
Abstract
Abstract
Background:
Most pediatric hospice patients receive services from agencies typically oriented to adults. Information regarding how pediatric hospice patients differ from adult hospice patients is lacking.
Objective:
We aim to assess differences between pediatric and adult hospice patients regarding patient characteristics and outcomes.
Methods:
We compiled a retrospective inception cohort of patients enrolled at nine hospices in the CHOICE network (Coalition of Hospices Organized to Investigate Comparative Effectiveness) between August 1, 2008 and June 30, 2012. Measurements included patient characteristics and outcomes, including discharge from hospice and site of death.
Results:
Among 126,620 hospice patients, 986 (0.8%) were 18 years of age or younger. Pediatric patients were less likely to have an admitting diagnosis of cancer (odds ratio [OR] 0.62; 95% confidence interval [CI]: 0.54–0.72). Although children were less likely to use oxygen at enrollment (OR 0.31; 95% CI: 0.26–0.37), they were more likely to have an enteral feeding tube (OR 4.04; 95% CI: 3.49–4.67). Pediatric patients were half as likely as adults to have a do-not-resuscitate order (DNR) order upon hospice enrollment (OR 0.52; 95% CI: 0.46–0.59). The average hospice length of stay for pediatric patients was longer than that of adults (103 days versus 66 days, p<0.001). Children were more likely to leave hospice care (OR 2.59; 95% CI: 2.00–3.34), but among patients who died while enrolled in hospice, pediatric patients were more likely to die at home (OR 3.25; 95% CI: 2.27–3.88).
Conclusions:
Pediatric hospice patients differ from adult patients in their broader range of underlying diagnoses and their use of hospice services.
Introduction
T
Most pediatric and young adult patients who receive hospice services enroll in hospice agencies typically oriented to adult patients. A 2007 survey of member hospices by the National Hospice and Palliative Care Organization found that whereas 78% of hospices reported that they serve pediatric patients, only 36.6% had a formal pediatric program in place. 2 A study of hospice patients in California found that larger hospice programs and those with memberships in pediatric-oriented professional organizations were more likely to provide services to pediatric patients. 5
Pediatric hospice patients may differ in key regards from adult hospice patients. The nature and magnitude of these differences, however, have not been well measured, so hospice programs may be ill-equipped to handle these differences. For instance, a cohort study of pediatric patients who received palliative care consultative services from hospital-based pediatric palliative care teams found that most patients were observed to be alive a year after entry into the cohort, suggesting that these patients were offered palliative care earlier in the course of illness. 6 Similarly, pediatric patients with life-limiting illness may have longer lengths of stay on hospice, due either to earlier referral or as a result of difficulties determining accurate prognoses for rare conditions. Pediatric hospice patients may be more likely to die at home than adult hospice patients, as a retrospective national case series found that the odds of children with complex conditions dying at home has been increasing over time. 7 Furthermore, whereas medical and surgical advances have resulted in increased survival for infants and children with a variety of congenital and acquired conditions, the complexity involved in caring for pediatric patients with complex chronic conditions has also increased. 8
Together, these challenges may be difficult for many adult-focused hospice programs. These and other differences would have implications regarding how hospice programs can best tailor their services appropriately for pediatric patients and their families. We therefore conducted a retrospective cohort study of all patients who enrolled in a national hospice network, with the goal of comparing and contrasting the populations of pediatric and adult enrollees.
Methods
The nine participating hospices in this study are part of the CHOICE (Coalition of Hospices Organized to Investigate Comparative Effectiveness) network. 9 CHOICE is a research-focused collaborative of hospices that all use Suncoast Solutions Electronic Health Record (EHR) Software, and that have agreed to share their data for research purposes. CHOICE projects are defined and approved by a steering committee comprising leaders from all hospices in the network. Hospices participating in this study serve between 400 and 2700 patients per day. Hospices are located in New Mexico, California, Florida, Pennsylvania, Wisconsin, Michigan, and Texas, and one that cares for patients in both Kansas and Missouri. All are not for profit.
CHOICE uses data extracted from a proprietary platform (Solutions Intelligence) developed by Suncoast Solutions. This platform creates a data warehouse that hospices use for tracking, quality measurement, and benchmarking. Warehouse data reside on a secure server that is managed by Suncoast Solutions. Data elements for this study were defined a priori and then extracted from the warehouse. Extracted data were then stripped of identifiers to create a Health Insurance Portability and Accountability Act (HIPAA)-compliant limited dataset, and then transferred as an encrypted file to the University of Pennsylvania.
We extracted a dataset containing basic demographic variables (age, gender, and race), diagnoses (admitting diagnosis and up to three additional diagnoses), and site of care at the time of enrollment (home, long-term care facility, hospital, hospice inpatient unit). We extracted clinical data elements that were markers of the severity of the illness and the complexity of care (including presence of pain, use of oxygen or Foley catheter, presence of intravenous (IV) access).
We anticipated a sample of at least 100,000 patients of whom approximately 1% would be below the age of 18. This sample would provide 80% power to detect (α=0.05) a small difference (5%) in the prevalence of selected patient characteristics between children and adults. We compiled descriptive statistics regarding counts, proportions, means, standard deviations, and ranges. We evaluated associations of either pediatric or adult patients with different characteristics or outcomes using two sample t tests and univariate logistic regression models, and report p values and 95% confidence intervals (CI). The University of Pennsylvania's Institutional Review Board approved the use of secondary data for this study. Stata version 13.1 (Stata Corp., College Station, TX) was used for statistical analysis.
Results
Of the 126,620 hospice patients admitted between August 1, 2008 and June 30, 2012 (Table 1), 986 (0.8%) were 18 years of age or younger. Over this time period, hospices served a median of 53 pediatric patients, with a range among the hospices of serving as few as 5 or as many as 354 pediatric patients.
At the time of admission to hospice; bpercentage is of patients who died.
CI, confidence interval; DNR, do-not-resuscitate order.
Patient gender and primary caregivers for pediatric patients
The adult sample was 44.2% (55,540/125,634) male, and the pediatric sample was 50.8% (501/986) male (odds ratio [OR] 1.3, p<0.01, 95% CI: 1.15–1.48). Pediatric patients were less likely than adults to identify as Caucasian (685/986, 69.5% versus 109,018/125,634, 86.8%; OR 0.28, p<0.01, 95% CI: 0.24–0.34). Primary caregivers for pediatric patients were most often mothers (81%), followed by fathers (8%) and grandparents (1.22%).
Location at time of enrollment
Nearly 75% (738/986) of the pediatric sample was living in a private residence at the time of hospice enrollment, compared with only 50% (62,795/125,634) of the adult sample (OR 1.5, p<0.001, 95% CI: 1.36–1.65). Pediatric patients were much less likely to enroll in hospice from a nursing home (7/986, 0.7% pediatric patients versus 28,310/125,634, 22.5% adult patients; OR 0.02, p<0.01, 95% CI: 0.01–0.044) or inpatient hospital setting (241/986, 24.4% pediatric patients versus 34,529/125,634, 27.5% adult patients; OR 0.59, p<0.01, 95% CI: 0.51–0.69).
Diagnoses
Adult and pediatric hospice patients had quite different admission diagnoses (Fig. 1). Although malignancies were common in both groups, compared with the adult population, pediatric patients were significantly less likely to be admitted with a diagnosis of cancer (273/986, 27.7% pediatric patients versus 47,874/125,634, 38.1% adult patients; OR 0.62, p<0.01, 95% CI: 0.54–0.72). Adults often were identified as having nonspecific or ill-defined conditions, whereas pediatric patients were more likely to have central nervous system conditions or congenital anomalies. Specific diagnoses among pediatric patients were also more likely to be unique, and to be encountered at much lower frequency than diagnoses among adult patients. Among adult patients, 97% of hospice enrollment diagnoses appeared more than once during the study period across all CHOICE sites. In contrast, 42.6% of hospice enrollment diagnoses for pediatric patients were encountered only once in the interval studied. Many of these diagnoses were for pediatric complex chronic conditions, including neurological disorders, chromosomal anomalies, congenital malformations, or inherited disorders of metabolism (Fig. 2).
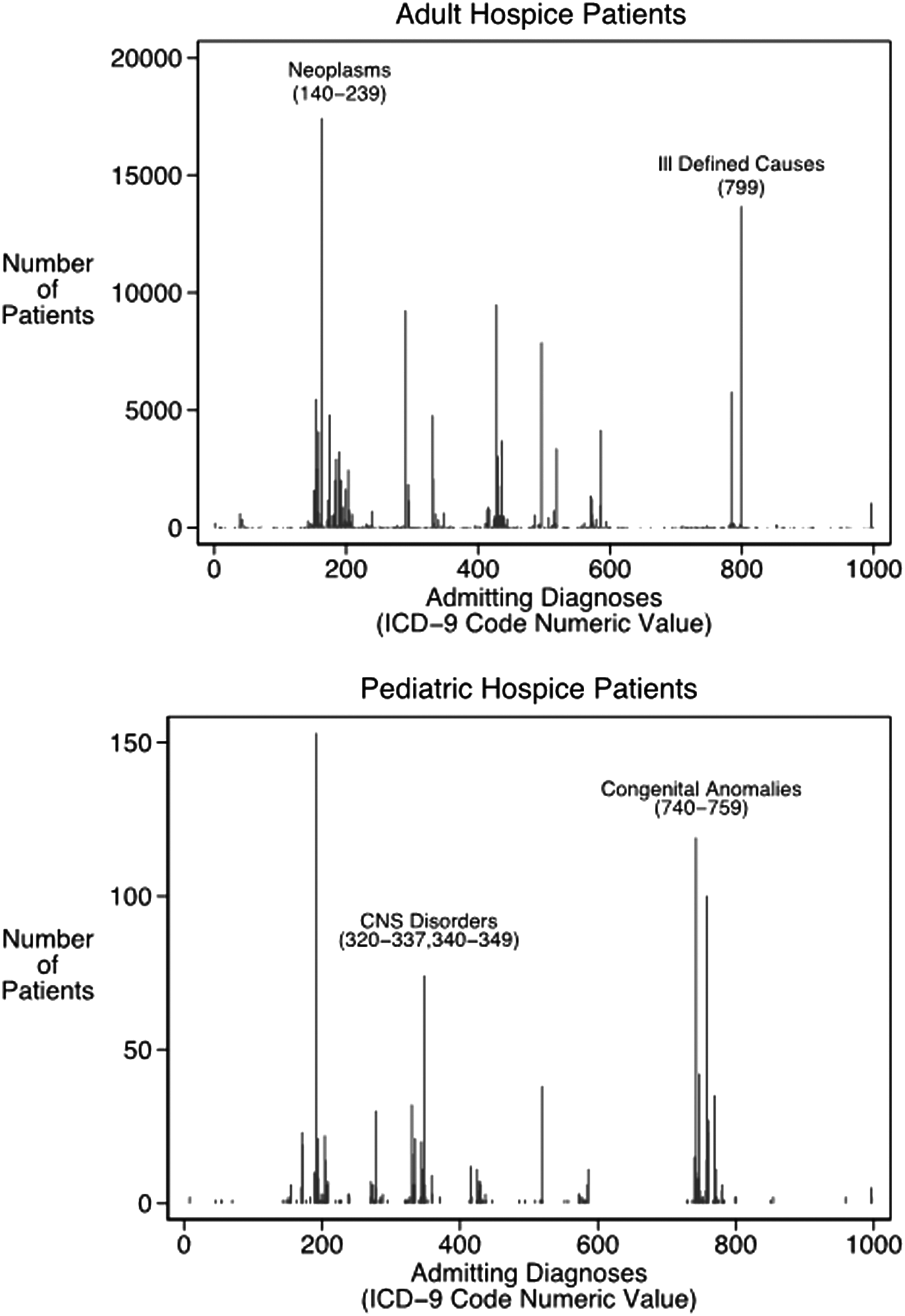
Admission diagnoses in adult compared with pediatric hospice patients.

Complex chronic conditions among pediatric hospice patients.
Medical technology
At the time of hospice enrollment, pediatric patients were significantly less likely to have indwelling Foley catheters than were adult patients (208/986, 21.1% pediatric patients versus 33,172/125,634, 26.4% adult patients; OR 0.74, p<0.01, 95% CI: 0.64–0.87). Oxygen use at the time of hospice enrollment was also much more common among adults, with 36.2% (45,545/125,634) of adult patients on supplemental oxygen at the time of hospice initiation, compared with only 15% (148/986) of pediatric patients (OR 0.31, p<0.01, 95% CI: 0.26–0.37). Enteral feeding tube (gastric or jejunal) use, however, was four times more likely among pediatric hospice enrollees than among adults (251/986, 25.5% pediatric patients versus 9795/125,634, 7.8% adult patients; OR 4.04, p<0.01, 95% CI: 3.49–4.67).
Do-not-resuscitate order (DNR) status
Pediatric patients were approximately half as likely as adults to have a DNR in place at the time of hospice enrollment (385/986, 39.05% pediatric patients versus 69,381/125,634, 55.22% adult patients; OR 0.52, p<0.01, 95% CI: 0.46–0.59).
Use of opioids
Neither pediatric nor adult patients were likely to have IV opioids ordered as part of their initial hospice orders (15/970, 1.52% pediatric patients versus 1523/124,111, 1.21% adult patients; OR 1.26, p=0.4, 95% CI: 0.75–2.1).
Mortality
In total, 68.6% (676/986) of pediatric patients and 87.6% (110,057/125,634) of adult patients in the sample died while receiving hospice care. Children were much less likely to die in hospice than were adults (OR 0.31, p<0.01, 95% CI: 0.27–0.35) (Table 1 and Fig. 3). Patients who did not die in hospice either were continuing to receive hospice services at the time of study completion, or had been discharged alive from hospice; mortality data following discharge were not available.
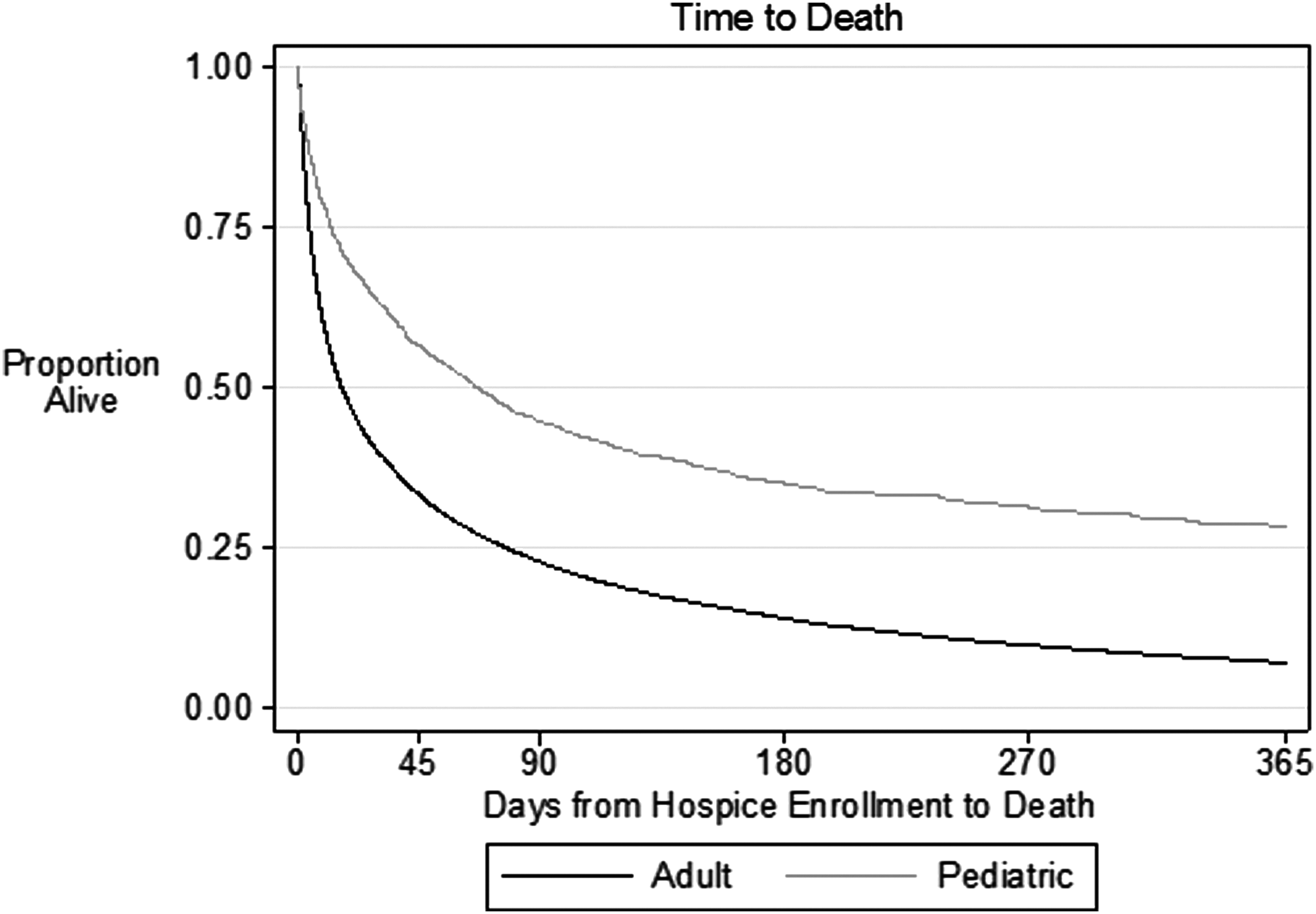
Time from hospice enrollment to death in adult and pediatric patients.
Location of death
Of 110,733 adult and pediatric patients who died while enrolled in hospice, pediatric patients were more likely than adults to die at home (517/676, 76.48% pediatric patients versus 55,291/110,057, 50.15% adult patients; OR 3.25, p<0.001, 95% CI: 2.72–3.88).
Hospice length of stay and timing of enrollment
Pediatric patients had longer hospice lengths of stay than did adults. The average length of stay in hospice for pediatric patients was 103 days (standard deviation [SD], 183 days), compared with only 66 days for adult patients (SD, 132 days; comparison of means, p<0.001). Among patients who died while in hospice, the average length of stay for pediatric patients was 62 days (SD, 122 days), and for adult patients it was 53 days (SD, 112 days; comparison of means, p=0.032) (Fig. 3). Among all patients who died in hospice, pediatric patients were less likely than adults to be referred to hospice within the last week of life (200/676, 29.59% pediatric patients versus 39,932/110,057, 36.28% adult patients; OR 0.74, p<0.01, 95% CI: 0.63–0.87).
Disenrollment from hospice
Disenrollment from hospice (also called revocation of hospice, requested by the patient or the patient's surrogate decision maker, such as a parent for a pediatric patient or a spouse for an adult patient) was more common among pediatric than adult patients enrolled in hospice, and occurred consistently even for patients who were still alive and enrolled in hospice for long periods of time (Fig. 4). Whereas 6.49% (64/986) of pediatric patients disenrolled from hospice prior to death, only 2.61% (3282/125,634) of adult patients did so (OR 2.59, p<0.01, 95% CI: 2.00–3.34).
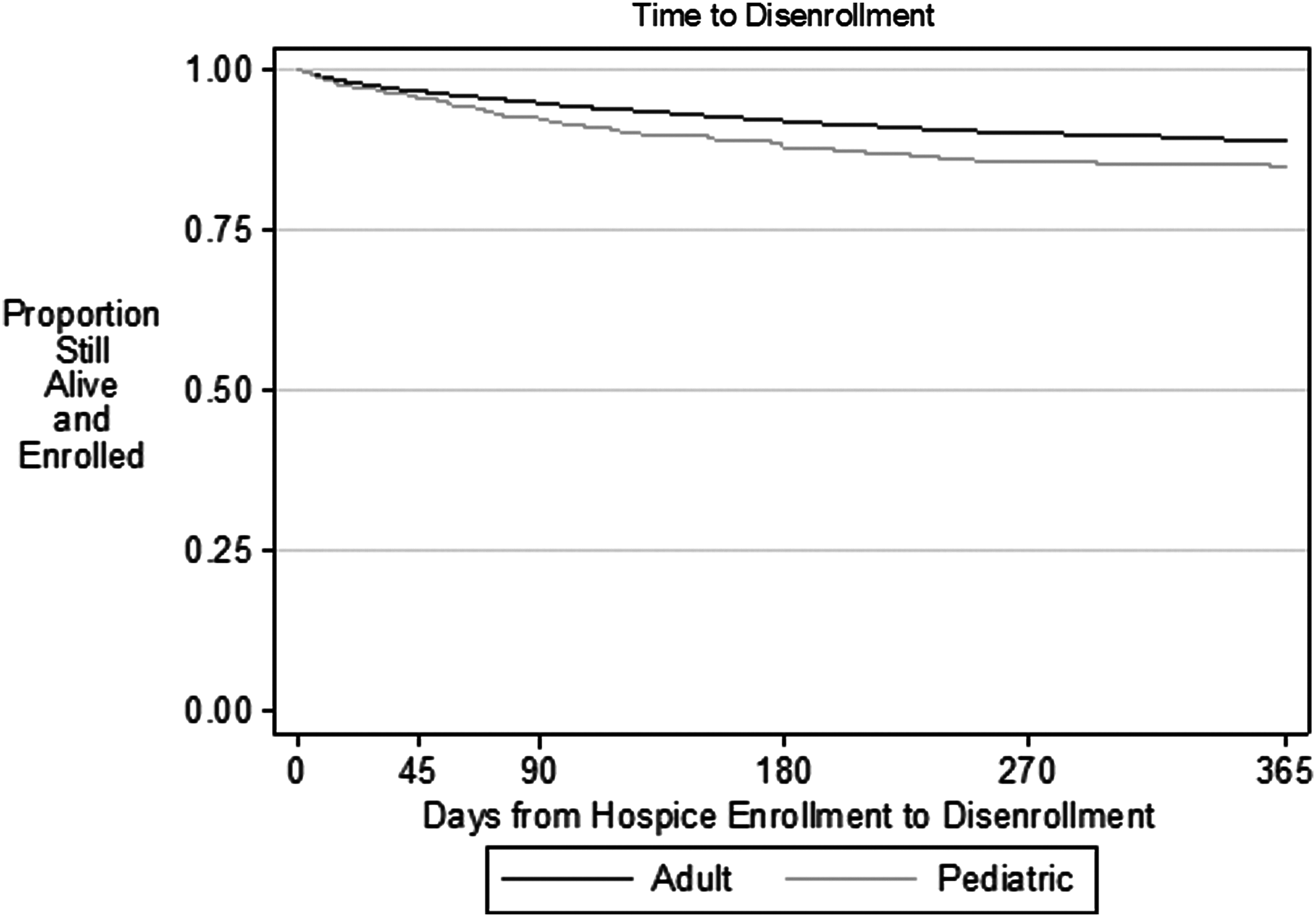
Time from hospice enrollment to disenrollment in adult and pediatric patients.
Discussion
This retrospective cohort study of pediatric and adult patients cared for at nine hospice agencies in the United States compared the demographic, clinical, and patterns of service utilization between pediatric and adult patients. In this cohort, pediatric hospice patients differed from adults in their hospice admission diagnoses, their use of medical technology, their longer hospice length of stay, their location at the time of death, and their hospice enrollment status and use of hospice services at the time of death.
Four major findings warrant further discussion. First, pediatric patients were more likely than adults to disenroll from hospice services. Specific reasons for disenrollment were not documented, but there are several potential reasons that pediatric patients may have disenrolled from hospice, and these reasons may be different from those of adult patients. Adult patients choose to disenroll from hospice due to improvement or stabilization of their condition, or to seek more aggressive care. 10 Among pediatric patients, some may disenroll from hospice to seek curative or life-prolonging treatment. Other patients may disenroll because their prognosis and treatment goals change over time as they progress to a state of chronic disability. 11 Predicting survival and disability is challenging in pediatric patients, and many patients outlive their initial prognosis. The Patient Protection and Affordable Care Act and its “Concurrent Care for Children” requirement, enacted in March 2010, has allowed children with complex chronic conditions to receive hospice and palliative care services while also continuing treatment for their underlying conditions. 12 As more patients use this benefit, program evaluations will have to assess whether concurrent care decreases disenrollment (because concurrent care becomes an acceptable norm) or increases disenrollment (because patients with earlier-stage serious illness enroll but subsequently disenroll due to stabilization or improvement of their health). Nonetheless, an understanding of the dynamic nature of hospice utilization by pediatric patients may assist hospice providers in anticipating the choices and expectations of pediatric patients and their families.
Second, length of stay for pediatric hospice patients was significantly longer than that for adult patients. This suggests that pediatric patients are referred to hospice earlier in the course of illness when compared with adults. The pattern of earlier referral among pediatric patients may, paradoxically, reflect both the difficulty in prognosticating for certain conditions (resulting in what turns out to be incorrect belief that death may be near) and the grim fatal certainty of other diagnoses (resulting in early referral). Early referral may also reflect differences in the professional practice norms in the provision of pediatric and adult palliative care, with pediatric providers more likely to offer palliative care and hospice services earlier in a patient's course, particularly with the advent of the concurrent care model. Alternatively, pediatric patients and their families may be more likely to request palliative care and hospice services earlier in the disease course, particularly in cases where a condition is known to be fatal. In addition, the length of stay for pediatric patients in this study may even be lower than in reality, given that pediatric patients are more likely to disenroll from hospice and may therefore have multiple hospice admissions. Earlier hospice referral among pediatric patients may allow patients and their families to better access the full range of hospice services available, and allow patients and families additional time to develop relationships with hospice staff. In the future, the implications of early versus late referral to hospice care will be important to study regarding patient outcomes and satisfaction of patients, family, and staff.
Third, the diversity of admitting diagnoses for pediatric hospice patients was greater than that for adult hospice patients. Furthermore, pediatric patients were much more likely than adults to be admitted with a diagnosis not previously encountered by an individual hospice. Many of these pediatric diagnoses were rare conditions, and pediatric patients are a relative rarity among hospice patients. The variety and rarity of admitting diagnoses for pediatric patients present unique challenges to hospice agencies. Although similar supportive treatments may be appropriate for many rare diagnoses, providers may have very limited experience in caring for patients with these conditions. Hospice providers may have to rely on the families of pediatric patients for information about specific conditions, or on regional centers and subspecialty referring providers to provide support and education about rare diagnoses. Collaborations between hospitals and community hospice providers have been described, and such partnerships may need to be expanded in the future. 13
Finally, pediatric hospice patients were more likely than adult hospice patients to die at home. Children are less likely than adults to reside in long-term care facilities, and so they may be more likely to die at home as a result. Limited options for pediatric hospice patients to be admitted to acute care settings prior to death could also lead to increased rates of death at home. In particular, pediatric hospitals may be less likely than adult hospitals to have general inpatient contracts for hospice patients. Finally, the difference may be due to parental preference, as a number of studies have shown that many parents prefer for death to occur at home for their children with terminal illness. 14
Several strengths and limitations should be kept in mind when interpreting the results of this study. One limitation of the study is that our data collection relied entirely on abstraction from medical charts, and thus lacked information about why pediatric patients left hospice, and whether or not they returned to hospice at a later time. We also lacked data regarding patient and family satisfaction with the hospice experience. Future observational studies should include additional narrative data from patients and families to answer these questions. Second, the pediatric sample at each hospice site was small, and so data were not analyzed by site; sites may have differed in the demographics of patients enrolled, and in the patterns of service utilization by patients. Future research should focus on elucidating the nature and magnitude of these potential differences among hospices. Third, as the care of children with complex chronic conditions continues to evolve, including expanded use of the “Concurrent Care for Children” requirement in the Affordable Care Act, patterns of hospice use in the pediatric population may change. Thus, the results of this study may need to be updated with time. Despite these limitations, this is the largest study of pediatric hospice patients, and is the first to compare pediatric and adult hospice patients on a population level.
Future population-level surveillance of the hospice population will allow further understanding of the differences between pediatric and adult hospice patients. For example, our results that pediatric patients are less likely to have a DNR, and are more likely to receive tube feeding at the time of hospice admission suggest that goals of care may differ between pediatric and adults hospice enrollees. Further examination of goals of care and how they may differ between children and adults will be useful to hospice providers serving both patient populations.
This report provides important information to hospice providers caring for both pediatric and adult patients. Hospice agencies may use this information to educate staff about expected hospice use in pediatric populations, which will likely differ from staff experience with adult patients. This report also highlights the potential need for hospice providers to build relationships with regional pediatric centers to educate staff about rare pediatric conditions, and to obtain the support necessary to optimally manage all children referred to hospice care. This study provides data to hospice providers that will allow them to better understand and improve the care of hospice patients of all ages.
Footnotes
Acknowledgments
All authors contributed to the conception and design of the study, implemented different aspects of the analysis, drafted sections of the manuscript, revised the manuscript, and approved the final version for submission.
This study was supported in part by the Agency for Healthcare Quality and Research, Coalition of Hospices Organized to Investigate Comparative Effectiveness (R21 HS21780-02) and Comparative Effectiveness and Safety of Hospital-Based Pediatric Palliative Care (1R01HS018425).
Author Disclosure Statement
No competing financial interests exist.