
Abstract
Abstract
Background:
For parents of a critically ill infant, good communication may help alleviate stress and anxiety. To improve communication, physicians must be responsive to families' needs and values surrounding the care of their hospitalized infant.
Objective:
We adapted a Decision-Making Tool for the Neonatal Intensive Care Unit (N-DMT) to encourage consideration of family concerns and preferences in daily care planning.
Design:
This was a randomized controlled design.
Setting/Subjects:
Parents and providers of critically ill neonates were eligible. Parents were randomized to an intervention group (using the N-DMT) or standard of care. N-DMT information was shared through the electronic medical record and communicated directly to the primary provider.
Results:
Complete data were obtained on 10 control and 9 intervention families. Groups did not differ on demographics or mean infant Score of Neonatal Acute Physiology (SNAP) scores (36 versus 37). FIN-PED scores were similar for both groups. The control group showed decreased anxiety over time. The content of rounds did not differ between groups. The intervention group reported lower satisfaction with care, specifically in questions regarding communication.
Conclusions:
In this pilot study, we found that families in the intervention group were less satisfied with communication. Families who are primed to expect better communication, such as those participating in a communication intervention, may be less satisfied with standard care.
Introduction
P
Providers' efforts to provide emotional and informational support is critical to parents' ability to cope with the anxiety associated with having an infant in intensive care.5,6 Although much communication occurs during rounds, there are few descriptive studies of NICU rounds.
This exploratory study was designed to contribute to this area by describing the communication content of NICU rounds and conducting a randomized study using a NICU adaptation of the Seattle Palliative Care Group's Decision Making Tool (DMT). 7 We expected that sharing information from the DMT would increase discussion of family concerns and preferences on rounds, where multiple, high-stakes decisions are made. We hoped to encourage consideration of family concerns and preferences in daily care planning and improve family-centered communication, thereby decreasing parental anxiety and increasing satisfaction with NICU care.
Methods
Parents of infants admitted to a tertiary care NICU were eligible for the study if their infant was less than 8 days old, had an expected length of stay of more than 14 days, a Score of Neonatal Acute Physiology (SNAP) 8 greater than 20 (high risk for morbidity and mortality), and spoke English. Parents were excluded if any provider caring for the infant refused to participate in the study. Eligible providers included NICU physicians, nurse practitioners, respiratory therapists and nurses. The project was approved by the Institutional Review Board with written informed consent.
The DMT was adapted for use as an interview tool. Questions addressed four main areas including: (1) medical indications for treatment (“Give a brief description of your baby's condition”); (2) parent preferences (“How do you like things explained to you?”); (3) quality of life (“What goals and hopes do you have for your baby's life?”); and (4) contextual issues (“How do your cultural or spiritual beliefs impact how you make decisions?”). The goal was to encourage parents to articulate needs and values that could be relevant to medical decision-making.
A randomized, controlled design was used. In the intervention group, parents were interviewed using the NICU-adapted DMT (N-DMT). Information obtained was placed in the electronic medical record (EMR) and communicated to the primary NICU provider via email. For controls the content of a recent social work note was communicated with the primary provider via e-mail, creating an attentional control group. Daily rounds on all infants were audio-recorded for 3 consecutive days after enrollment to see if information from the N-DMT was incorporated into daily care planning.
Parents in both groups were surveyed at study entry and 2 weeks later. At both times, parents completed the State component of the State-Trait Anxiety Inventory (STAI) to establish and control for parental anxiety and evaluate for impact of the N-DMT on anxiety. The second survey included the Family Inventory of Needs–Pediatrics (FIN-PED) survey, 9 and an N-DMT–specific survey, with items such as “My baby's doctors considered my goals and hopes for my baby during decision-making” and “My baby's doctors considered my family's spiritual well-being.” Items were scored on a Likert scale, 1–4, strongly agree to strongly disagree. The total N-DMT score could range from 8–32. Principal component analysis extracted one scale with a Cronbach α of 0.92.
Recordings were analyzed via the Roter Interaction Analysis System (RIAS), a quantitative tool for assessing content and quality of patient-physician communication. 10 Data were coded to understand if and how providers used information from the N-DMT in daily care planning (Table 1). Because rounds for each infant was recorded more than once, analytic methods were used to account for the repeated measures where appropriate. Demographic and survey data were analyzed via nonparametric tests; multiple linear regression analysis was used to identify independent predictors of anxiety and satisfaction with care.
RIAS, Roter Interaction Analysis System; CPAP, continuous positive airway pressure.
Results
Of eligible families, 25 of 37 were approached during the week of birth when study personnel were available; 20 consented to participate. Complete data were obtained for all participants except 1 intervention family who did not complete follow-up surveys. Daily rounds were recorded successfully 55 of 57 times and analyzed via RIAS. A total of 183 of 190 providers consented to participate.
There were no significant demographic differences between groups (Table 2). There were no differences in the content of rounds between groups (Table 3). Psychosocial exchange was infrequent (1.3% versus 1.4% of all talk; intervention versus control groups). Medical talk was the most frequent (65% versus 62%).
All continuous variables are reported as median (range); all categorical variables as number (percent).
SNAP, Score for Neonatal Acute Physiology; NICU, neonatal intensive care.
Data presented as medians.
N-DMT, Decision-Making Tool for the Neonatal Intensive Care Unit (N-DMT).
The duration and the relative contribution of parents to rounds were not significantly different between groups (Table 4). However, there was decreased psychosocial discussion by the presenting provider on rounds when parents were present (1.6% versus 0.4%; p=0.04). This was true for both groups. The proportion of psychosocial discussion by the attending (p=0.53) and other providers (p=0.19) did not change.
Data are presented as medians (range).
For rounds where parents were present (n=10).
N-DMT, Decision-Making Tool for the Neonatal Intensive Care Unit (N-DMT).
Both groups showed high anxiety, indicated by scores greater than 40 on the STAI. 11 Unlike the intervention group, the control group showed a decrease in anxiety over time. Scores for both groups at the 2-week follow-up were similar (45.3 intervention versus 46.3 controls; Table 5). Anxiety scores were not related to gestational age, birth weight or SNAP scores.
STAI, State-Trait Anxiety Inventory; possible scores range from 20–-80, with higher scores indicating greater anxiety.
CI, confidence interval.
There were no differences between intervention and control groups for all but one question on the FIN-PED. For the question, “I needed to know what treatment my baby was receiving,” the intervention group was less satisfied compared to the controls (mean of 4 versus 3.33; range, 0 to 4, “not met” to “completely met,” p=0.013).
There was no significant difference in satisfaction with care as measured by the N-DMT scale between the intervention and control groups (median [range]: 26 [15–28] versus 28.8 [19–32]), in a univariable model or multiple variable model controlling for gestational age. There was, however, a pattern of decreased satisfaction with care among the intervention group compared to the control group across the N-DMT-specific survey questions, although the differences were not statistically significant (Fig. 1).
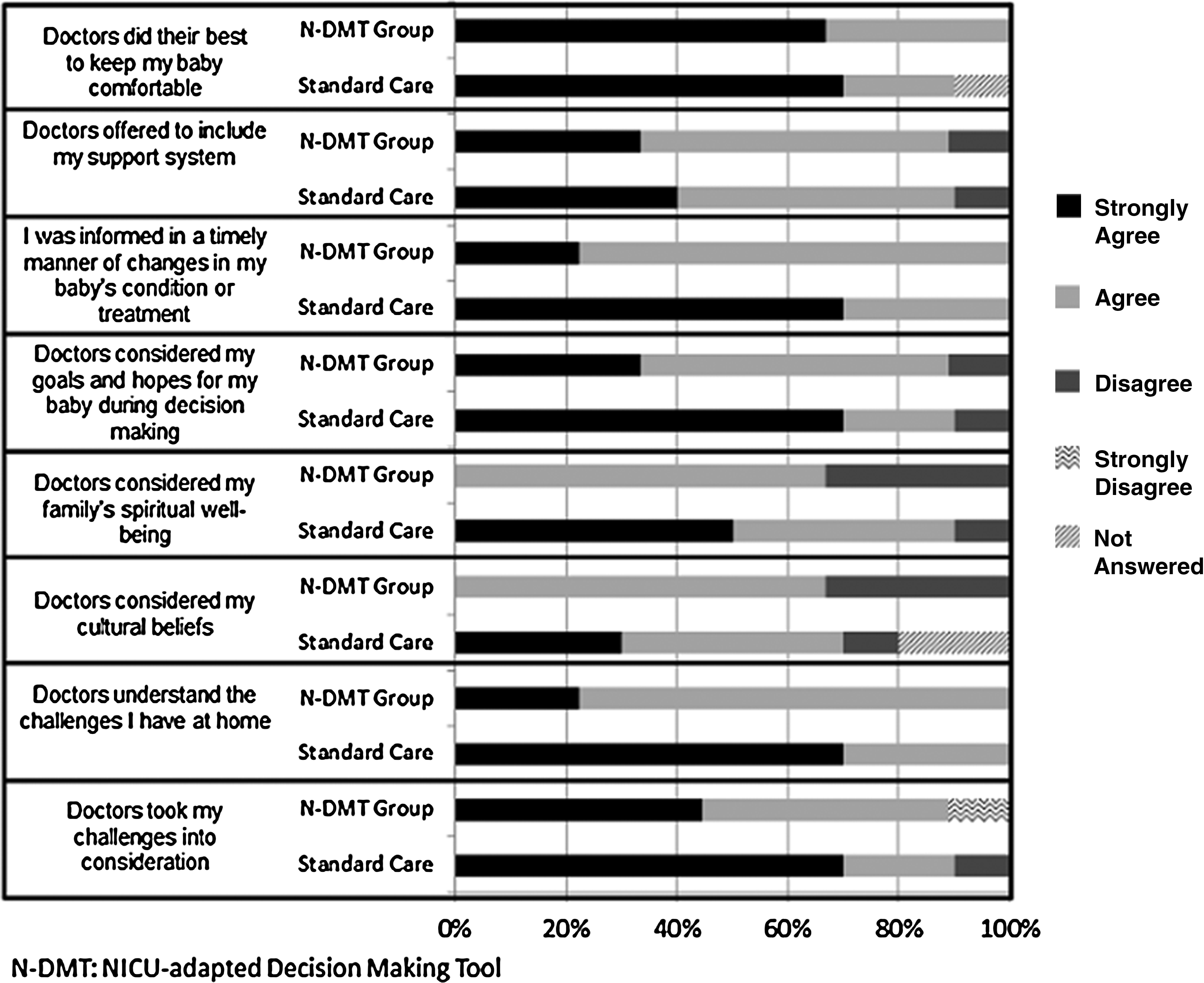
N-DMT–specific survey questions. N-DMT, NICU-adapted Decision-Making Tool.
Discussion
Our study is among the first to describe the communication content of NICU rounds. We examined the extent to which an N-DMT affected the communication process.
Despite the exploratory nature of the study, we have established a proof of concept: both providers and parents agreed to recordings of NICU rounds and recordings can be reliably analyzed. We found that the proportion of psychosocial and emotional communication during NICU rounds was negligible. We were surprised by this, given the high levels of parental anxiety and evidence that both emotional and informational communication is valued by parents. 6
When compared to standard NICU care, the N-DMT neither increased discussion of parent concerns during daily rounds nor reduced parental anxiety. Moreover, we found that parents in the intervention group were less satisfied with care. The original DMT was effective at increasing discussion of parental concerns during family meetings. 7 With our adaptation, parental concerns were relayed to providers in written form; there was no requirement that those concerns be addressed. Even when parents attended, the total amount of family-centered discussion on rounds did not change significantly. However, the amount of psychosocial discussion by the presenting provider was significantly less, perhaps reflecting an assumption that parents will voice their own concerns.
Larger studies have shown that even with dedicated effort to improve communication, it is difficult to change provider behavior. 12 One solution might be incorporating a question regarding family needs into a rounds checklist, as has been effective in improving communication about other aspects of ICU care. 13
The control group showed decreased anxiety over time; the intervention group was unchanged. We did not find that anxiety was related to gestational age, birth weight, or SNAP score, but we did not investigate the relationship to infant recovery from illness. Baseline anxiety of parents was not explored and may have contributed to differences in anxiety.
Families who received the N-DMT were less satisfied with communication than were controls. This held true after controlling for infant characteristics. Satisfaction may be more related to the fulfillment of expectations concerning communication than to the medical care received.14–16 Curtis et al. 17 noted no increase in communication satisfaction and slightly increased depressive symptoms of patients after a communication intervention. After participating in the N-DMT interview, parents may have been primed to expect increased communication from providers specific to their concerns and were less satisfied when they did not receive it.
Although this pilot study determined that it is feasible to incorporate the N-DMT into a busy NICU environment, it did not result in increased family-centered communication during rounds. Researchers should be mindful that family expectations may change after involvement in studies concerning communication, possibly resulting in negative unintended consequences.
Footnotes
Acknowledgments
We thank the Seattle Palliative Care Group for allowing us to modify their Decision Making Tool and Dr. Hays for his insightful discussion regarding this project.
Author Disclosure Statement
No competing financial interests exist.