal dexmedetomidine with morphine has not yet been studied. Thus, the purpose of this study was to investigate the effect of intrathecal dexmedetomidine on spinal morphine analgesia in patients with refractory cancer pain.
Methods
Patient selection
Following approval by the ethics committee of the Jinling Hospital and written informed consent, 26 patients with cancer and refractory pain were enrolled in this study.
Inclusion criteria included severe pain (visual analog scale [VAS]>6) with large doses of systemic opioids (converted to oral morphine doses more than 200 mg/d). In addition, patients with severe pain and taking lower doses of morphine due to dose-limiting side effects were included. Exclusion criteria included coagulation dysfunction, atrioventricular block greater than first degree, inability to understand and reliably provide pain assessments, and known hypersensitivity to dexmedetomidine or morphine.
Experimental procedure
The experimental procedure used is shown below (Fig. 1).

Experimental procedure.
Statistical analysis
Results are expressed as the means and standard deviations or numbers and percentages. Differences in the daily morphine consumption and bolus dose injection times between phase M and phase M+D were analyzed by t test. The difference in pain intensity, pain frequency, and sleep deprivation were analyzed by repeated-measures of analysis of variance (ANOVA). Differences between groups were tested by Dunnett's test. The differences in the frequency of side effects between phase M and phase M+D were analyzed by χ2 test. The difference in p<0.05 was considered to be significant.
Results
Patient demographics and baseline characteristics are summarized in Table 1. Two patients were lost to follow-up; a total of 24 patients were studied.
Pain intensity (numeric rating scale) and frequency (4-point verbal ordinal scale) on the day before intrathecal administration (baseline) were 6.9±1.2 and 2.4±0.5, respectively. During phase M, these decreased to 2.8±1.0 (p<0.05) and 0.8±0.4 (p<0.05), respectively, and to 2.4±1.0 (p<0.05) and 0.5±0.5 (p<0.05) during phase M+D, respectively (Fig. 2).
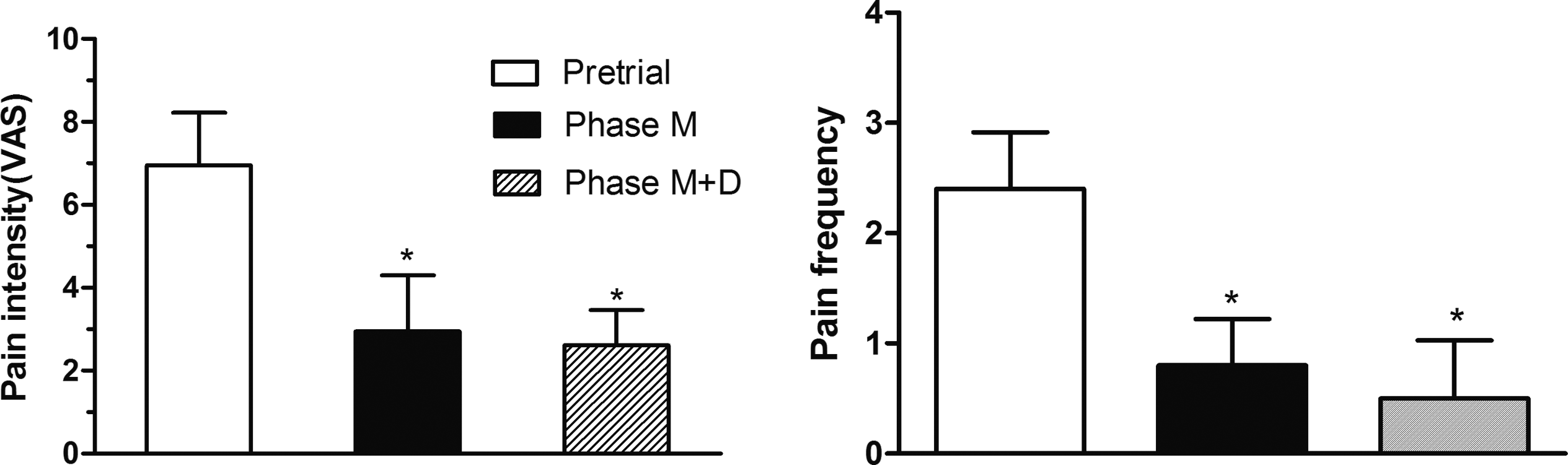
The mean values of pain intensity (visual analog scale [VAS]) and frequency (4-point verbal ordinal scale) on the day before intrathecal administration, during phase M and phase M+D. Value are mean±standard error of the mean [SEM], n=24. Phase M, intrathecal morphine only. Phase M+D, coadministered rated dexmedetomidine with morphine. *p<0.05 vs. before intrathecal administration.
Most of the patients had sleep deprivation before intrathecal administration, with scales (numeric rating scale) averaging 6.8±1.3, which were improved after intrathecal administration to 2.8±1.0 (p<0.05) and 2.4±0.6 (p<0.05) during phase M and phase M+D, respectively (Fig. 3).
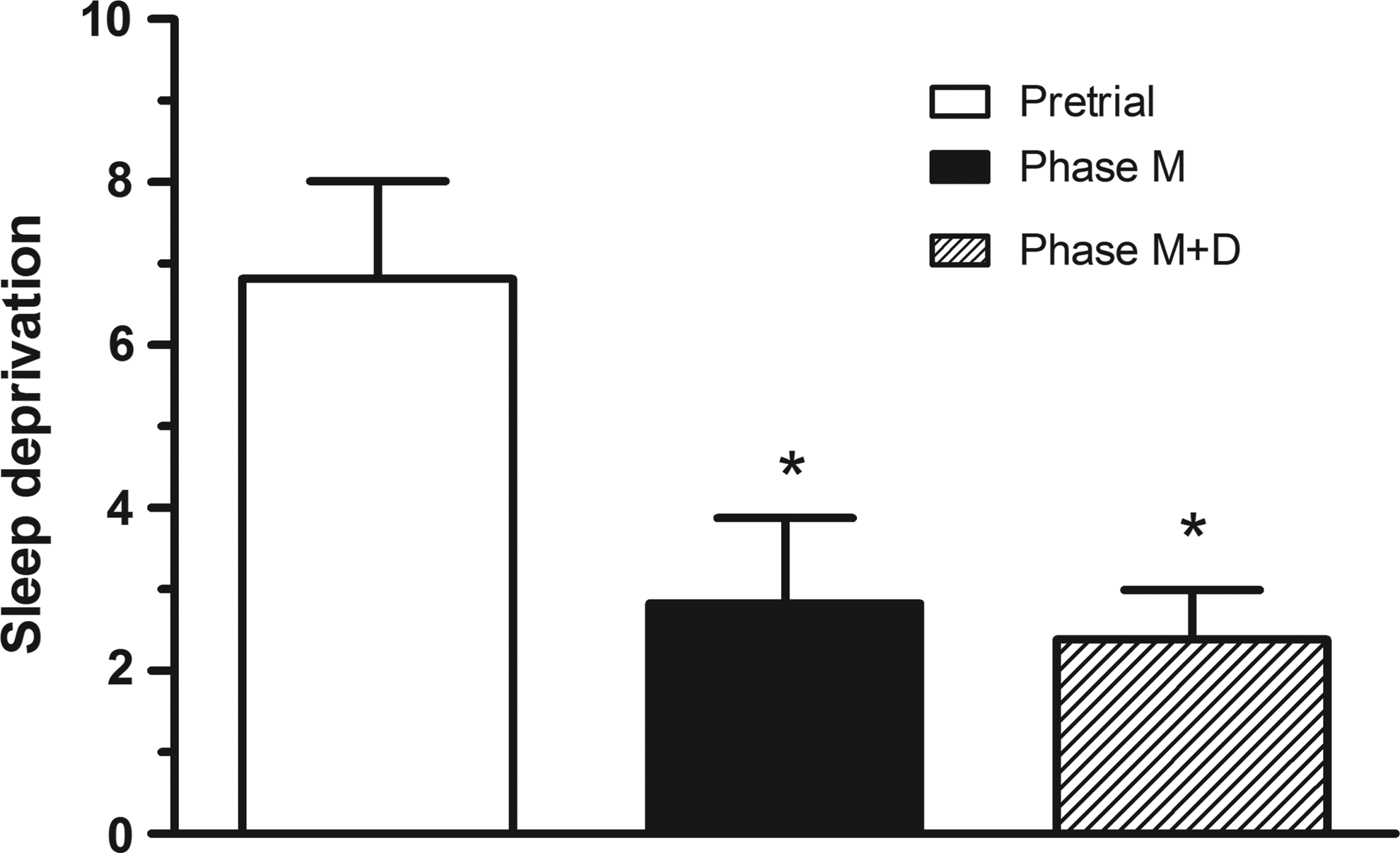
Sleep deprivation on the day before intrathecal administration, during phase M and phase M+D. Value are mean±standard error of the mean (SEM), n=24. Phase M, intrathecal morphine only. Phase M+D, co-administrated dexmedetomidine with morphine. *p<0.05 vs. before intrathecal administration.
Daily morphine consumption and bolus dose injection times during phase M were 7.9±1.1 mg and 6.9±0.9 times, respectively. During phase M+D, they decreased to 5.3±0.8 mg (p<0.05) and 2.8±0.7 times (p<0.05), respectively (Fig. 4).

Daily morphine consumption and bolus dose injection times during phase M and phase M+D. Value are mean±standard error of the mean (SEM), n=24. Phase M, intrathecal morphine only. Phase M+D, coadministered dexmedetomidine with morphine. *p<0.05 vs. phase M.
Side effects were observed and are listed in Table 2. No serious side effects such as respiratory inhibiton, hypotension, or bradycardia were observed at any phase.
p<0.05 vs. pretrial.
Discussion
Our results showed that patients with refractory cancer pain could be greatly relieved by intrathecal morphine alone or morphine plus dexmedetomidine. Furthermore, coadministration of dexmedetomidine with morphine could reduce the intrathecal morphine consumption.
There are two types of drug delivery system for intrathecal analgesia: external catheter and implantable infusion pumps. Because all cases were patients with advanced cancer expected to live 3 to 6 months, and due to economic considerations, an external catheter connected to a computerized ambulatory drug delivery (CADD) pump was used. This regimen was easy to operate and with relative low hospital cost but has risk of possible infection. In the present study, no case of infection was observed, which might be attributed to the small number of patients and short observation.
Several studies about epidural analgesia with intrathecal clonidine have been performed, but few studies on intrathecal dexmedetomidine administration were reported. A previous study indicated that systemic administration of dexmedetomidine with morphine attenuated the expression of tolerance to the analgesic effect of morphine and enhanced the morphine analgesia. 12 Our results revealed that intrathecal administraion of dexmedetomidine with morphine reduced the morphine consumption in patients with refractory cancer pain. The daily intrathecal morphine consumption of phase M+D was significantly reduced than that of phase M. The synergistic effects of morphine and dexmedetomidine could explain this clear benefit on pain control.
Constipation was the most common side effect of opioids. Sixteen patients experienced constipation before intrathecal administration but intrathecal analgesia also produced some adverse reactions. First, nausea and vomiting were the most common adverse reactions, but could be tolerated by most patients after symptomatic treatment. Moreover, the reaction degree will be gradually attenuated with the time of intrathecal analgesia prolonged. Second, urination difficulty was also very common and often occurred in men but seldom in women. Urinary retention was the most troublesome complication and sometimes bladder catheterization was required. One patient developed transient hallucinations during phase M, because a large dose of morphine was required to relieve his pain. Hallucinations disappeared when the morphine dose was reduced during phase M+D. Also, three patients experienced somnolence during phase M and two additional patients experienced it during phase M+D. According to previous studies, dexmedetomidine could provide a unique quality of sedation similar to normal sleep. Under these circumstances, patients could be woken up by verbal stimulation and were able to communicate with the medical staff. The moderate sedation was a benefit for patients.
There were no serious side effects in this study such as life-threatening respiratory depression, hypotension, or bradycardia. The possible explanation might be attributed to the dose of intrathecal morphine was adjusted by titration and overdose was avoided. Although the incidence of some side effects was lower in the phase M+D than in phase M, the difference was not statistically significant, probably because of the small number of patients, brief trial period, and large dose of intrathecal morphine required. Future studies with larger sample size would be needed.
In conclusion, intrathecal administraion of dexmedetomidine with morphine reduced the morphine consumption in patients with refractory cancer pain. No serious side effects were observed. Thus, the concomitant use of intrathecal morphine and dexmedetomidine is an effective and safe method of refractory cancer pain control.
Footnotes
Author Disclosure Statement
No competing financial interests exist.