
Abstract
Abstract
Objective:
The aim was to achieve endoscopic debulking surgery with regional low-dose radiotherapy as an alternative to tracheostomy for the management of metastatic endoluminal laryngeal tumor.
Background
: Endometrial adenocarcinoma rarely metastasizes to the head and neck region. Laryngeal metastases from endometrial adenocarcinoma are even rarer and usually indicate widespread disease. We present the case of a 55-year-old Asian woman with endometrial adenocarcinoma. She received radical surgical treatment and postoperative radiotherapy in April 2009. Fifteen months later, a solitary pulmonary lingual lobe metastasis was found and lobectomy was performed. The patient had hemoptysis another 15 months later, and a laryngeal endoluminal tumor was found by bronchoscopic examination. To prevent upper airway compromise, we performed transoral endoscopic debulking surgery with postoperative regional low-dose radiotherapy, instead of traditional tracheostomy. The patient underwent palliative chemotherapy after the surgery. After the intervention, the patient lived 19 months without upper airway obstruction.
Discussion
: According to the literature reviewed, this is the first case of endometrial adenocarcinoma with metastasis to the larynx. We here present this unique case and provide a less invasive treatment for upper airway obstruction. Without a tracheostoma, the patient's quality of life was greatly improved. Moreover, there was a reduced risk of lower airway infection.
Conclusions:
We suggest endoscopic debulking surgery with regional low-dose radiotherapy as an alternative to tracheostomy for the management of metastatic endoluminal laryngeal tumors.
Introduction
E
Because hematolymphatic drainage is sparse in the larynx, metastatic laryngeal tumors are extremely rare and represent only 0.09%–0.40% of all laryngeal tumors. 3 They usually occur in the late stage of disease and cause upper airway obstruction. Patients may be kept away from their daily activities, and their quality of life is negatively affected. Restoration of the patient's quality of life is the main goal of the management of such conditions.
Laryngeal metastases arise most commonly from cutaneous melanoma and renal cell carcinoma, followed by lung, prostate, colon, stomach, and ovarian cancers. 3 The English-language literature reviewed in this work reported no case of endometrial adenocarcinoma with laryngeal metastasis. We here present a case of laryngeal metastatic endometrial adenocarcinoma and discuss its metastatic routes and the management of the upper airway.
Case Presentation
A 55-year-old gravida 4, para 4 woman (height 155 cm; weight 58.8 kg) had undergone radical hysterectomy, bilateral salpingo-oophorectomy, and bilateral pelvic lymph node dissection in April 2009. Pathology showed endometrial adenocarcinoma with right parametrium metastasis, pT3bN0M0, stage IIIa. Histology revealed mixed-type adenocarcinoma of the uterus including endometrioid, serous, and clear cell carcinoma. Postoperative adjuvant chemoradiotherapy (CRT) had also been performed. Fifteen months later, in July 2010, a solitary pulmonary tumor located in the lingual lobe was found, and she then received lingual lobectomy. Pathology showed metastatic adenocarcinoma from the endometrium.
She presented at our outpatient clinic in October 2011 with symptoms of strider and hemoptysis. A subglottic laryngeal tumor (see Fig. 1) was noted on flexible laryngoscopy. An endoluminal tumor was located in the cricoid area, with 30% airway obstruction (see Fig. 2) demonstrated on computed tomography (CT).
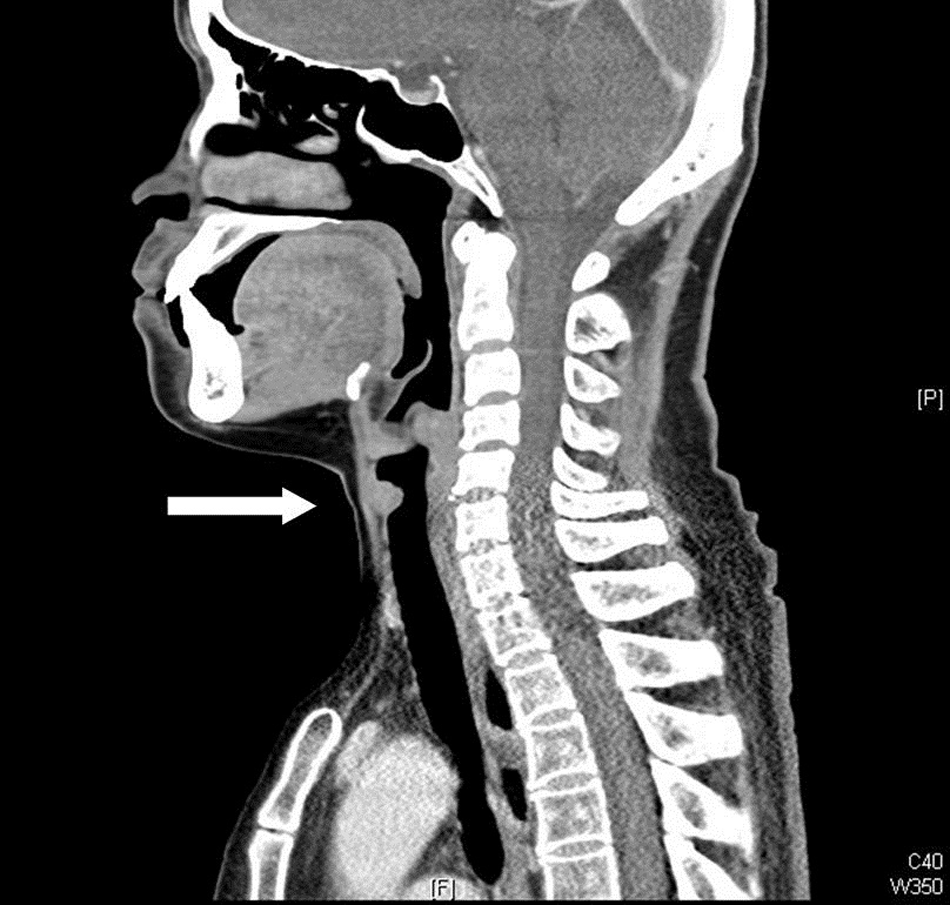
A nodular mass about 1*1.2 cm on the anterior wall of larynx (about 1 cm below the vocal folds).
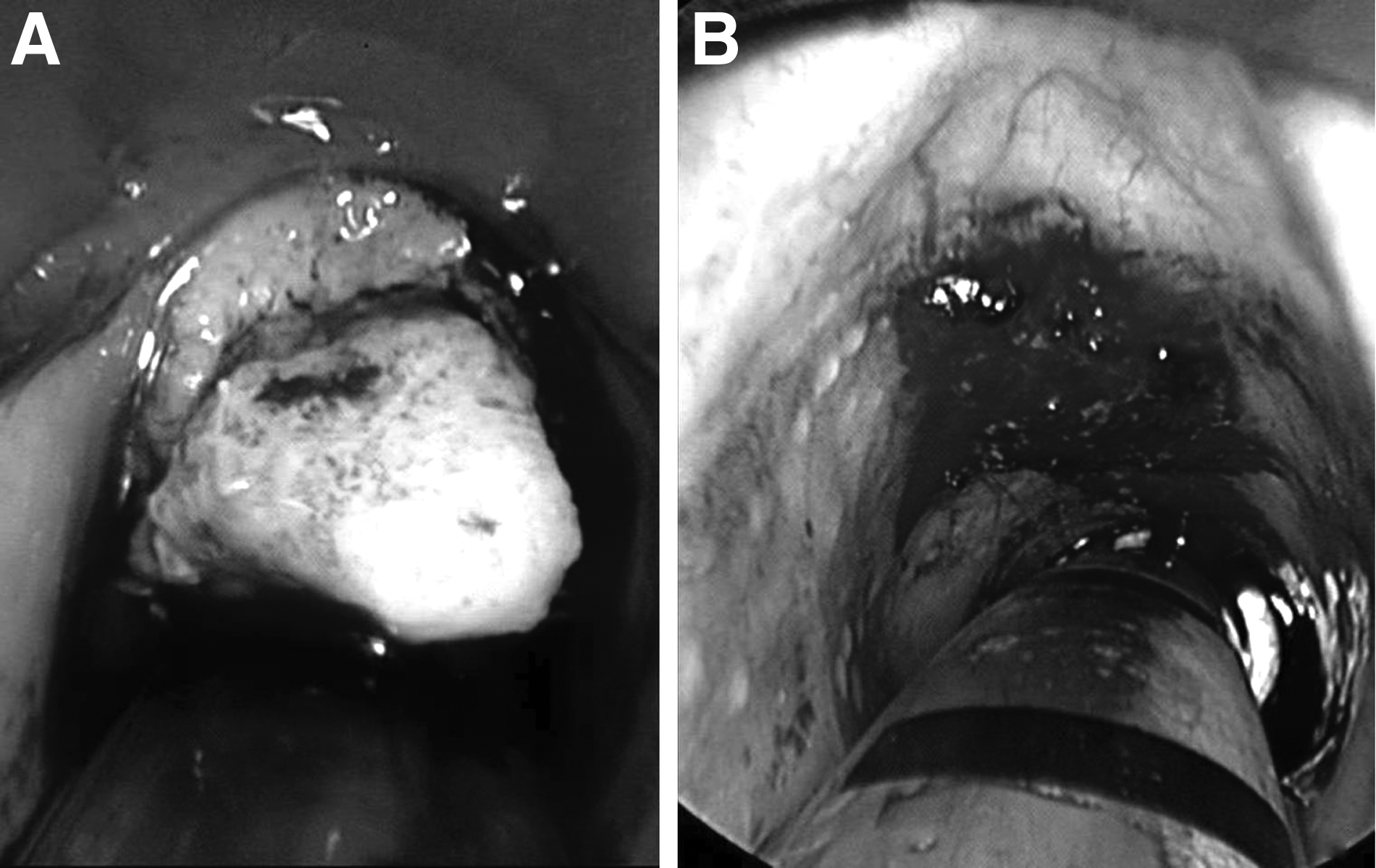
We performed flexible bronchoscopy and biopsy of the tumor, followed by the administration of CO2 laser (Acublade, Surgitouch, Luminus, San Mateo, CA) set to a circular scanning, continuous delivery mode to ablate the tumor. The pathology report revealed metastatic endometrial adenocarcinoma. After the surgery her symptoms were relieved and she was discharged on the third postoperative day. Adjuvant low-dose radiotherapy 4500 (GY/15 fx) was then performed in the laryngotracheal area.
After the intervention the patient received palliative chemotherapy and attended regular follow-up consultations in our gynecology outpatient department. She lived 19 months without upper airway compromise.
Discussion
Endometrial carcinoma is the most common gynecological malignancy in developing countries. 4 Adenocarcinoma of the endometrium is the most common type of uterine cancer. The incidence of endometrial carcinoma with extra-abdominal metastasis is approximately 2.88% (18/625). 5 Creutzberg's report showed that the actual three-year overall survival after the diagnosis of distant metastasis is 14%. 6
Surgery is the first priority of treatment for operable endometrial adenocarcinoma. The decision regarding the administration of adjuvant therapy is based on the risk of persistent or recurrent disease. Patients are risk stratified according to stage and pathological features as having low-risk, intermediate-risk, and high-risk disease. The patient in the present case had a pathological diagnosis of pT3bN0M0 (stage IIIa); moreover, histopathology revealed the presence of adenometrioid, serous, and clear cell types. According to these findings, a high-risk disease was confirmed; therefore, she underwent adjuvant CRT after the initial surgery.
Metastasis to the larynx may occur via hematogenous or lymphatic routes. In this patient, tumor emboli may have been carried in the venous bloodstream and reached the larynx through the left heart, aorta, upper thyroid artery, or upper laryngeal artery. In addition, in some cases, neoplastic cells may spread via the vertebral venous plexus.7,8 In cases of lymphatic spread, tumor cells may also form embolism at the larynx through the thoracic duct, followed by the left supraclavicular lymph nodes and subglottic lymph nodes.9,10 However, our patient had both pulmonary and laryngeal metastases without metastatic lymph nodes; thus, hematogenous spread is more likely in this case.
Under the circumstances of the case presented here as endometrial adenocarcinoma with metastasis to the larynx, curative intent, aggressive treatment was not suggested. Palliative treatment was preferred because survival of the patient was expected to be poor. Previous reports have shown that most cases of metastatic laryngeal cancer undergo tracheostomy to secure the upper airway. However, once a patient has received tracheostomy, he or she will need to live with the sequelae related to this procedure, such as inability to talk, infection of the tracheostoma, formation of granulation, or even the development of tracheoesophageal fistula. All these complications not only affect the patient's quality of life but may also be life threatening. To avoid potential morbidity, endoscopic debulking of the tumor to relieve the upper airway obstruction symptom was suggested as an alternative treatment in a previous report. 11 In the present case, we performed transoral laser ablation of the tumor and administered adjuvant low-dose regional radiotherapy. The patient tolerated the treatment well and had an inpatient hospital stay of only 3 days. She lived 19 months after the operation, with no further upper airway obstruction during the remainder of her life.
Metastatic laryngeal tumor is an uncommon but life-threatening disease. Although metastasis is a systemic problem, the patient's life may be endangered by a local condition rather than systemic status. Upper airway problems are thought to be the major cause of death in such cases. Regarding the patient's condition and the goal of palliative treatment, a less-invasive procedure with preservation of quality of life should be the priority of the management of these cases. In cases of metastatic endoluminal laryngeal tumors, we suggest endoscopic debulking surgery with adjuvant radiotherapy, instead of tracheostomy, for upper airway preservation.