
Abstract
Abstract
Background:
Malignant bowel obstruction (MBO) is a common condition among palliative patients and has limited management options. There is a paucity of widely accepted national and international evidence-based guidelines to direct the management of MBO in palliative patients.
Objective:
The aim of this study was to survey current practice in New Zealand of nonopioid pharmacological management of MBO and compare it with the available literature.
Methods:
The study utilized a survey consisting of three scenarios: probable incomplete malignant bowel obstruction (PIMBO), incomplete malignant bowel obstruction (IMBO), and complete malignant bowel obstruction (CMBO). An online survey was conducted over 2 months targeting palliative medicine practitioners working in a hospital, hospice inpatient unit, or community setting in New Zealand.
Results:
Forty-eight doctors responded. Of the respondents, 56.3% used guidelines to manage MBO; however, 88.9% of the guidelines used were locally generated at the doctor's institution. Metoclopramide was the drug of choice in treating PIMBO, whereas haloperidol and hyoscine butylbromide (HB) were the preferred drugs as the severity of bowel obstruction increased. Dexamethasone was accepted as standard practice for managing all severities of MBO. A variation in the preferred starting and maximum dose of all the drugs was seen. There was a decrease in the use of laxatives and enemas as the severity of MBO increased.
Conclusion:
Variation in practice for managing MBO was evident among doctors in New Zealand. There is a need for national and international evidence-based guidelines to help define best management for the differing severities of this problematic condition.
Introduction
M
Treatment options for MBO include surgery, endoscopy±self-expanding metal stents (SEMS), and pharmacotherapy. According to a European Association for Palliative Care (EAPC) consensus paper, 6% to 50% of patients with MBO are poor operative candidates, which leaves endoscopy and pharmacotherapy as the only options for a large proportion of MBO patients. 5 Most of the research done on the management of MBO combines patients with different severities of MBO, and this heterogeneity makes interpretation of the data difficult. 1 As it currently stands, the literature is devoid of national concensus guidelines in New Zealand for selecting treatment options for patients suffering from MBO. 2
The aim of this study was to define the current practice in New Zealand of nonopioid pharmacological management of MBO at different levels of severity—probable incomplete malignant bowel obstruction (PIMBO), incomplete malignant bowel obstruction (IMBO), and complete malignant bowel obstruction (CMBO).
Method
Survey design
The survey was designed in two parts (the complete survey can be found at www.surveymonkey.com/s/PMBONZ). The first part collected demographic data about the participants. The second part of the survey collected information on the current nonopioid pharmacological practice of treating MBO. Three hypothetical scenarios depicting patients with PIMBO, IMBO, and CMBO formed the framework of the second part of the survey (see Table 1). For the purpose of this study, incomplete bowel obstruction was defined as an obstruction where some gas and bowel content is able to pass through the point of obstruction, whereas complete bowel obstruction was defined as complete occlusion of the bowel lumen. 22 The definition of PIMBO was similar to incomplete bowel obstruction but with a greater degree of uncertainty as characterized by an inconsistent pattern of nausea and vomiting and absence of colic.
Ethical approval was sought and deemed not necessary by the national ethics committee.
Survey distribution
The target population for the survey was palliative medicine specialists and other doctors working in a hospice inpatient unit, community hospice, or hospital palliative care setting in New Zealand.
The survey was distributed electronically to members of the New Zealand chapter of the Australia and New Zealand Society of Palliative Medicine (ANZSPM Aotearoa) and via Hospice New Zealand to all the hospices in New Zealand. ANZSPM Aotearoa e-mailed the survey link to their 89 members. Information was collected over a 2-month period (April 28 to June 24, 2013) with one reminder e-mail sent through ANZSPM Aotearoa at 6 weeks.
Due to New Zealand privacy laws, it was not possible to get a list of all the doctors to whom the survey was e-mailed. Therefore, it is not possible to accurately calculate the response rate.
Data collection and analysis
All responses were collated into a central database. Statistical analysis included χ2 test specifically looking for trends in use of antiemetics, antisecretory drugs, route of administration, oral laxatives, and enemas. One-way analysis of variance (ANOVA) was used to analyse differences in prescribed doses of dexamethasone across the three scenarios. A p value of <0.05 was considered to be significant. Drug dose usage was reported as median with range.
Results
Demographics
There were a total of 48 responses. The overall response rate of the survey was difficult to calculate due to the lack of a confirmed denominator. The majority of respondents were members of ANZSPM (43.8%). The demographic data are summarized in Table 2 and show that the respondents were an experienced group regularly involved in treating MBO.
MBO, malignant bowel obstruction.
Use of guidelines to treat MBO
Of the total 48 participants, 27 (56.3%) used guidelines to manage MBO, and the majority (88.9%) utilized local guidelines generated at the participant's institution. Only 7.4% used existing literature, specifically quoting the palliative care formulary (PCF) and the systematic review by Mercadante et al. 7
Interpretation of the likelihood of MBO
Participants interpreted the scenarios depicting IMBO and CMBO as more likely to be diagnostic of MBO. Whereas the scenario depicting PIMBO was interpreted more variably and displayed a bell curve distribution (Fig. 1).
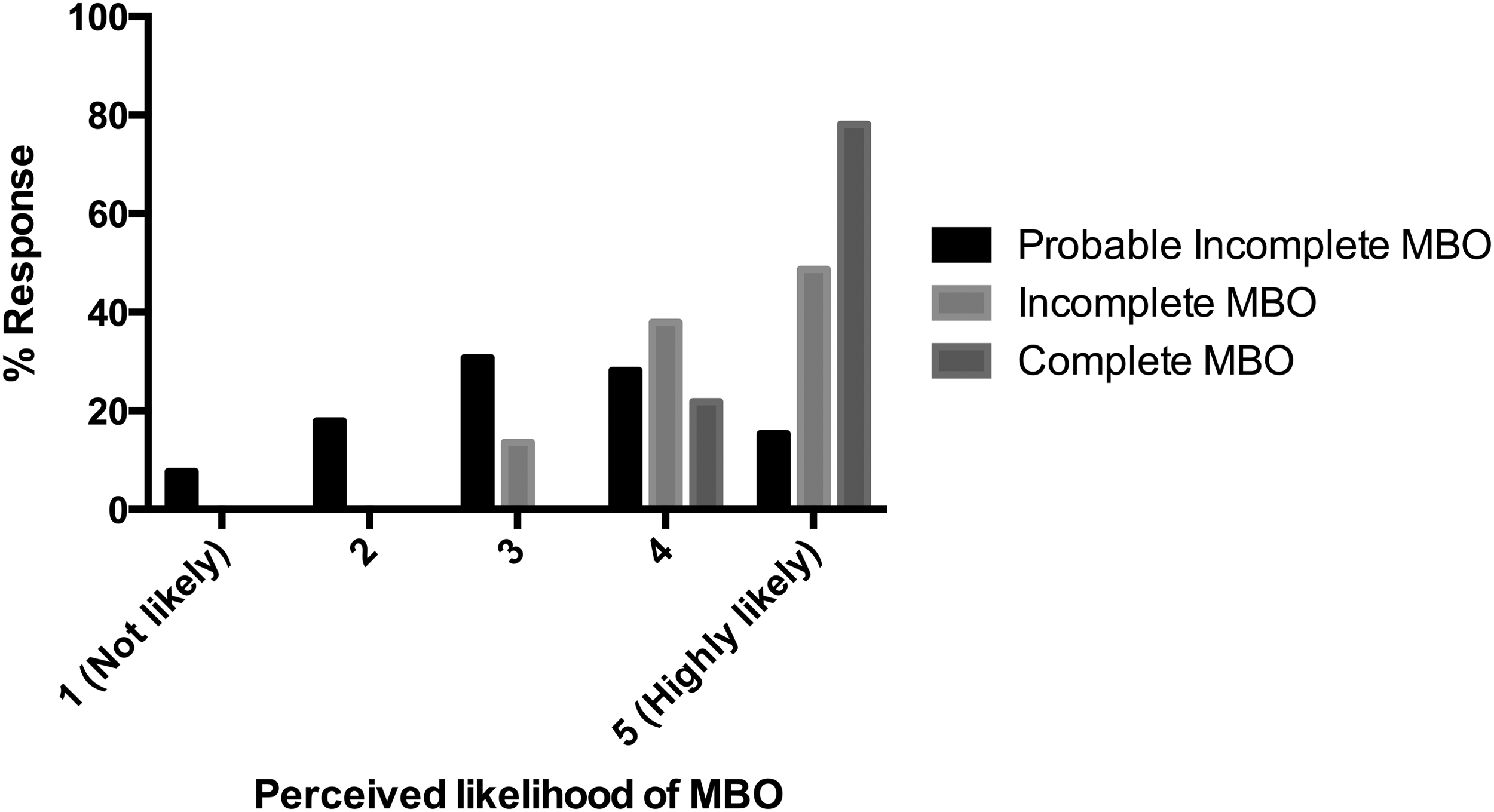
The interpretation of the respondents with regards to the likelihood of MBO for all three scenarios: PIMBO, IMBO, and CMBO.
Preferred drug to treat MBO
The preferred first choice of drug in treating PIMBO, IMBO, and CMBO can be seen in Figure 2 and dosing in Table 3. Metoclopramide was the most commonly chosen first-line drug for management of PIMBO. However, there was a significant trend for reduced use of metoclopramide in the scenarios depicting IMBO and CMBO (p<0.001).

Preferred first-choice of drug for the management of all three scenarios: PIMBO, IMBO, and CMBO.
CMBO, complete malignant bowel obstruction; IMBO, incomplete malignant bowel obstruction; PIMBO, probable incomplete malignant bowel obstruction.
Hyoscine butylbromide (HB) and haloperidol were the most commonly chosen first-line drugs in the management of IMBO and CMBO with a significant trend to their increased use in these scenarios (p<0.001 for both drugs). A significant increase for cyclizine use in both the IMBO and CMBO versus PIMBO was also observed (p=0.003).
In IMBO, octreotide was chosen second line if HB failed to control symptoms. Levomepromazine was generally avoided in the first-line treatment for MBO.
Route of drug administration
The majority of participants preferred to administer drugs via the subcutaneous route –bolus or continuous subcutaneous infusion (CSI). The CSI route was chosen increasingly as the severity of the MBO increased through the scenarios from PIMBO to CMBO (p=0.019) as shown in Figure 3.

Preferred route of administration of drugs in the all three scenarios: PIMBO, IMBO, and CMBO scenarios.
Ancillary drugs
There was a statistically significant reduction in the use of oral laxatives and enemas as the severity of MBO increased (p<0.001) (Fig. 4).
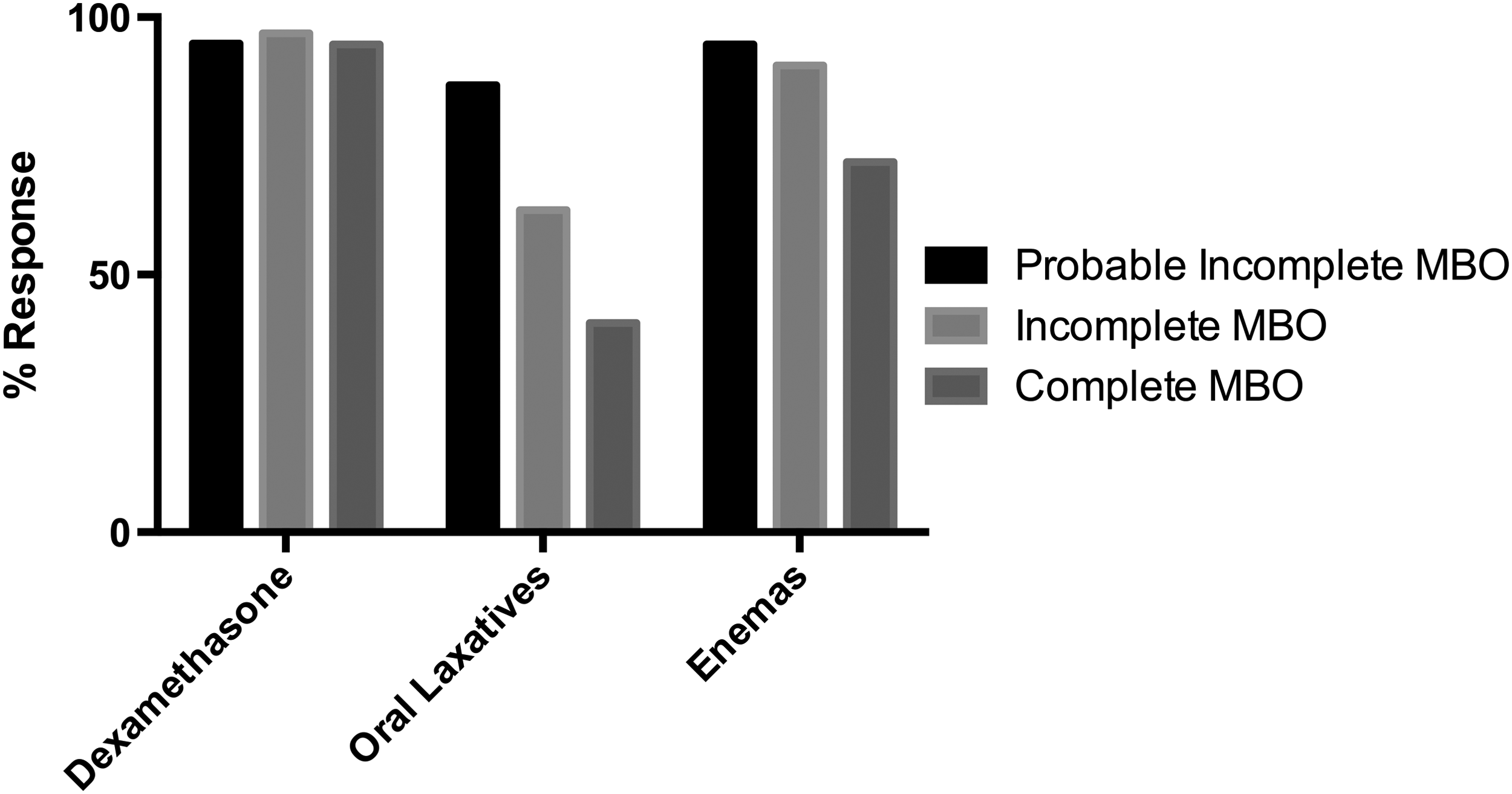
Use of ancillary drugs in the management of MBO for all three scenarios: PIMBO, IMBO, and CMBO.
The majority of the participants used dexamethasone in the management of MBO. There was no significant difference in the starting (p=0.24) or maximum (p=0.414) doses of dexamethasone between the three case scenarios. In all three case scenarios, most participants would trial dexamethasone for 5 to 7 days to assess for a response before weaning or stopping the dexamethasone (Fig. 5).
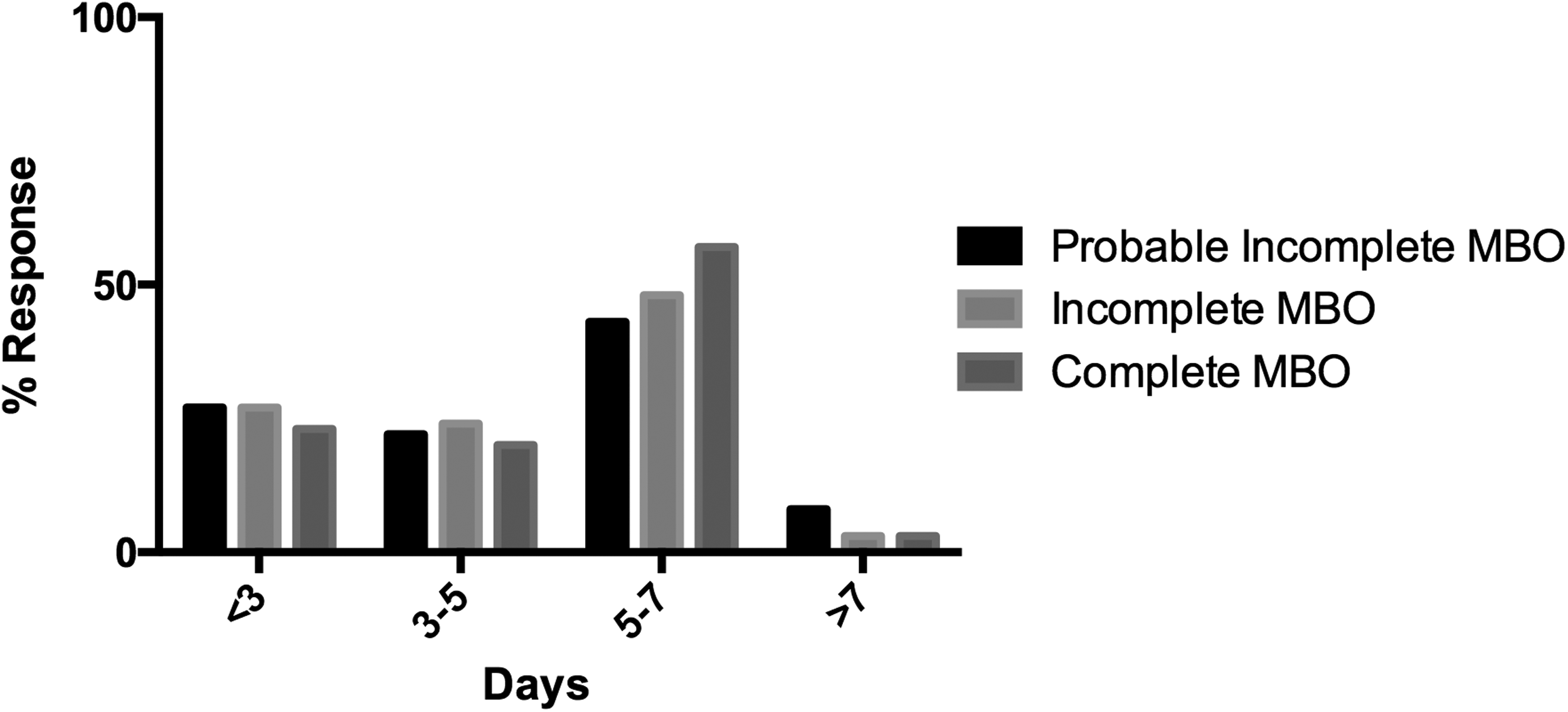
Number of days participants would trial dexamethasone to assess for response for all three scenarios: PIMBO, IMBO, and CMBO.
Participants were given the option of mentioning any other drugs they would consider in first-, second-, or third-line management of MBO. A small percentage of participants indicated that they would consider the use of ranitidine in the management of IMBO (6.3%) and CMBO (3.1%).
Discussion
Here we present the first national survey to document current practice in the nonopioid pharmacological management of MBO at different levels of severity in New Zealand. Pharmacological management of MBO is variable, with 56.3% of the respondents indicating that they use clinical guidelines, the majority of which are locally generated (88.9%).
The results of the survey showed that participants were more confident diagnosing IMBO and CMBO than they were diagnosing PIMBO, and this is consistent with the literature.10,13 Most studies done in palliative patients include patients at various levels of severity and do not necessarily separate patients with CMBO and IMBO, which makes interpretation of the data difficult. 1
MBO can be incomplete or complete, is often multilevel, and can develop insidiously over weeks to months.1,2,5 In many palliative settings radiological imaging is not readily accessible (community or inpatient hospice). Plain erect and supine abdominal X-rays can be arranged without too much cost to ambulatory patients; however, plain abdominal films are unable to accurately confirm clinical findings of MBO in about one-third of patients. 22 More-sophisticated imaging such as contrast radiography and computed tomography scans are costly, require travel or admission to a hospital or radiology facility, and are sometimes not appropriate in palliative patients where the result of the test is unlikely to change the course of treatment. Moreover, although computed tomography has a high sensitivity (81%) for diagnosing complete bowel obstruction and is particularly useful for identifying obstruction caused by adhesions, it is much less reliable in diagnosing incomplete bowel obstruction (sensitivity of 48%). 22 Therefore, in New Zealand, the diagnosis of MBO in patients who are in a hospice inpatient unit or in the community is often made on clinical history and examination alone.
Preferred drugs and dosages
Currently, there is no standard approach to treating the different stages of MBO, that is, PIMBO, IMBO, and CMBO. 2 In the case scenario depicting PIMBO, metoclopramide was the drug of first choice for 89.7% of the respondents. The literature supports use of metoclopramide in patients with incomplete bowel obstruction where colic is absent, with recommended doses ranging from 60 mg to 240 mg.1,5 It appears that the respondants used lower doses of metoclopramide to treat incomplete bowel obstruction. However, the dose of cyclizine used for the management of MBO was consistent with current literature.1,5
Haloperidol and HB were the most popular drugs in IMBO (52.9% and 44.1%, respectively) and CMBO (40.6% and 59.4%, respectively). The existing literature displays wide variation in the dose of haloperidol recommended to treat MBO, ranging from 3 mg/day to 15 mg/day.1,5,10 Again, the respondants used lower doses than what is recommended. Possible explanations for this conservative practice include positive results seen at lower doses or wariness of extrapyramidal side effects.
The median starting dose of HB was consistent with current literature, where the recommended dose of HB ranges from 40 mg to120 mg.1,5–7,9 Higher doses of HB are usually limited by the unacceptable anticholinergic side effects of the drug.
Octreotide has been reported to be superior to HB in controlling symptoms of MBO.2,12,15 There are also studies that suggest that earlier use of octreotide may prevent the development of definitive obstruction by allowing the recovery of bowel transit and preventing the pathological distension-secretion cycle, although these studies were conducted on a very small cohort of patients.8,13 Despite this evidence, octreotide was generally used second-line if HB failed to control symptoms.
Dexamethasone
The majority of participants felt dexamethasone had a role in the management of PIMBO, IMBO, and CMBO. Dexamethasone is presumed to reduce intestinal mural edema and hasten resolution of MBO and is widely accepted as standard treatment for MBO.1,7,10 Dexamethasone doses between 6 mg and 16 mg administered intravenously have shown a trend toward resolution of bowel obstruction symptoms without significant morbidity, although the results were not statistically significant. 16 Despite there being no firm evidence for the role of dexamethasone in treating MBO, the general recommendation is that dexamethasone be trialed for the possibility that it may hasten recovery from MBO and also for its nonspecific effect on general well-being. 10
This survey exhibited a wide variation in the starting dose of dexamethasone, ranging between 4 mg and 16 mg, with some doctors starting on a small dose, presumably to use the smallest dose that is effective, whereas others start on a larger dose (16 mg), presumably to wean according to effect. There is little evidence to support either method, although Twycross has mentioned that there may be a benefit in starting at a higher dose and tapering to effect so as to not miss a response. 11
In all three case scenarios, respondents displayed variation in terms of how long they would trial dexamethasone to assess for a response. The majority of respondents said they would trial dexamethasone for 5 to 7 days. Hardy et al. recommend trialing dexamethasone for 5 days and stopping it if no favorable response is seen. 10 Twycross recommends trialing dexamethasone for no longer than a week if no benefit is seen. 11 In the survey results, there is notable variation in the trial length, with a substantial number of practitioners trialing dexamethasone for <5 days before assessing response. This result seems consistent with the dearth of information on the role of dexamethasone in the management of MBO.
Laxatives and enemas
There was a significant reduction in the use of oral laxatives and enemas with increasing severity of MBO. The role of laxatives and enemas in the management of MBO has not been extensively researched. As fecal impaction has been implicated in the pathophysiology of MBO, the use of a stool softener may be beneficial in incomplete bowel obstruction.13,17 Bulk forming, osmotic, and stimulant laxatives are not recommended. 17 Where constipation is thought to be contributing to symptoms, the use of phosphate enemas have been recommended. 17
Other drugs
Participants were asked if they would use any “other” drugs in the treatment of MBO. A small percentage of participants mentioned that they would consider ranitidine (6.3% in IMBO, 3.1% in CMBO) in the management of these patients. A recent meta-analysis on the use of proton pump inhibitors (PPIs) and histamine H2 antagonists has indicated that both classes of drugs reduce gastric losses in MBO, with ranitidine being the more superior drug. 18 More recently, Currow et al. presented the results of a multicenter, randomized, controlled trial at the 19th International Congress on Palliative Care comparing the use of octreotide with that of placebo where both groups received ranitidine, dexamethasone, and parenteral fluid. 19 This study revealed no statistically significant difference in the number of days free of vomiting. The main difference was the reduced requirement for HB in the octreotide group in the first 24 hours, but this requirement increased impressively by day 3 of the trial. Similarly, the superior effect of octreotide appears to be prominent in the initial stages of managing MBO, with it no longer being superior to HB after 4 to 6 days of treatment. 12
Although not mentioned by the participants, olanzapine and amidotrizoate have also been utilized in the management of MBO. In a small, single-centered study with no cohort group, olanzapine was shown to be effective in treating nausea and vomiting in patients with an incomplete bowel obstruction due to advanced cancer. 4 Amidotrizoate (more commonly known as Gastrografin®) is a water-soluble oral contrast medium. It stimulates fluid shift into the bowel lumen resulting in diluted bowel content and an elevated pressure gradient across an obstruction, which may help passage through a narrower lumen. It stimulates bowel motility and may also reduce bowel-wall edema. 8 A systematic Cochrane review of the literature suggests that amidotrizoate does not cause resolution of small-bowel obstruction but is a good predictor of adhesive small-bowel obstructions that will resolve without surgery. 21
Route of administration
With the high prevalence of nausea and vomiting in patients with MBO, it is not surprising that the majority of respondents indicated that they would administer drugs parenterally in all three case scenarios. The most common route being subcutaneous, either by bolus or CSI method. Current literature also supports parenteral administration of drugs in patients with MBO either subcutaneously (bolus or continuous infusion), intravenously (bolus or infusion), rectally, transdermally, or sublingually.1,5
Study limitations
This study has limitations, with the most prominent one being the inability to accurately calculate a response rate due to New Zealand privacy regulations, which prevent direct access to staff lists. The three hypothetical scenarios depicting PIMBO, IMBO, and CMBO are likely to be interpreted variably especially because physical examination results and radiological investigation results were not available for all three scenarios. Participants were able to choose more than one drug for their first-line treatment; however, there was no opportunity to clarify if the drugs would be used in conjunction with or instead of the second drug. Participants were broadly asked if laxatives were contraindicated in the management of PMBO, IMBO, and CMBO, making it difficult to ascertain if their answer reflected that they felt all laxatives were contraindicated versus certain classes of laxatives were contraindicated (e.g., osmotic, stimulant, and bulk-forming laxatives).
Conclusion
There is variation in how palliative medicine practitioners in New Zealand currently manage the different severities of MBO. This can be explained by the absence of good data to guide practice and the lack of widely accepted national and international evidence-based guidelines for the management of MBO.
Footnotes
Acknowledgments
We thank ANZSPM Aotearoa, Hospice New Zealand, and Parag Bhatnagar (technical support).
Author Disclosure Statement
No competing financial interests exist.