
Abstract
Abstract
Background:
Dignity therapy is a brief psychotherapy developed for patients living with a life-limiting illness.
Objective:
To determine the influence of dignity therapy on depression and anxiety in inpatients with a terminal illness and experiencing a high level of distress in a palliative care unit.
Methods:
A nonblinded phase II randomized controlled trial of 80 patients who were randomly assigned to one of two groups: intervention group (dignity therapy+standard palliative care [SPC]) or control group (SPC alone). The main outcomes were depression and anxiety scores, as measured with the Hospital Anxiety and Depression Scale, and assessed at baseline (T1), day 4 (T2), day 15 (T3), and day 30 (T4) of follow-up. This study is registered with www.controlled-trials.com/ISRCTN34354086.
Results:
Of the final 80 participants, 41 were randomly assigned to SPC and 39 to dignity therapy. Baseline characteristics were similar between the two groups. Dignity therapy was associated with a decrease in depression scores (median, 95% confidence interval [CI]: −4.00, −6.00 to −2.00, p<0.0001; −4.00, −7.00 to −1.00, p=0.010; −5.00, −8.00 to −1.00, p=0.043, for T2, T3, and T4, respectively). Dignity therapy was similarly associated with a decrease in anxiety scores (median, 95% CI: −3.00, −5.00 to −1.00, p<0.0001; −4.00, −7.00 to −2.00, p=0.001; −4.00, −7.00 to −1.00, p=0.013, for T2, T3, and T4, respectively).
Conclusion:
Dignity therapy resulted in a beneficial effect on depression and anxiety symptoms in end-of-life care. The therapeutic benefit of dignity therapy was sustained over a 30-day period. Having established its efficacy, future trials of dignity therapy may now begin, comparing it with other psychotherapeutic approaches within the context of terminal illness.
Introduction
I
The clinical consequences of both depression and anxiety are well known. Depression, for example, is a recognized risk factor for suicide and requests to hasten death, 7 disrupting social connections and diminishing individual's capacity to overcome loss and difficulties associated with incurable diseases. 2 Anxiety can markedly interfere with patients' lives as an independent psychiatric disorder or as an amplifier in association with certain physical symptoms, such as pain or dyspnea, thus rendering their control more difficult.
Psychological suffering for terminally ill patients is also often framed in terms of loss of dignity. 8 The empirical work by Chochinov and colleagues 9 regarding the concept of dignity in terminally ill patients created the Model of Dignity offering important insights as to how patients face terminal illness in terms of their dignity. This model provides the theoretical basis for a brief, individualized intervention designed to address psychosocial and existential distress among terminally ill patients (dignity therapy). 10
The most recent trial by Chochinov and coworkers, 11 designed to compare dignity therapy with standard palliative care and client-centered care, showed that although dignity therapy did not significantly reduce distress, those assigned to dignity therapy were significantly more likely than other study groups to find this approach helpful, to improve quality of life, increase sense of dignity, change how their family saw and appreciated them, and be helpful to their family. In this study, dignity therapy did not show any effect on patients' symptoms of depression and anxiety, but the authors stated that this apparent lack of effect might have been due to the low initial base rates of distress. For this reason, future investigation using dignity therapy should target more distressed patients, with symptoms of depression and anxiety. Portuguese cancer populations have been shown to have high levels of depression and anxiety. 12 For this reason, we conducted a randomized controlled trial (RCT) of Portuguese terminally ill patients hospitalized within an inpatient palliative medicine unit, with high levels of psychological suffering at baseline, to study the efficacy of dignity therapy on symptoms of depression and anxiety. The preliminary results of this RCT (interim analysis, n=60 patients) have been published elsewhere. 13
This article reports the efficacy data for dignity therapy on symptoms of depression and anxiety within a cohort of 80 patients with end-stage cancer.
Methods
We conducted a phase II nonblinded RCT comprising two study arms: an intervention group, consisting of dignity therapy in addition to standard palliative care (SPC), and a control group, consisting of SPC alone. Given the nature of the study design, it was not possible for the investigators or patients to be blinded to the study arm assignment.
Depression and anxiety symptoms were assessed using the Hospital Anxiety and Depression Scale (HADS) at baseline, day 4, day 15, and day 30 post-dignity therapy, as per the study protocol (Table 1).
DT, dignity therapy; HADS, Hospital Anxiety and Depression Scale; SPC, standard palliative care.
Our study is registered with www.controlled-trials.com/ISRCTN34354086.
Participants
Recruitment took place from S. Bento Menni's 10-bed tertiary inpatient palliative medicine unit in Lisbon. Recruitment took place over 36 months (May 2010 through May 2013).
We used the following inclusion criteria: 18 or more years of age; having a life-threatening disease with a prognosis of 6 months or less; no evidence of dementia or delirium, determined by chart review or clinical consensus of the palliative care team; Mini Mental State score 20 or more; ability to read and speak Portuguese; ability to provide written informed consent; and availability for 4 to 5 research encounters over a period of 1 month.
Our study received ethical approval from the Ethics Committee of the Instituto das Irmãs Hospitaleiras do Sagrado Coração de Jesus-Casa de Saúde da Idanha.
Randomization and masking
The randomization process was computer generated, using a fixed block of four, and was conducted by an independent statistician. Allocation concealment was achieved using sequentially numbered envelopes for consecutive trial participants. After baseline measures were obtained by the secondary investigator (F.O.), the envelope was opened in the presence of the patient to reveal the study arm to which the patient was assigned. While the principal investigator (M.J.) was not blinded to patients' arm assignment, he was blinded to the psychometric results throughout the entire protocol. The secondary investigator was blinded to the content of dignity therapy sessions.
Interventions
Standard palliative care
Standard palliative care was provided by a multiprofessional palliative care team, comprising three palliative medicine physicians (one of whom was M.J.), nurses, a psychologist social worker, and spiritual assistant, thus providing the capacity for all patient- and family-related physical, existential, and psychosocial needs to be addressed. Clinical care included regular clinical follow-up: physical examination, symptom assessment and management, and clinical interviews (median, 25 minutes; range, 10–30 minutes). Meanwhile, standard palliative care was provided for all patients throughout the entire hospital stay, including the period of time they were enrolled within the RCT. Aside from the provision of dignity therapy, participants randomly assigned to the standard care arm received regular assessment and management by the entire multiprofessional team. Other than the principal and secondary investigators, the remainder of the palliative care team were not informed as to which patients were enrolled in the study or whether or not they received dignity therapy. This reduced any potential for bias or alteration of care based on knowledge of arm assignment. The principal and secondary investigators had limited clinical contact with patients, given the former works 1 day per week in the palliative care ward and the latter is the chief nurse and has little direct patient contact.
Dignity therapy
Dignity therapy is a brief psychotherapeutic approach with the aim of bolstering the patient's sense of meaning and purpose, reinforcing a continued sense of worth within a framework that is supportive, nurturing, and accessible for those near death. Patients enrolled in dignity therapy are asked to audio-record aspects of their lives they would most want their loved ones to know about or remember. Dignity therapy offers patients the opportunity to talk about issues that matter the most to them, to share moments that they feel were the most important and meaningful, to speak to things they would like to be remembered by, or offer advice to their family and friends. These recorded sessions provide the basis of an edited transcript, entitled a generativity document, which is returned to patients for them to share with individuals of their choosing. Creating this document is meant to make patients feel valued and that something of themselves will last beyond death.
Therapeutic sessions, running between 30 and 60 minutes, were offered at patients' bedsides and audio-recorded. Every tape-recorded session was erased after the completion of the study protocol. This study utilized the dignity therapy question framework, 10 as per previously published trials (Table 2). All dignity therapy sessions were completed by the principal investigator (M.J.), who attended an international dignity therapy workshop held in Winnipeg, Canada, hosted by the developers of dignity therapy; all procedures for dignity therapy were conducted in accordance with those described and published by Chochinov et al.10,14 A third-party—a senior psychiatrist (A.B.)—acquainted with dignity therapy vetted randomly selected dignity therapy transcripts, to monitor fidelity and protocol adherence.
Patients meeting eligibility criteria and agreeing to participate in the study were asked to provide written informed consent. Once patients completed the baseline assessment (T1), those randomly assigned to dignity therapy were provided with the standard framework of questions, thus giving them time to reflect and shape their eventual responses (Table 1). The taped dignity therapy session was scheduled to take place within 2 to 3 days. The therapeutic session was entirely guided by the dignity therapy framework. Once the taped session was complete, over the course of the next 2 to 3 days, the patient's recorded dialogue was transcribed verbatim and then edited (as per the dignity therapy protocol/manual) and reshaped into a written narrative. Once this editing process was complete, another session was arranged as soon as possible, for the therapist to read the document to the patient, allowing for final editorial corrections and revisions. The final version of the generativity document was given to the patient, to be distributed to the individuals of their choosing.
Outcomes
Primary outcomes were symptoms of depression and anxiety, measured with HADS, at baseline (T1), day 4 (T2), on day 15 (T3), and day 30 (T4) of follow-up (Table 1).
Statistical analysis
Based on previously published Portuguese studies of the HADS in cancer populations, 12 we considered a mean reduction of 1.5 points on the HADS depression subscale to be clinically significant. Assuming a type I error of 5%, a power of 80%, and a standard deviation of 2.5, each study arm required at least 45 patients. Assuming a dropout rate of 10%, we intended to include in the overall study 50 patients in each group. Our study protocol included two interim analyses: the first after 60 participants 13 and another after 80 participants were obtained. In the final interim analysis, the mean reduction was superior to 1.5 points on the HADS depression subscale (Table 3) and therefore the trials were closed; this report includes data gathered until study closure in May 2013.
Wilcoxon test.
Mann-Whitney test.
CI, confidence interval; DT, dignity therapy; HADS, Hospital Anxiety and Depression Scale;
Evaluation time points: T2=post-intervention; T3=day 15; T4=day 30.
We compared continuous variables and ordinal rating scales using nonparametric statistical tests, Mann-Whitney test was used for independent group comparison (dignity therapy versus SPC) and Wilcoxon test for paired comparisons, between each time measure (T2, T3, and T4) and baseline, within each study group. To measure the effect, median differences (paired and unpaired) were used, and the respective 95% confidence interval, using the method proposed by and Altman 14 and Royston. 15
The criterion for statistical significance was set at p<0.05 in a two-tailed test. The statistical analysis was applied to all the patients who had at least one complete evaluation at any given follow-up point (T2, T3, T4, as per protocol analysis).
Results
Summary demographic and illness data for both groups are presented in Table 4. There were no differences between the two groups regarding the baseline characteristics. Over a 36-month period, 150 patients were admitted into the palliative care unit ward; 92 patients were assessed for eligibility, 80 of whom were randomized (39 to dignity therapy and 41 to SPC; Fig. 1). After randomization, one patient died before receiving dignity therapy and another presented severe clinical deterioration; 10 patients were lost to follow-up (as a result of death, clinical deterioration, or declining further participation) at T2 (dignity therapy: n=6; SPC: n=4); 18 patients were lost to follow-up at T3 (dignity therapy: n=9; SPC: n=9) and 14 patients at T4 (dignity therapy: n=5; SPC: n=9; Fig. 1).
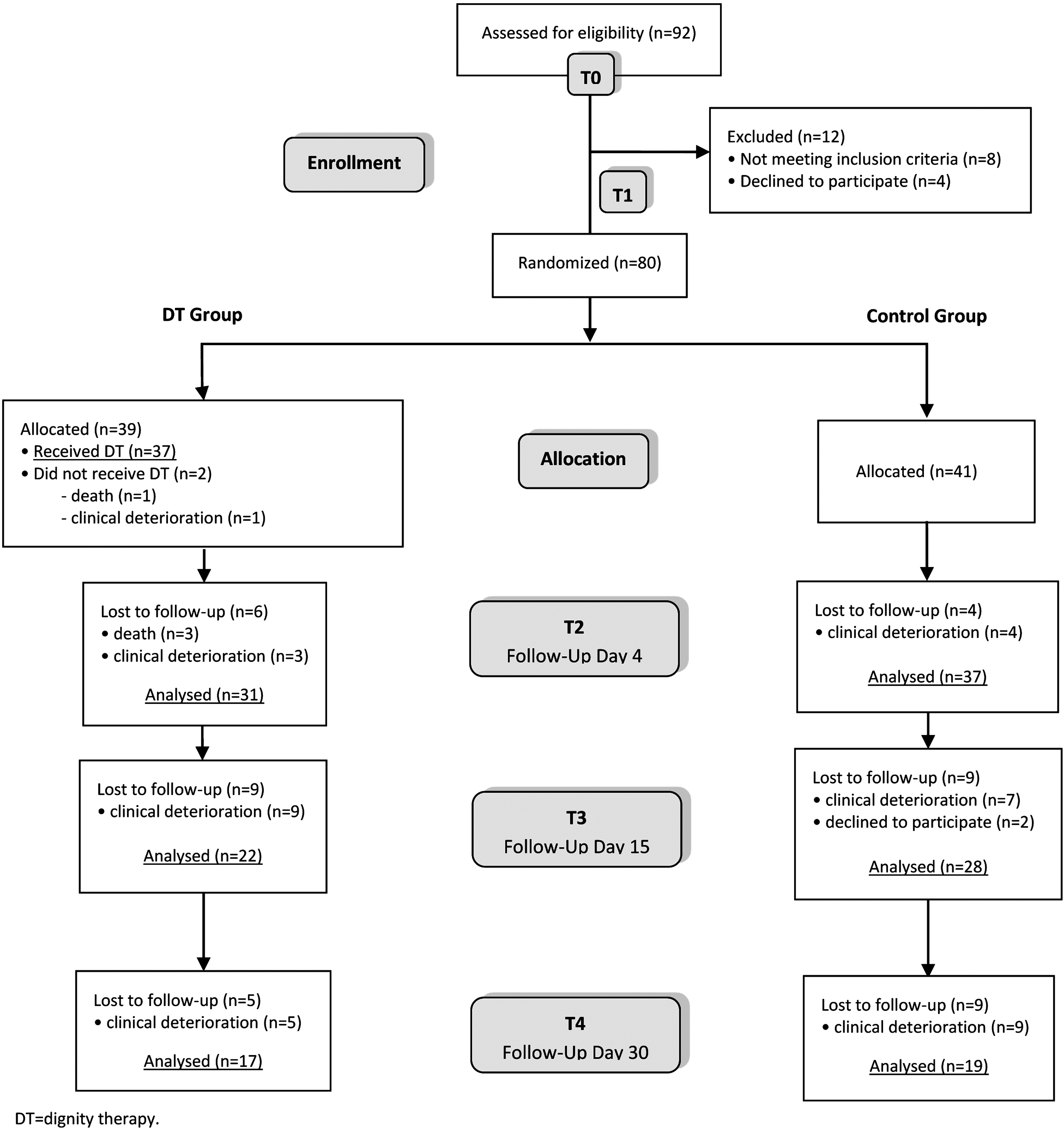
CONSORT diagram. DT, dignity therapy.
Fisher's exact test.
Lung, n=14; breast, n=6; ovarian, n=6; glioblastoma, n=4; uterus, n=4; bladder, n=3; endometrium, n=3; stomach, n=3; tongue, n=3; prostate, n=3; rectum, n=3; unknown primary cancer, n=2; esophagus, n=2; melanoma, n=2; caecum, n=2; larynx, n=2; biliary tract, n=1; colon, n=1; glioma, n=1; dorsal neurinoma, n=1; chronic myeloid leukemia, n=1; linfoid leucemia, n=1; multiple myeloma, n=1; neoplasm of the nose, n=1; pancreas, n=1; small bowel neuroendocrine tumor, n=1; urethra, n=1; vascular arterial cancer, n=1.
Lateral amyotrophicsclerosis, n=2; trigeminal neuralgia, n=1.
Based on medical records or patients information.
Palliative Performance Scale: 100%=healthy; 0%=death.
DT, dignity therapy. HADS-a, Hospital Anxiety and Depression Scale–Anxiety Subscale; HADS-d, Hospital Anxiety and Depression Scale–Depression Subscale; SD, standard deviation; CI, confidence interval.
The mean survival time was 25.4 days (dignity therapy=27.4, SPC=26.8; p=0.453).
Depression
Both groups had a mean (standard deviation [SD]) score on the HADS depression subscale exceeding 11 at baseline (SPC: 13.20 [3.91]; dignity therapy: 12.87 [4.79]; p=0.741). Table 5 shows median (interquartile range [IQR]) scores on the HADS depression subscale at all assessment periods.
HADS-a, Hospital Anxiety and Depression Scale–Anxiety Sub-scale; HADS-d, Hospital Anxiety and Depression Scale–Depression Subscale; RCT, randomized controlled trial; SPC, standard palliative care; IQR, inter quartile range; DT, dignity therapy.
Evaluation time points: T2=postintervention; T3=day 15; T4=day 30.
In patients assigned to dignity therapy a significant decrease on depression ratings on day 4 and day 30 (median=−3.00; 95% CI, −5.00 to −1.50, p=0.001; median=−1.00; 95% CI, −4.00 to 2.00, p=0.001, respectively) was observed, but not on day 15 (median=−2.25; 95% CI, −5.00 to 0.50, p=0.100; Table 3).
Within the SPC group, there was a significant increase in depression ratings between baseline and all assessment periods (median=1.50; 95% CI, 0 to 2.50, p=0.045; median=2.50; 95% CI, 1.0 to 3.50, p=0.004; median=3.00; 95% CI, 1.50 to 5.00, p=0.006, respectively; Table 3).
Compared with the SPC group, those receiving dignity therapy demonstrated significantly less depression at all assessment periods (median=−4.00; 95% CI, −6.00 to −2.00, p<0.0001; median=−4.00; 95% CI, −7.00 to −1.00, p=0.010; median=−5.00; 95% CI, −8.00 to −1.00; p=0.043, respectively; Table 3).
Anxiety
Both groups had a mean (SD) score on the HADS anxiety subscale less than 11 at baseline (SPC: 8.88 [4.36]; dignity therapy: 9.67 [4.77]; p=0.442). Table 4 shows median (IQR) scores on the HADS anxiety subscale at all assessment periods.
Compared to the SPC group, those receiving dignity therapy demonstrated significantly lower anxiety ratings at all assessment periods (median=−3.00; 95% CI, −5.00 to −1.00, p<0.0001; median=−4.00; 95% CI, −7.00 to −2.00, p=0.001; median=−4.00; 95% CI, −7.00 to −1.00, p=0.013, respectively; Table 6).
Wilcoxon test.
Mann-Whitney test.
HADS, Hospital Anxiety and Depression Scale; DT, dignity therapy; CI, confidence interval.
Evaluation time points: T2=postintervention; T3=day 15; T4=day 30.
Within the dignity therapy group, there was a significant reduction on anxiety ratings between baseline at all assessment periods (median=−4.00; 95% CI, −5.50 to −2.50, p<0.0001; median=−5.50; 95% CI, −7.50 to −3.00, p=0.001; median=−4.50; 95% CI, −8.00 to −2.00, p=0.003, respectively; Table 6).
In the SPC group, there was an increase on the HADS anxiety subscale between baseline and all assessment periods, although not statistically significant, (median=0.50; 95% CI, −0.50 to 1.50, p=0.536; median=1.00; 95% CI, −1.00 to 3.50, p=0.325; median=0.50; 95% CI, −2.50 to 5.00, p=0.637, respectively; Table 6).
Discussion
As previously demonstrated in the Portuguese population with cancer 12 and in our previous interim analysis, 13 our study sample experienced high levels of depression and anxiety at baseline. The levels were notably higher than those reported by Chochinov et al. 11 Comparatively, the mean sample scores for HADS depression were 13.2 versus 5.86 and HADS anxiety were 8.88 versus 5.22, respectively. Our findings suggest that dignity therapy can be offered to eligible participants, even those with more severe psychological distress at baseline. Although Chochinov 16 has cautioned that patients with marked depression may be at risk of creating a distorted version of themselves through dignity therapy, there was no evidence to suggest this in our study.
In our previous interim report, 13 dignity therapy appeared to have a short-term benefit on the psychological distress encountered by patients near the end of life: patients who received dignity therapy were significantly more likely than SPC patients to experience reductions on depression ratings, immediately posttreatment, with improvement being sustained throughout subsequent follow-up, with the exception of the day 30 evaluation. The present study, using a larger patient sample, shows that participants receiving dignity therapy experience a significant reduction in symptoms of depression, and were in fact less depressed at every time point compared with the control group. As such, it appears that a single dignity therapy session seems to have a sustained effect that can be seen at 30 days postintervention. This probably indicates that using dignity therapy to help the patient articulate memories, speak about their past, and share important reflections has benefits that are sustain well beyond the intervention itself. Providing them the opportunity to create a personal generativity document engages the patient in a vital role, which likely diminishes their sense of helplessness and despair.
Our present findings regarding dignity therapy's ability to mitigate anxiety symptoms at all assessment periods corroborate those in our previous interim report. 13 One can only speculate on the causal linkage between dignity therapy and the reduction of anxiety. Perhaps dignity therapy enables patients to address existential issues, such as unfinished business, manifesting as a reduction of anxiety. It remains of interest that this positive effect was sustained well beyond the time of therapeutic engagement.
There are several limitations to this study. Our patients sample primarily comprised older patients. As such, the influence of dignity therapy within younger cohorts remains to be established. Despite a relatively small sample size, we were able to detect significant differences between and within-group, indicative of clinically meaningful improvement. The majority of the study participants had end-stage malignancies. Our future research will explore the utility of dignity therapy for other terminal conditions, such as end-stage organ diseases. Within this trial, dignity therapy was performed exclusively by one therapist (M.J.), who carefully followed the dignity therapy protocol 16 and was trained by the originators of this therapeutic approach. While he was not blinded to the study arm assignment, thus generating the potential for bias, patients in both groups received equal quality palliative care (SPC) and all evaluations, treatment plans, and direct interventions were carried out, as per unit protocol, by the entire multidisciplinary team. Finally, we recognize that since neither group study was blinded, a remote but yet possible placebo or nocebo effect might be present in the findings.
Based on our findings, dignity therapy resulted in a sustained beneficial effect on psychological distress encountered by patients near the end of life. These results are important in shaping the future role of dignity therapy within palliative care research initiatives and the structure of clinical care programs. The stage is now set to test dignity therapy, within randomized control trials, comparing its performance against other approaches aimed to mitigate significant end-of-life distress.
Footnotes
Acknowledgments
M.J. and A.B. were responsible for the conception and design. M.J. was responsible for supervising the study, analyzing the data, and writing the initial draft and final report. F.O. was responsible for the scale assessments. B.N. supervised the data statistical analysis. A.V.C. helped with the revising of the final report. All coauthors helped revise the final manuscript and had full access to all of the data.
We are grateful to each and every patient who participated in our study. Without their commitment, effort, and generosity, in spite of any physical or psychological suffering they may have been experiencing, this study would not have been possible. We would like to thank: Filipa Fareleira, Vivelinda Guerreiro, Sofia Mata, Carlos Centeno, Peter Lawlor, Todd Weeks. We are grateful to the palliative care team of the Palliative Medicine Unit of S. Bento Menni. A special word of gratitude to Professor Chochinov for his unwavering guidance and wisdom.
A word of gratitude in the memory of Isabel Levy for the research scholarship of Associação Portuguesa de Cuidados Paliativos.
Author Disclosure Statement
No competing financial interests exist.