
Abstract

Introduction
Palliative Care for Older Adults
Palliative care for elders differs from what is usually appropriate in younger adults because of the nature and duration of chronic illness during old age. The prototypical example of a palliative care patient is that of a 55-year-old mother of two with advanced ovarian cancer. Care for this patient would include chemotherapy until it no longer meets the patient's goals of care; treating her symptoms (e.g., nausea, pain, fatigue); addressing her psychological and spiritual concerns; supporting her partner; and helping to arrange for care of her children after her death. The majority of this patient's care occurs at home (with or without hospice) or in the hospital, and the period of functional debility is brief (months). In reality, a frail 88-year-old widowed woman with advanced heart failure, diabetes mellitus, osteoarthritis, mild cognitive impairment, and frailty typifies the most common example of a patient requiring palliative care. Palliative care for this patient involves treating the primary disease process (advanced heart failure); managing her multiple chronic medical conditions and comorbidities (diabetes mellitus, arthritis) and geriatric syndromes (cognitive impairment, frailty); assessing and treating the physical and psychological symptom distress associated with all of these medical issues; and establishing goals of care and treatment plans in the setting of an unpredictable prognosis. Additionally, the needs of her caregiver(s) are also different from those of the caregiver of the younger patient. Individuals caring for geriatric patients are often adult children with their own families, work responsibilities, and medical conditions. These roles must be balanced with the months to years of personal care that they will provide to their aging parent. Finally, because older adults often make multiple transitions across care settings (home, hospital, rehabilitation, long-term care), especially in the last months of life, palliative care programs for older adults must assure that care plans and patient goals are maintained from one setting to another. Thus, palliative care for the elderly is centered on the identification and amelioration of functional and cognitive impairment; the development of frailty leading to dependence on caregivers; symptom, emotional, and spiritual distress; and bereavement needs of adult children and elderly partners. The overlap between the traditional fields of geriatrics and palliative care is shown in Figure 1.
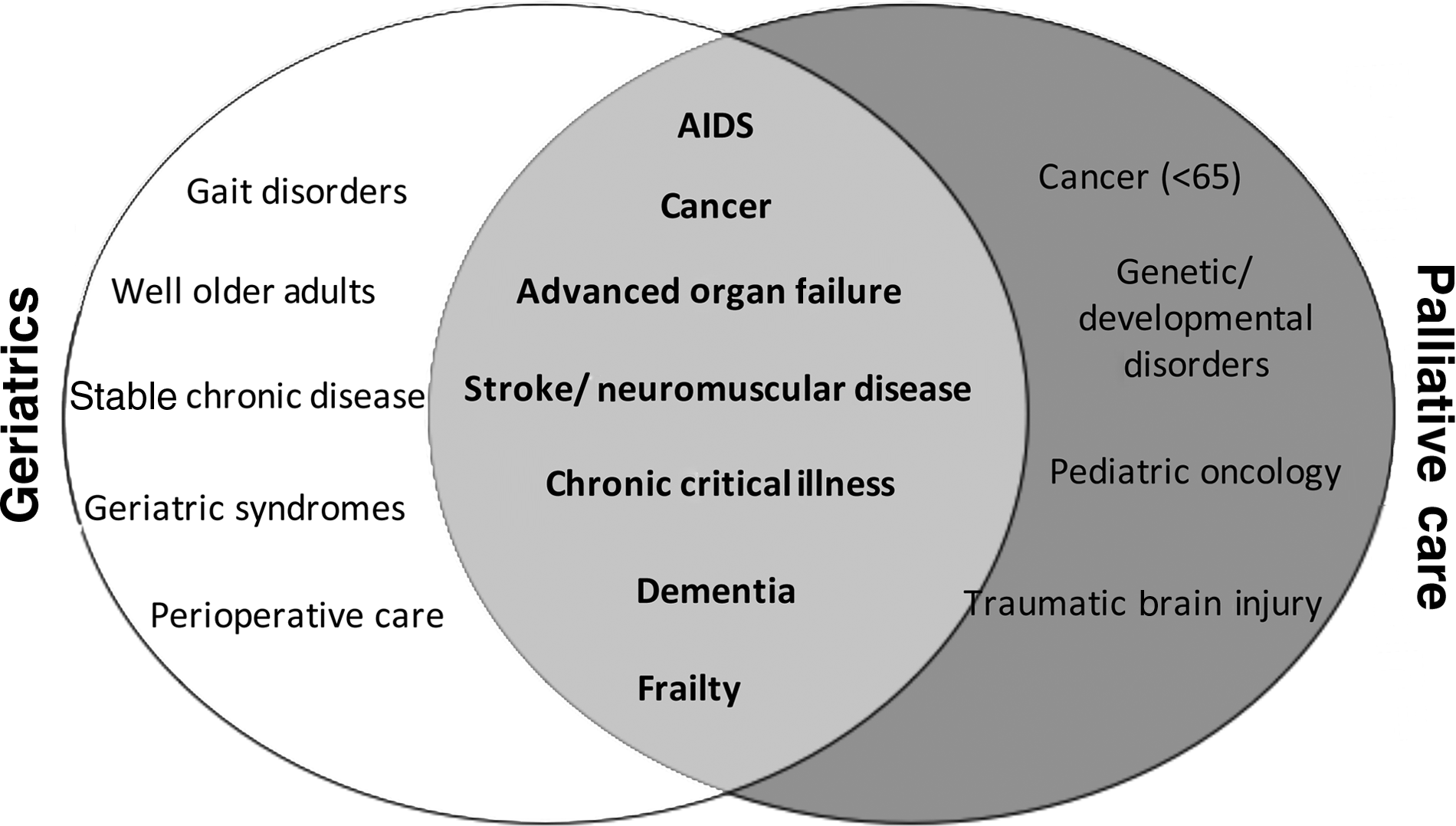
The intersection between geriatrics and palliative care.
The Knowledge Base of Palliative Care for Older Adults
Although death occurs far more commonly in the elderly than in any other age group, the evidence base for palliative care in older adults is sparse. 7 For example, the majority of symptom prevalence studies have focused on patients with cancer and AIDS, have not included the oldest old, have excluded patients with associated comorbidities, or have focused almost exclusively on pain. The incidence and prevalence of pain in older populations is unknown. Studies have suggested that the prevalence of significant pain in community-dwelling older adults may be as high as 56% 8 and that almost one-fifth of older adults take analgesic medications on a regular basis. 9 Similarly, it has been suggested that 45%–80% of nursing home residents have substantial pain and that many of these patients have multiple pain complaints and multiple potential sources of pain. 10 Available data also point to a high prevalence of nonpain symptoms in older adults with serious and chronic illness. In retrospective interviews with family members of patients who died of noncancer illnesses in the United Kingdom, 67% of patients experienced moderate to severe pain, 49% had trouble breathing, 27% reported nausea, 36% reported depression, and 36% reported sleep disturbances. 11 In an analysis of patients with heart failure, end-stage liver disease, lung cancer, and COPD from the SUPPORT trial, over 20% of patients consistently experienced severe dyspnea during the six months prior to death.12–14 A companion study to SUPPORT reported almost identical pain findings for a cohort of hospitalized patients 80 years and older 15 and also noted a high prevalence of anxiety and depression in the last six months of life. 16
Preliminary studies suggest pain and other symptoms are underassessed, undertreated, and are associated with a number of negative outcomes in older adults. 17 Pain is perhaps the best studied symptom, and data from several studies suggest that untreated pain is associated with depression, decreased socialization, sleep disturbance, impaired ambulation, and increased health care utilization in older adults. 18 These studies are limited by small sample sizes, have included relatively healthy subjects with defined conditions (e.g., osteoarthritis), have focused on postoperative surgical patients, or have been confined to one disease state (e.g., cancer). Additionally, they have not included frail older adults nor adults with multiple comorbidities and have not examined the association of pain with outcomes such as gait disturbances, rehabilitation and functional recovery, frailty, and functional dependence. 18 Studies in older adults that have included these outcomes (functional recovery, frailty, falls, and function) have typically not included pain and other symptoms as independent variables.19–21 Studies on the prevalence, assessment, and association of other symptoms (e.g., dyspnea, anxiety, nausea, fatigue) on quality of life, function, and other outcomes are largely lacking.
The evidence base for the effective management of pain and other symptoms in older adults is also sparse. Although the American Geriatrics Society published guidelines for the treatment of acute and persistent pain, these guidelines were largely based upon small cohort studies and expert opinion. 22 Recommendations for age-adjusted dosing are not available for most analgesics, 18 and almost all analgesics have side effect profiles that are particularly problematic in older adults. 22 Interventions directed at other symptoms (e.g., dyspnea, nausea, anxiety) have rarely included older adults or have focused on relatively narrow conditions (e.g., chemotherapy induced nausea), and the results are difficult to generalize to older adults with advanced illness and multiple comorbidities. 7 Even studies in younger adults have rarely linked the treatment of pain to outcomes other than symptom relief. Although many have argued that patient comfort should be sufficient stimulus to alter pain management practices,1,23,24 the documented difficulties in shifting clinician priorities and behaviors 25 suggest that empirical data regarding the adverse effects of pain and other symptoms on clinical outcomes are required to change practice patterns and improve patient care.
Moreover, the burdens of serious illness extend to patients' families and friends.4,5,26 More than 50 million individuals are relied on as informal caregivers 27 due to recent efforts to reduce hospitalization rates and lengths of stay. The majority of these people are older adults who endure stress and burden related to both caring for the individual in the setting of serious illness and in coping with their death. An increasing body of research demonstrates adverse financial, physical, and psychological effects on them. For example, a study recently reported that over one-third of 893 caregivers had substantial stress; and 86% stated that they needed more help with transportation (62%), homemaking (55%), nursing (28%), or personal care (26%) than they were currently receiving or could afford. 5 Caregivers with care needs were significantly more likely to consider suicide, have depressive symptoms, and to report that caring for patients interfered with their lives and reduced their independence. 4 Caregiving has also been shown to be an independent risk factor for death, major depression, and associated comorbidities. 28
What Is Needed?
An adequate evidence base for palliative care for older adults will require new knowledge; creation of innovative models of care delivery; the development of new research instruments, designs, and analytic techniques; and the application of established instruments, designs, and techniques from other fields to palliative care and aging research. Traditionally, research in pain and other symptoms has relied upon patient self-report as the gold standard of assessment. 29 For patients with cognitive impairment, such assessment may be impractical or simply impossible, and reliable means of assessing pain and other symptoms through behavioral observation or through the use of proxies are required. Unfortunately, existing observational scales 30 require considerable skill, experience, and familiarity with the patient to administer; and validated scales employing proxy respondents are not available. 18 Researchers also face complexities in studying patients with multiple symptoms that may interact with each other—particularly since it may be difficult to distinguish symptoms caused by the patient's illness from those resulting from treatments. Such patients require instruments that assess a wide constellation of symptoms and multiple dimensions within each individual symptom. A few such instruments exist, however, they are relatively complex, lengthy, burdensome, and have not been validated in older adults.31–34 Indeed, in a population-based study of adults with recently diagnosed rectal cancer, subjects who were older, had poor performance status, or were receiving active palliative care were significantly more likely to have missing data on physical functioning and on global quality of life than younger and more highly functional patients over the two-year study. 35 Although some research questions in geriatric palliative care may be addressed using the gold standard of clinical research—the randomized controlled trial—many others may only be feasibly addressed through observational data and quasi-experimental designs. Thus, improvements in care require careful and innovative use of nonrandomized and sometimes uncontrolled settings. 1
Finally, specific analytic issues unique to palliative care in older adults also require attention. For example, the problem of missing or distorted data is considerable in palliative care research. 1 Data is often missing because patients with advanced disease die during studies or are unable to report directly about their symptoms, concerns, or attitudes due to their illness, treatment, or both have left them confused, weak, or unconscious. Sophisticated research methods to deal with nonrandom missing data are required in palliative care research but are not yet widely used. Many studies in palliative care are observational or employ quasi-experimental designs and thus require analytic techniques that strengthen the inferences made from the studies.
Addressing the Knowledge Gap
In summary, there is a pressing need to improve the evidence base for palliative care in older adults. The areas of research that need to be addressed include establishing the prevalence of symptoms in patients with chronic disease; evaluating the association between symptom treatment and outcomes; increasing the evidence base for symptom treatment; understanding patients' psychological/spiritual well-being and quality of life goals; and elucidating sources of caregiver burden, reevaluating service delivery, and adapting research methodologies specifically for palliative care. Although great strides were made in outlining the need for improving palliative care at the 2004 NIH State of the Science Conference on Improving End-of-Life Care, 36 even at this landmark event there was a focus on terminal disease and not on expanding the idea of palliative care to include improving the quality of care of older patients with multiple chronic illnesses. In an effort to address this gap in research and develop the knowledge that clinicians need to appropriately care for older adults with serious illness, 15 research experts in aging and palliative care research gathered in Bethesda, Maryland, on January 31, 2013 at a meeting co-sponsored by the National Palliative Care Research Center, the National Institute on Aging (NIA), and the Icahn School of Medicine at Mount Sinai Claude D. Pepper Older Adult Independence Center. The purpose of the meeting was to examine the state of the science in geriatric palliative care, identify research priorities that could, if addressed, lead to improved palliative care in older adults, and identify studies needed to fill gaps. Over the next six months, the Journal will be publishing a series comprising the proceedings of this conference entitled “Research Priorities in Geriatric Palliative Care.” The topics that will be addressed include the epidemiology of serious illness; research methods; multimorbidity; nonpain symptoms; informal caregiving; establishing goals, values, and preferences; long-term care; disparities; and policy initiatives. The topics of research priorities for pain in older adults 37 and care for persons with end-stage dementia 38 are not included in this series, as comprehensive papers addressing these topics have been recently published. It is our hope that this series will help to develop a template that will guide research and funding priorities in palliative care for older adults.
Footnotes
Acknowledgments
This work was supported by the NIA, Claude D. Pepper Older Americans Independence Center at the Icahn School of Medicine at Mount Sinai [5P30AG028741], and the National Palliative Care Research Center. Dr. Morrison is the recipient of a Midcareer Investigator Award in Patient-Oriented Research (5K24AG022345-10).