
Abstract
Abstract
Background:
To improve the quality of care for dying patients, experts have called for all clinicians to be able to provide a generalist level of palliative care. Core clinical clerkships provide an opportunity to incorporate palliative care training to address the lack of required palliative care rotations at most U.S. medical schools.
Objective:
The objective of this study was to identify and quantify missed opportunities to train third-year medical students in generalist palliative care during required core clerkships.
Design:
This study was a cross-sectional survey of third-year students at a leading U.S. medical school without a required palliative care rotation.
Measurements:
Students completed a survey during the last 4 months of the 2012–2013 academic year quantifying and evaluating their experiences caring for dying patients. Attitudes were assessed using a scale from a national survey of students, residents, and faculty.
Results:
Eighty-eight students responded (response rate [RR]=56%). More than one-quarter (26%) never participated in caring for a patient who died. More than one-half (55%) never delivered significant bad news and 38% never worked with a specialist in palliative medicine. Eighty-four percent of students who cared for a patient who died and 60% of students who delivered significant bad news had one or more of those experiences that were not debriefed.
Conclusions:
At an institution without a required palliative care rotation, third-year medical students rarely or never care for patients who die during core clerkships, and when they do, their teams do not debrief or reflect on these experiences. Clinical faculty, including palliative care consultants, can address missed opportunities for palliative care training during core clerkships by augmenting and routinely debriefing students' experiences giving bad news and caring for dying patients.
Introduction
T
Many recommendations for improving undergraduate palliative care training call for additional coursework and clinical rotations.9–16 However, the crowded undergraduate curriculum and the numerous specialties competing for limited time make this difficult. Identifying existing opportunities to teach medical students clinical palliative care during core clerkships may optimize already available resources without adding courses or rotations.
When students are able to care for dying patients, they experience intense emotions17–19 and want to debrief and reflect on these challenging experiences.18,20,21 Rather than investigating debriefing and reflection, prior studies have primarily focused on students receiving feedback about specific tasks such as delivering bad news or conducting goals of care discussions. 4 Studies that have investigated debriefing and reflection about patient deaths focused on students' most memorable death 18 rather than students' experiences throughout required clerkships.
The purpose of this study was to identify and quantify missed opportunities training third-year medical students in clinical palliative care during core rotations at an institution without a required palliative care rotation. We defined training opportunities in clinical palliative care as delivering significant bad news to seriously ill patients, caring for dying patients, debriefing or reflection on these experiences, and working with palliative care clinicians.
Methods
We surveyed third-year medical students at Harvard Medical School (HMS) during the last 4 months of the 2012–2013 academic year. Students received surveys electronically three times during the study period, with two opportunities to complete a paper version. Completing the survey entered students in a lottery to win a $10 gift card. The HMS Institutional Review Board approved this study. All students complete a year-long, required curriculum at one of four Harvard-affiliated hospitals with established palliative care services. There is no required hospice or palliative care rotation.
Students reported the number of experiences they had caring for dying patients, delivering significant bad news (defined as the diagnosis, recurrence, or progression of a life-threatening illness), and working with palliative care clinicians. Students also reported the number of these experiences that were debriefed or reflected on with their team. Attitudes about caring for dying patients were assessed with a scale used in a national survey of students, residents, and faculty. 4 Survey data was collected and stored using RedCAP. 22
Descriptive statistics were calculated for the quantity of students' experiences. We divided the number of experiences where debriefing occurred over the total number of experiences to calculate the percent of experiences debriefed. We used a similar method to calculate the percent of unsupervised giving bad news experiences. Student attitudes were collapsed from a 4-point Likert scale to “agree” and “disagree” for analysis. JMP (JMP, version 10.0, SAS Institute Inc., Cary, NC) was used for all statistical analyses.
Results
We surveyed 157 third-year students. Eighty-eight students completed the survey constituting a 56% response rate. The mean age was 26 and 48% of respondents were female. Students from each of the four Harvard-affiliated hospitals participated (Beth Israel Deaconess Medical Center [34%], Brigham & Women's Hospital [33%], Cambridge Health Alliance [7%], and Massachusetts General Hospital [26%]).
Experiences caring for dying patients
Students cared for a median of one patient who died (range, 0–8) and 26% of students (n=23) never cared for a patient who died. Students delivered significant bad news a median of 0 times (range, 0–10), with 55% of students (n=48) never delivering significant bad news. Students worked with a palliative care clinician a median of 1 time (range, 0–6), with 38% of students (n=33) never working with a palliative care clinician.
Of the 61 students who cared for a patient who died and responded to the question about debriefing with their teams, 84% (n=51) had one or more patient deaths that were not debriefed and 56% (n=34) never debriefed a patient death. Of the 35 students who delivered significant bad news and responded to the question about debriefing, 60% (n=21) had one or more experiences giving bad news that were not debriefed, and 31% (n=11) never debriefed with their team about these experiences.
Of the 36 students who delivered significant bad news to a patient and responded to the question about giving bad news alone, 31% (n=11) delivered bad news without supervision on one or more occasion, with 17% (n=6) never having supervision when delivering significant bad news. Figure 1 illustrates students' experiences.
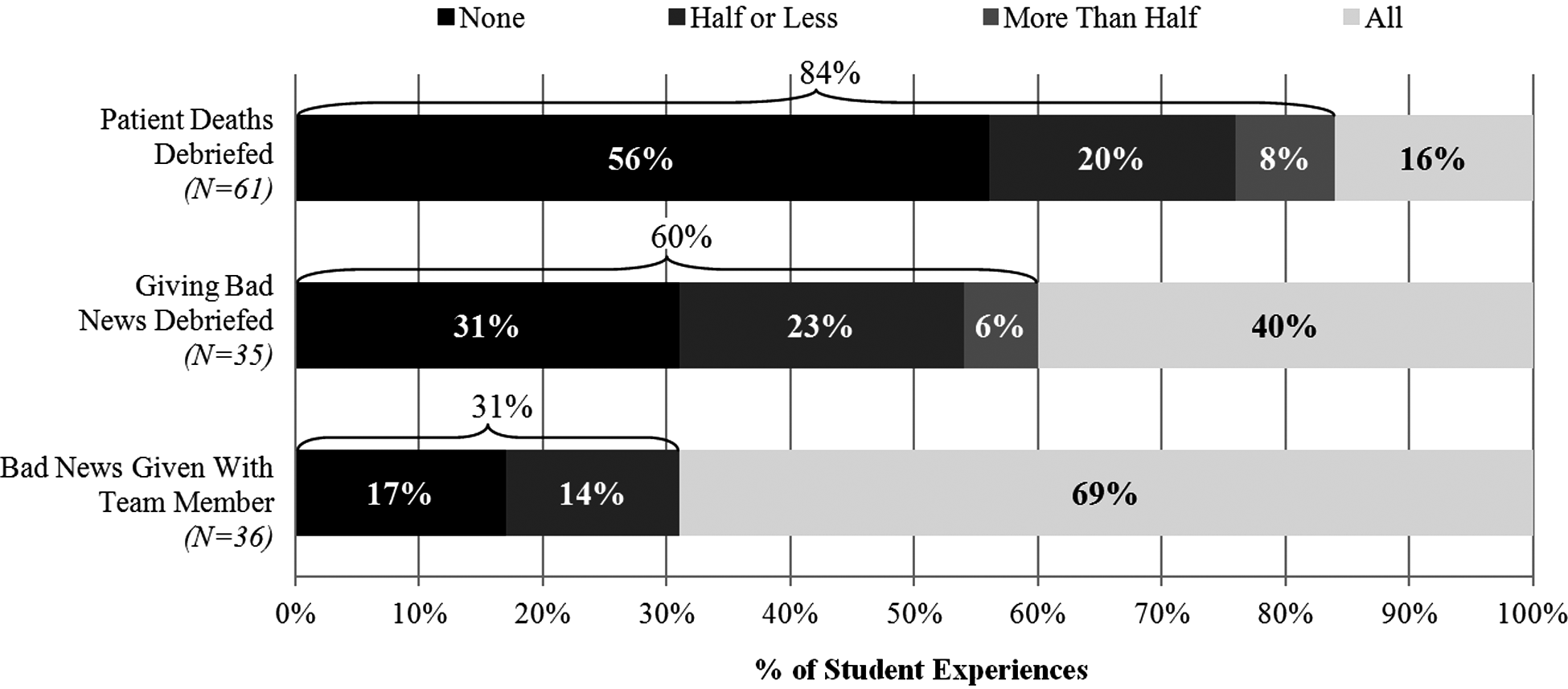
Third-year students' experiences caring for seriously ill and dying patients. The proportions of students who cared for a patient who died or gave bad news but did not debrief the experience represent the degree of missed opportunities in generalist palliative care training during core clerkships.
Evaluation of training
Eighty-three percent of students (n=73) wanted more education on caring for seriously ill and dying patients during core clerkships, and 42% (n=37) reported too little participation in caring for patients at the end of life. Of students who did not care for a patient who died and who responded to whether they would have liked to have cared for a patient who died, 100% (n=21) would have liked to care for a patient who died.
Student attitudes
Eighty-six of the 88 participants responded to the attitude survey. Eighty-two students (93%) reported that it was “moderately” or “very” important to learn about caring for seriously ill and dying patients. Half (n=43) agreed that caring for dying patients is depressing, 37% (n=32) would feel guilty after a patient died, and 24% (n=21) dread having to deal with the emotional distress of family members at the end of life. Table 1 presents students' attitudes for each item.
Discussion
Despite students expressing a clear interest and desire to learn about and care for seriously ill and dying patients, we found that there were many missed opportunities for students to receive training in generalist palliative care during required clerkships. One of the primary missed opportunities we identified was the lack of exposure to caring for patients who died. The lack of mentored debriefing of experiences caring for patients who died and experiences delivering significant bad news represent additional important missed opportunities that add to the paucity of medical students' exposure to generalist palliative care training.3,18,23 Our students also had few experiences working with palliative care clinicians even in hospitals with robust palliative care consultation services.
The desire for debriefing and reflection, as opposed to “feedback” on a task, has been reflected in qualitative studies of medical students14,18,20,21 and physicians.24,25 Our attitude data showing that students feel guilty, depressed, and challenged by the emotional burden of families when caring for dying patients confirm previous findings that the emotional aspects of this care are particularly challenging. 4 These findings support the importance of debriefing and reflection that focuses on the emotional aspects caring for dying patients. A challenge for future studies is to define what constitutes “adequate” debriefing and reflection. 20
Because this study was a single-institution survey with a limited response rate, the generalizablilty of the results to third-year medical students at schools without required palliative care rotations may be limited. Fourth-year students were not included in this study because their coursework is primarily elective and not standardized across the student population. Finally, we defined opportunities for training in palliative care as exposure to caring for significantly ill and dying patients, mentored debriefing and reflection, and exposure to palliative care clinicians. Other opportunities for palliative care training during core clerkships such as training in pain management and exposure to hospice could represent areas where there are additional missed opportunities.
In conclusion, at an institution without a required palliative care rotation, third-year medical students rarely or never care for patients who die during core clerkships, and when they do, their teams do not debrief or reflect on these experiences. Clinical faculty in all required rotations and palliative care consultants can address these missed opportunities by augmenting and more consistently debriefing students' experiences caring for seriously ill and dying patients and by focusing debriefing on the emotional aspects of providing this care.
Footnotes
Author Disclosure Statement
No competing financial interests exist.