
Abstract
Abstract
Objective:
Our aim was to evaluate the use of very-low-dose methadone with haloperidol in the acute-care setting.
Methods:
We reviewed the records of 735 hospitalized patients receiving a palliative care consultation between 2011 and 2014. All patients with pain on opiates were offered conversion to methadone, 2.5 mg/day to 15 mg/day, in conjunction with scheduled haloperidol. Additional doses of haloperidol or short-acting opiates were given as needed for pain. Patients receiving an opiate at a morphine-equivalent daily dose (MEDD) of ≥40 mg had pain scores assessed daily, before and after conversion. Descriptive statistics were used to summarize the results.
Results:
Forty-three patients underwent conversion from another opiate (median MEDD, 78.5 mg) to methadone (median daily dose, 5 mg) and haloperidol (median daily dose, 1.5 mg). The median pain score was 5 in the week prior to conversion, 1 in week 1 after conversion (p<0.001 for difference), and zero in week 2. Similar results were seen for patients with cancer and noncancer diagnoses and for those with the highest and lowest initial opiate doses.
Conclusion:
The use of very-low-dose methadone in conjunction with haloperidol in the acute-care setting resulted in improved pain control after conversion from typical opiates.
Introduction
O
Methods
We reviewed the electronic health records of 735 patients admitted to Mills-Peninsula Hospital, Burlingame, California, who received a palliative care consultation between November 1, 2011 and February 1, 2014. The protocol was approved by the Institutional Review Board of Mills-Peninsula Health Services as exempt from further review.
All patients with pain were offered oral methadone, in daily doses of 2.5 mg to 15 mg, as initial treatment or as conversion from another opiate. Patients also received oral haloperidol on a scheduled basis, with breakthrough pain treated with oral or intravenous doses of haloperidol or a short-acting opiate. The practice preference of the attending physician dictated whether they received “full conversion” to methadone and haloperidol, using haloperidol for breakthrough pain, or “tapered conversion,” using short-acting opiates for breakthrough pain. In all cases, the previously scheduled opiates, both short-acting and long-acting, were immediately discontinued upon conversion. Pain was assessed and recorded by the bedside nurse using a standard numeric rating system, with a pain scale from 0 to 10.21,22
Data were extracted on patient demographics, medication regimens, and pain scores. The morphine-equivalent daily dose (MEDD) of opiates was calculated, assuming an opioid-naïve state.7,23 For patients treated with another opiate at an MEDD of ≥40 mg, the median and peak pain scores for each patient were recorded daily for up to 1 week prior to conversion and for 2 weeks after conversion, or until hospital discharge, and the group median and interquartile range (IQR) of these values were pooled for each week. Pain scores ≥7 were considered a marker of severe pain.22,24 The percentage of severe pain scores was recorded daily and pooled for the group. The number of patients with a ≥2-point drop or increase in median pain scores from week –1 to week 1 was also recorded.
Descriptive statistics were used to summarize results. Comparisons of the number of severe pain scores between two time points or subgroups were made with the χ2 test of association, and comparisons of median pain scores were made with the Wilcoxon signed rank test, using IBM SPSS Statistics for Windows, Version 22.0.0 (IBM Corp., Armonk, NY).
Results
The flowchart for study inclusion is shown in Figure 1, with baseline patient characteristics in Table 1 and details of the regimen in Table 2. Of the 43 patients converted to methadone and haloperidol, 18 had full conversion, with haloperidol given as needed for breakthrough pain, and 25 had tapered conversion, with short-acting opiates given as needed. The group median MEDD was 78.5 mg prior to conversion, 15 mg in week 1, and 10.9 mg in week 2. Methadone conversion was started a median of 6 days after admission. The median methadone dose given was 5 mg/day, and the median haloperidol dose (scheduled and as-needed) was 1.5 mg/day. For tapered conversion, patients received additional doses of short-acting opiates for breakthrough pain (median MEDD, 20 mg/day in week 1, and 10 mg/day in week 2).
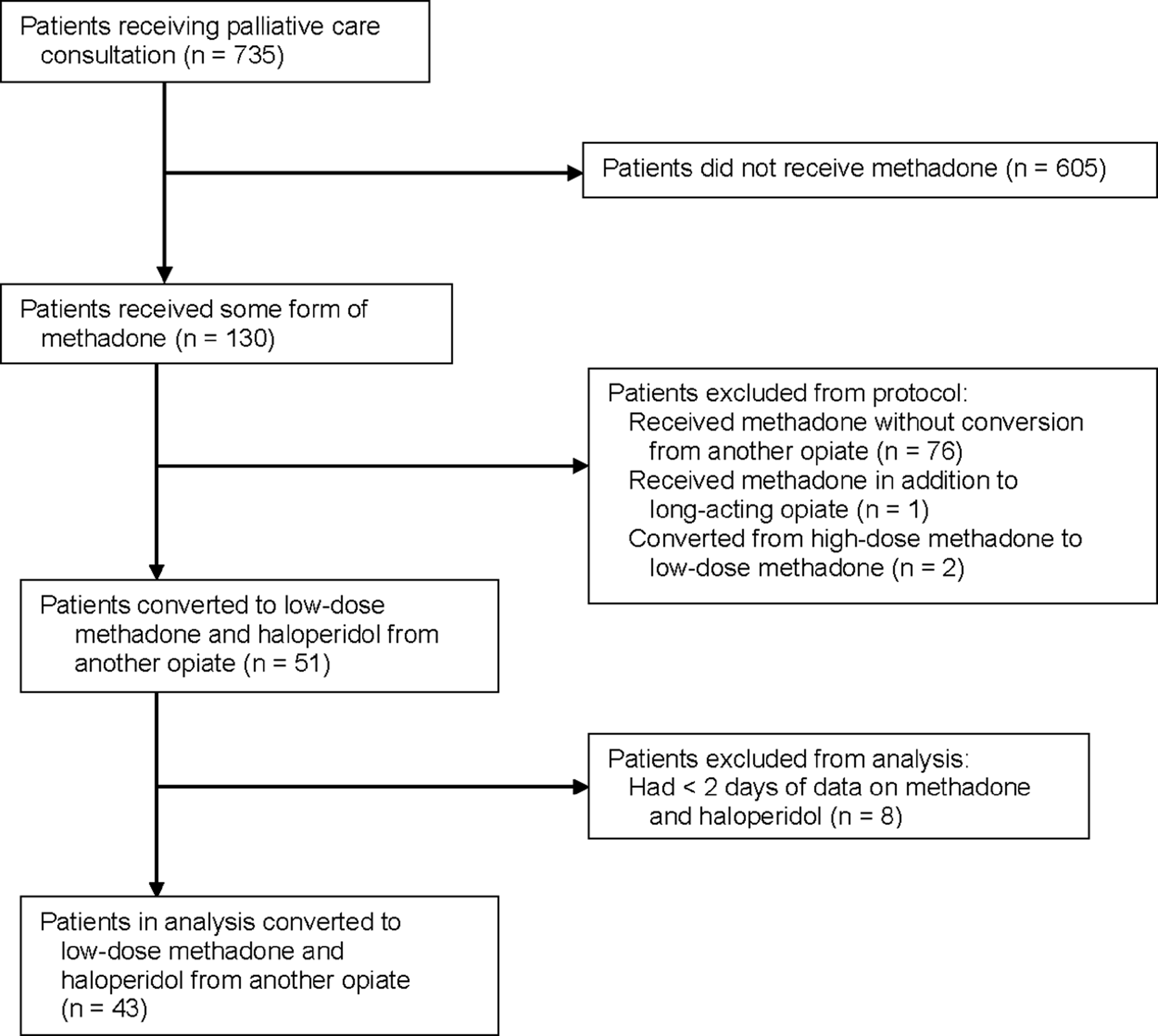
Flowchart of patient inclusion criteria.
IQR, interquartile range; SD, standard deviation.
IQR, interquartile range; MEDD, morphine-equivalent daily dose.
The group median pain score was 5 in week -1, 1 in week 1, and 0 in week 2 (Table 3), representing an 80% reduction in the first week after conversion (p<0.001 for difference). The percent of severe pain scores (score ≥7) was 38.5% prior to conversion, 22.8% in week 1, and 15.6% in week 2. A pain score drop of ≥2 points occurred in 19 patients (44%). No patient had a ≥2-point increase in pain or developed signs of toxicity to methadone or haloperidol requiring drug discontinuation, and none showed signs of withdrawal.
P value for change from week -1 to week 1.
Average of each patient's % severe pain scores, defined as ≥7, for each week.
Number of patients whose median pain score dropped by ≥2 points from week -1 to week 1.
IQR, interquartile range.
There was a significantly greater reduction in severe pain scores by week 1 for full conversion, using haloperidol for breakthrough pain, compared with tapered conversion, using short-acting opiates (Fig. 2; p=0.02 for difference). Similar reductions in scores were seen in patients with cancer and noncancer diagnoses (Table 4; p=0.06 for difference). Significant improvements in pain scores were seen for those with an initial MEDD of ≥250 mg (median, 415 mg) and for those with a MEDD of 30 mg to 80 mg (median, 37.8 mg), but there was a significantly greater improvement associated with highest-dose opiate group (p<0.001 for difference). The patient with the highest initial MEDD (1600 mg) had full conversion to methadone 7.5 mg/day, for a conversion ratio of 213.
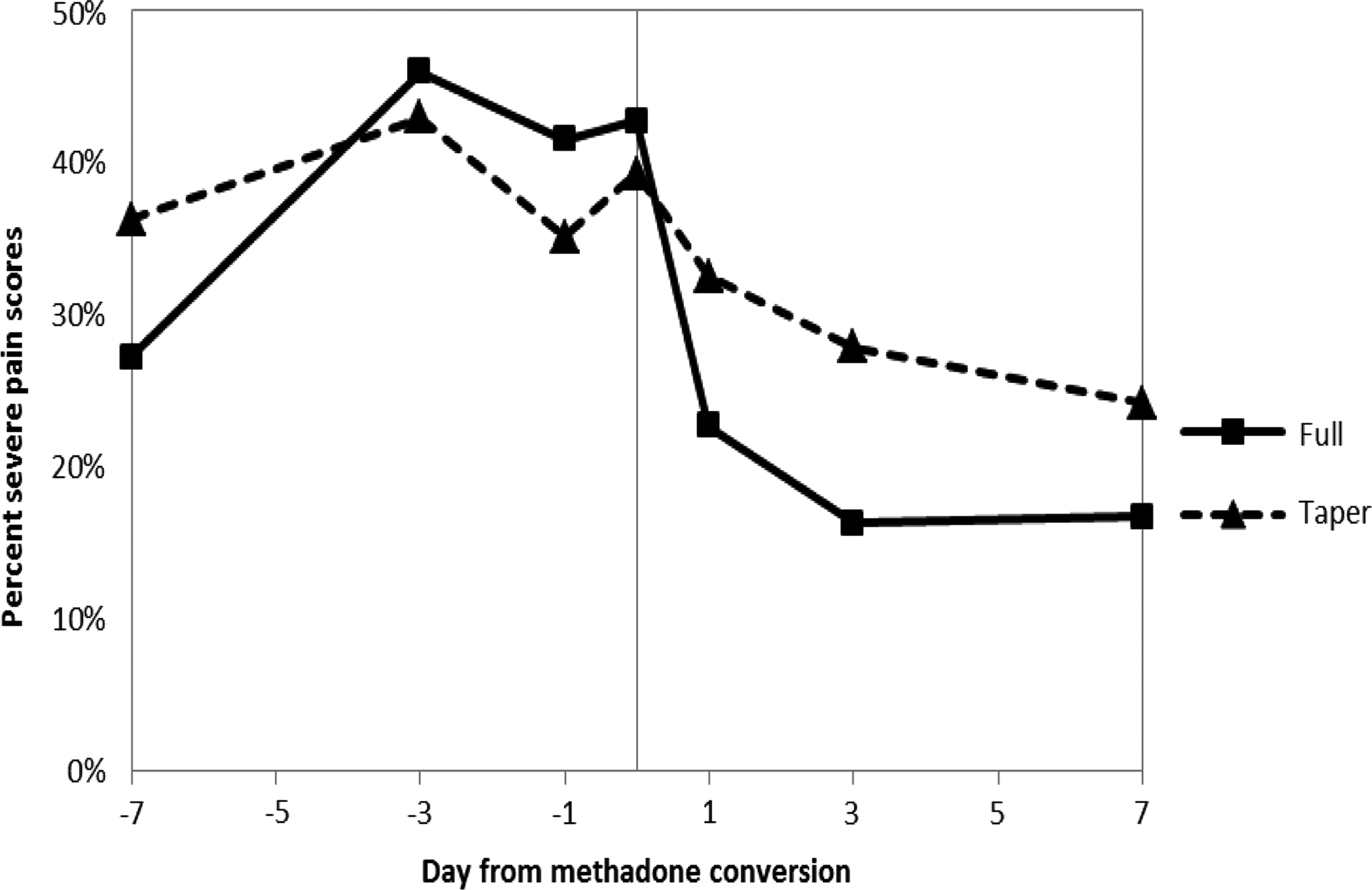
Percent severe pain scores (score ≥7) over time, for full and tapered conversion. Data reported for days −7, −3, −1, 0, 1, 3, and 7.
P value for change from week -1 to week 1.
Average of each patient's % severe pain scores, defined as ≥7, for each week.
IQR, interquartile range; MEDD, methadone-equivalent daily dose.
Discussion
We studied the opiate conversion to very-low-dose methadone and haloperidol in 43 patients with pain in the acute-care setting. The median pain scores dropped from 5 to 1 in the first week after conversion and to 0 by week 2. Significant improvements were seen for all subgroups studied, but those who had full conversion using haloperidol for breakthrough pain had greater improvements by week 1 than those with a tapered conversion using short-acting opiates as needed. In addition, those with higher initial opiate doses had more dramatic reductions in pain scores than those with lower doses, without evidence for increased pain or signs of withdrawal. Our regimen differs significantly from standard conversion guidelines, as we did not use a specific opioid conversion ratio and the median daily dose of methadone, 5 mg, was less than one-tenth of doses often used.9,25–30
Hospital pain management typically involves the use of high-dose parenteral opiates, which may lead to hyperalgesia through the pro-nociceptive NMDA pathway.1,3,4,26,31–45 Studies have shown a dose-dependent risk for opioid-related adverse events, prolonged hospital stays, and higher hospital costs.25,46 Reducing the dose of the opioid or inhibiting the NMDA pathway results in a reduction of pain and irritability.2,3,6,40,41,47,48 Methadone is a potent opioid-receptor agonist with NMDA-antagonist properties, and is often used in conversion from other opiates once hyperalgesia has occurred.6–12,49 Methadone offers the potential for large cost savings, as the direct cost of methadone is less than one-tenth the cost of typical opioids.50–52
Nonopioid medication use in the hospital has not received much attention, as opioids are considered first-line treatment for moderate to severe pain. 1 When nonopioid agents are used, they do not generally include haloperidol despite its potential NMDA-blocking effects.1,15–18,34,35,53,54 Placebo-controlled studies have indicated that haloperidol and other antipsychotic agents can significantly reduce pain.19,52 There is a potential risk for sedation, extrapyramidal side effects, and arrhythmias.55,56 However, the median daily dose of haloperidol in our study, 1.5 mg, is less than one-tenth the typical doses used, 19 and we found no evidence of adverse effects. In our study, complete conversion to methadone and haloperidol was associated with a drop of median pain score from 5 to 0, which is greater than what was seen with tapered conversion or with other methadone-conversion regimens,9,57,58 suggesting that haloperidol had a significant effect on pain control. It is possible that the combination of methadone and haloperidol has synergistic effects on pain pathways. 54
We conducted a retrospective, observational study of hospitalized patients referred for a palliative care consult who agreed to try the methadone regimen. It is possible that this group may not be representative of other hospitalized patients with pain. Our protocol involved the combined use of two medications, so it is unclear how much each drug contributed to the results. There were no reported cases of severe toxicity in our study, but larger studies with regular monitoring may be necessary to find rare events. Despite these study limitations, we believe this study presents promising results about a novel pain regimen that appears to be safe and effective. Our findings justify prospective clinical trials to explore this combination.
Footnotes
Author Disclosure Statement
No competing financial interests exist.