
Abstract
Abstract
Objectives:
The development of brain metastases is a common cause of morbidity and mortality in cancer patients. Limited life expectancy is well established once a patient requires whole-brain radiotherapy (WBRT). There is emerging evidence demonstrating the value of involving palliative care services alongside traditional treatments. However, data regarding the utilization of these services in patients requiring WBRT remain unexplored.
Methods:
Patients with histologic or radiographic evidence of brain metastases treated with WBRT alone between July 2010 and June 2012 were reviewed retrospectively. Patient demographics, the number of hospital admissions in the last 6 months of life, survival, and referrals to palliative care services were evaluated.
Results:
Ninety-eight patients were diagnosed with brain metastases and treated with WBRT alone. The median overall survival following WBRT was 80 days. Twenty-eight of the patients presented to the emergency department ≥2 times in the last 6 months of life. Sixty-eight percent of patients were referred to palliative care. Of those referrals, 57% were during an inpatient hospitalization. The median survival from palliative care referral to death was 27 days.
Conclusions:
Patients with brain metastasis requiring WBRT have a predictable dying trajectory. These patients are likely to have a high symptom burden and would benefit from palliative care. Timely palliative care referrals in this population remain inadequate and classically follow a hospital admission. Referrals continued to be late in the dying process and the recommendation for WBRT can be used as an independent marker for initiating end-of-life discussions and involving palliative care.
Introduction
B
For the majority of these patients, whole-brain radiation therapy (WBRT) with steroids is the primary treatment approach. 2 Recently, however, the clinical benefits of WBRT have been questioned compared with best supportive care alone. 7 Despite these issues, physicians continue to be optimistic about the clinical efficacy of WBRT and its impact on overall survival. 8
Although accurate prognostication proves challenging for many cancer types, there are certain presentations that carry a predictable dying trajectory.9,10 Patients with inoperable brain metastases requiring WBRT are in this category. The median survival for these patients falls well within the life expectancy recommended for referral to palliative care services.11,12
To date, seven published randomized trials have illustrated the feasibility and benefit of palliative care alongside standard oncology care.13–19 This growing body of literature indicates a better quality of life, better quality of care, decreased cost, improved symptom management, and in some cases improved survival with the addition of palliative care to standard treatment pathways. 20 Given these clear benefits, we investigated the utilization of palliative services in patients requiring WBRT at a major academic center with an accredited fellowship in hospice and palliative medicine and an inpatient hospice unit. To the best of our knowledge, data regarding the use of palliative care services in this population have been unexplored.
Methods
Patient characteristics
All radiotherapy referrals for brain metastases between July 2010 and June 2012 were retrospectively reviewed for inclusion in this study. Any individual who underwent surgical resection or stereotactic radiosurgery was excluded. Therefore, all patients included in this analysis received WBRT alone. Patient gender, performance status, race, degree of social support, histology, number of emergency department or hospital admissions within 6 months of death, and referrals to palliative care (including the referring physician) were evaluated. Palliative care included hospice or palliative care service.
Statistical analysis
Statistical analysis was performed using SPSS software (IBM SPSS Statistics for Windows, version X.0, Armonk, NY, IBM Corp.). Overall survival curves were assessed using the Kaplan-Meier method. The timing patterns and placement of referral were assessed using a k-mean cluster analysis. The final number of clusters was confirmed by clinical meaningfulness. A univariate analysis of palliative care referral was conducted using patient demographic variables. Our primary hypothesis was that referrals to palliative care would be infrequent and delayed despite the recognized poor prognosis of brain metastasis.
Results
Ninety-eight patients at our institution were diagnosed with brain metastasis and treated with WBRT alone in the above date range. Patient and tumor characteristics are seen in Table 1. All histologies were solid malignancies including small cell lung cancer. The largest contributing malignancy was non-small cell lung cancer representing 46% of patients. Melanoma, breast, and small cell lung cancer were the other malignancies contributing greater than 10%. The male to female ratio was 1.25: 1. The median age was 62 years. Responses showed that 80% of individuals were married or had access to social support at the time of clinical encounter. Twenty-eight of the 98 patients presented to the emergency room or were admitted to the hospital for acute care ≥2 times during the last 6 months of life. Eighty-four patients died, 13 were living, and the status of one patient remained unknown at the time of analysis.
RPA, recursive partitioning analysis.
The median overall survival after WBRT for the whole cohort was 2.7 months (80 days) by Kaplan-Meier analysis. Of those who died, the median survival following WBRT was 57 days. A total of 73 patients were classified as RPA Class III with a Karnofsky Performance Status (KPS) score of <70. The proportion of patients in RPA Class I and Class II could not be defined due to incomplete medical records.
Sixty-seven of the 98 patients were referred to palliative care services. After k-mean cluster analysis and evaluation of individual medical records, the referral patterns fell into four major categories (Fig. 1). Six patients were referred to palliative care services more than 3 weeks before WBRT, 6 patients were referred one week prior to WBRT (likely around the diagnosis of widespread central nervous system disease), 30 patients were referred to palliative care within one month of WBRT (typically after a rapid decline following WBRT), and 25 patients were referred to palliative care more than one month after WBRT (typically following a hospital admission). Of the patients referred to palliative care, 57% of the referrals were placed by an inpatient service during an emergency room or hospital admission, 39% were placed by a primary medical oncologist, and 3% were placed by a radiation oncologist (Fig. 2).
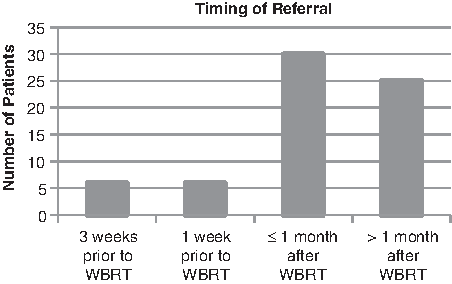
Timing patterns for referral to supportive care services.
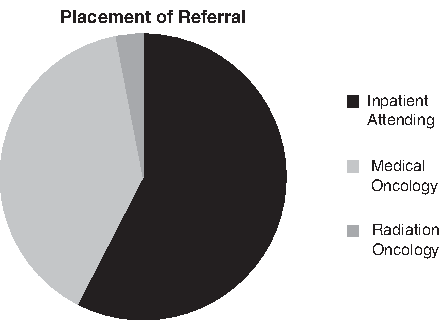
Referring provider for supportive care services.
Referrals to palliative care services appeared to be late in the dying process as the median overall survival after palliative care referral was 27 days (Fig. 3). Fifty-two percent of patients referred to palliative care services died within one month, and 76% died within 2 months. Thirty-two percent of patients were not known to have been referred at the time of analysis. Eleven patients died without referral, 11 remained alive without referral, and the referral status of 9 patients remained unknown.
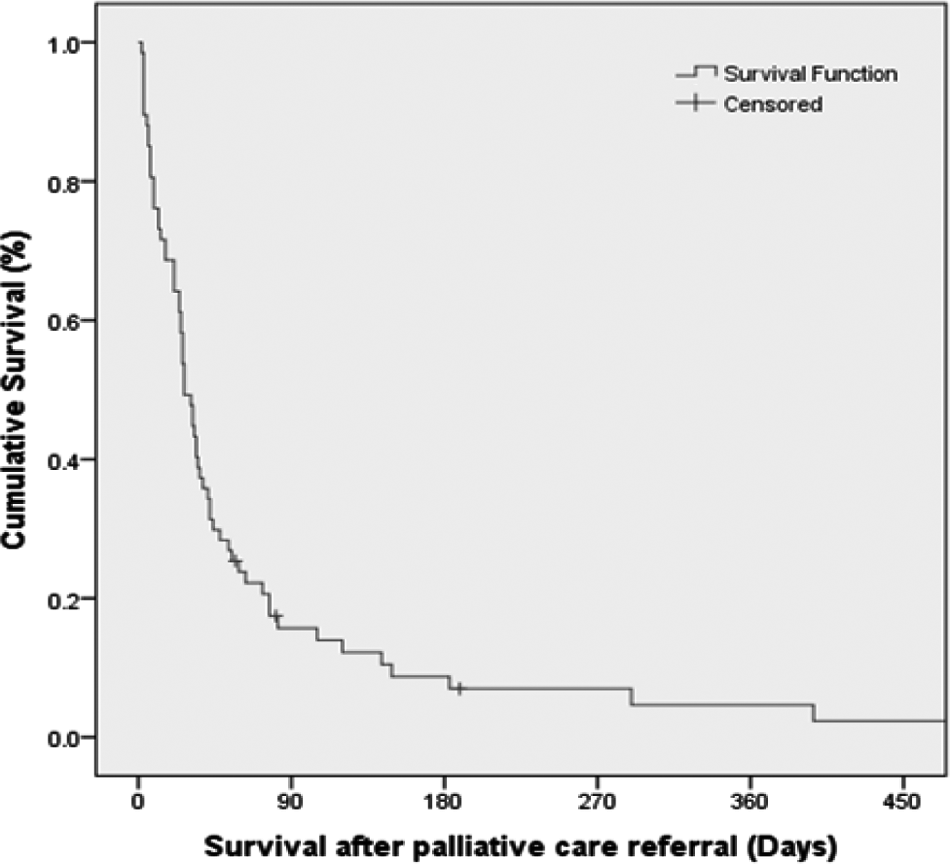
Overall survival following referral to palliative care service.
Discussion
Oncologists are frequently criticized for ineffectively addressing goals of care near the end of life. 21 The heterogeneity of cancer types and their variable presentations limit the ability to predict overall survival. 10 Moreover, goals of care change during a disease course; what a patient hopes for evolves from the time of diagnosis to the time of death. Recognizing the point where further treatment is no longer beneficial and transitioning to a palliative approach is challenging. This requires a comprehensive understanding of the disease process, the dying trajectory, and the expectations of the patient and his or her family. 21
Accurate prognostication remains challenging for most providers; multiple studies have shown physician deficits in predicting the time of death for patients with cancer.9,10,22 The general bias of physicians is to be exorbitantly optimistic by a time factor of two- to fivefold. 23 There are complex psychosocial as well as medical factors that contribute to these findings. That being said, failure to provide timely palliative care may dramatically impact the quality of life in terminal patients by depriving them of needed care. Identifying clear parameters indicative of limited survival may help address these issues. Data would indicate that there are certain clinical presentations where survival outcomes are much more predictable then we realize and patients with inoperable brain metastases requiring WBRT fall into this category.24–26
Both prospective and retrospective data have identified prognostic factors that can assist in this clinical decision-making process for patients with brain metastases. The three-arm RPA from the Radiation Therapy Oncology Group (RTOG) includes age, KPS, primary tumor status, and the presence of extracranial disease. 4 Additionally, the four-arm GPA developed by Sperduto and colleagues incorporates the number of brain metastases and a more defined account of extracranial disease. 3 The results of these and other prognostic studies show a median survival that falls between 2 and 7 months, with a small subset of patients (including those with breast and renal cell primaries) that can live beyond a year.3–6
Predictive factors for survival include good performance status, age <65 years, primary tumor control, lack of extracranial metastases, favorable tumor histology, and the presence of a solitary brain metastases.3–6 For patients with good risk features, resection and/or stereotactic radiosurgery are the current modalities of choice; WBRT is utilized predominantly in poor risk patients with multiple brain metastases. The very indication for WBRT remains a poor prognostic sign and survival approximates 2 months.11,12 These patients are likely to have a high burden of symptoms requiring palliative services.
The potential benefits of WBRT include improvement or stabilization of neurological symptoms, improved quality of life, improved performance status, and a reduction in steroids use. 25 In light of these potential benefits, there is strong evidence that physicians overestimate the true clinical advantages of WBRT and misjudge patient survival by 1.9 months. 8 This overly optimistic attitude may contribute to delayed palliative care referrals.
The potential toxicities from WBRT include nausea, vomiting, fatigue, weakness, and neurocognitive decline. These may be unnecessary and burdensome for patients who will not live long enough to see the benefits. 27 Recently, these considerations have led to the activation of a prospective randomized trial comparing best supportive care versus WBRT. 7
Though much attention has been placed on the significance of prognostic modeling, there is limited literature examining patterns of care following WBRT. In our series the median survival following WBRT was 80 days and 74% of our patients were RPA Class III. Only 68% of our patients were referred to palliative care services at the time of this analysis, and more than half of those referrals were placed by an inpatient attending during an admission for uncontrolled symptoms. Although it was clear that these patients had a poor prognosis, palliative care referrals remained late in the dying process, considering current guidelines recommend a referral when life expectancy is less than 6 months. 20 In our series the median survival from the time of palliative care referral was 27 days.
Although our cohort was small, univariate analysis failed to demonstrate any demographic variable associated with the timing of palliative care referral. These results are consistent with a larger study that showed no difference in hospice referral based on race, religion, gender, or income. 28 The indication for WBRT alone was the best prognostic indicator for limited life expectancy.
The 2012 consensus statement by the American Society for Clinical Oncology (ASCO) encourages integration of palliative care services with standard oncology practices. 20 This statement is in response to the growing body of evidence that indicates a better quality of life, better quality of care, improved symptom management, and in some cases improved survival with the addition of palliative care to standard treatment pathways. 20
Several randomized trials have illustrated the feasibility of providing palliative care services alongside standard oncology care. Overall, the addition of these services proves beneficial and no harm has ever been seen.13–19 Unfortunately, current health care policies and reimbursement schemes limit early and effective implementation of palliative care.29,30 Furthermore, the scarcity of clinicians trained in palliative care requires a selective approach, which targets patients with high symptom burden and short survival.
As we continue to navigate through the ever-changing medical climate, identifying patients who clearly have a limited survival and an increased need for symptom management is a sensible starting point for involving palliative care. Formalizing specific criteria (such as the requirement of WBRT) is an easy way to implement palliative care services. But, even with ideal referral strategies and resource utilization, providing these services to all patients with brain metastases would be challenging. Newer delivery strategies such as multidisciplinary supportive care conferences and patient/provider educational systems should be explored.
In a recent prospective study by Abernethy and co-workers, patients who were discussed at a single supportive care case conference experienced fewer hospitalizations and maintained a better performance status compared with the control group. 31 In our analysis, 28 of 98 patients presented to the emergency department at least twice during the last 6 months of life. Although dying patients inevitably experience increased symptoms and, therefore, incur increased costs, the use of supportive care conferences to identify such patients may prevent unnecessary hospital admissions and decrease the overall cost of care. 32
Currently, radiation therapy remains the primary treatment modality for brain metastases, yet radiation oncologists placed only 3% of palliative care referrals in this series. Whereas most radiation oncologists perceive themselves as part of the palliative team, less than 10% of palliative care professionals feel the same. 33 Ironically, 30% to 50% of radiation treatments are delivered with palliative intent. 34
Radiation oncologists have unique insight and experience in evaluating and providing treatment recommendations for patients who have developed brain metastases. This is a heterogeneous patient population, and these insights are imperative in personalizing treatment recommendations. A typical 2-week treatment course offers the opportunity to comprehensively assess the patient's needs. This includes not only primary intervention with radiation treatments, but also help with symptom management and working with patients and their families to align goals of care to prognosis. Radiation oncologists are often involved during this critical time in a patient's disease course, and the recommendation for WBRT can be a driver for palliative care referral. This is beneficial for the patient and the family, and it allows radiation oncologists to remain active members of the multidisciplinary team. The failure to do so could delay an important component of end-of-life care.
Going forward, several important questions remain. What should the role of the consulting physician be in end-of life-care? Which physician should be having these conversations and be placing the referral to palliative care? How do patients perceive consulting physicians in end-of life-care and how should palliative care physicians balance the multiple treatment recommendations from consulting physicians as they try to align goals of care with the patient?
This study has several limitations. First, it is single institutional and retrospective in nature. At our institution, surgical resection and/or stereotactic radiosurgery are preferred for patients with a limited number of brain metastases. Therefore, patients who received WBRT alone either had a large burden of intracranial disease or were poor surgical candidates. This may have contributed to the limited overall survival in our series. In addition, RPA classification could not be completed for all patients, and this may have biased the timing of palliative care referral. As a final point, one must consider the availability of palliative care services at an institution. Our center maintains an accredited fellowship in hospice and palliative medicine in addition to an inpatient hospice unit and consultation service. These services certainly influence the referral patterns and percent utilization.
Conclusions
The evidence for early integration of palliative care services into standard oncology practice continues to grow. There are objective data indicating a limited life expectancy for patients receiving WBRT; however, timely referrals to palliative care services remain delayed. The common pattern of care at our institution was completion of WBRT followed by a symptomatic hospital admission leading to palliative care referral by an inpatient service. Despite their extensive clinical experience and treatment of these patients, radiation oncologists were rarely involved in the referral process. Radiation oncology should be more proactive in patient care issues at the end of life, and the recommendation for WBRT should prompt a strong consideration for palliative care.
Footnotes
Author Disclosure Statement
No competing financial interests exist.