
Abstract
Abstract
Background:
Recent focus on palliative and end-of-life care has led medical schools worldwide to enhance their palliative care curricula.
Objective:
The objective of the study was to describe recent curricular innovations in palliative care for medical students, evaluate the quality of studies in the field, and inform future research and curricular design.
Methods:
The authors searched Medline, Scopus, and Educational Resource Information Center (ERIC) for English-language articles published between 2007 and 2013 describing a palliative care curriculum for medical students. Characteristics of the curricula were extracted, and methodological quality was assessed using the Medical Education Research Study Quality Instrument (MERSQI).
Results:
The sample described 48 curricula in 12 countries. Faculty were usually interdisciplinary. Palliative care topics included patient assessment, communication, pain and symptom management, psychosocial and spiritual needs, bioethics and the law, role in the health care system, interdisciplinary teamwork, and self-care. Thirty-nine articles included quantitative evaluation, with a mean MERSQI score of 9.9 (on a scale of 5 to 18). The domain most likely to receive a high score was data analysis (mean 2.51 out of 3), while the domains most likely to receive low scores were validity of instrument (mean 1.05) and outcomes (mean 1.31).
Conclusions:
Recent innovations in palliative care education for medical students represent varied settings, learner levels, instructors, educational modalities, and palliative care topics. Future curricula should continue to incorporate interdisciplinary faculty. Studies could be improved by integrating longitudinal curricula and longer-term outcomes; collaborating across institutions; using validated measures; and assessing higher-level outcomes including skills, behaviors, and impact on patient care.
Introduction
I
As palliative care educators advocate for scarce curricular time and select educational methods, it is imperative to identify rigorously tested curricula that can be used. Although previous reviews related to palliative care education exist, these have largely focused on the overall state of palliative care education in the United States, rather than evaluations of discrete curricula or innovations made in the field worldwide.4,6,7 Furthermore, to our knowledge there has been no systematic assessment of the quality of the evidence supporting such interventions. Therefore, we undertook a systematic literature review to inform curricular development at our own medical school, to understand recent trends in this field, and to evaluate the quality of the literature.
Methods
We conducted this systematic review in adherence with the PRISMA standards 8 as applied to a systematic review without meta-analysis. Meta-analysis was not pursued, because the literature in this area consists of heterogeneous interventions and outcomes, as well as many pilot or qualitative studies that are not amenable to this methodology.
Questions
These are the research questions we sought to answer:
• What educational interventions have recently been described to teach palliative care topics to undergraduate medical students? • What is the methodological quality of the studies in this field?
Study eligibility
We included academic articles published in the English language between 2007 and 2013. We chose this date range because a previous review in this topic area reviewed the literature through the end of 2006. 6 Articles were included if the population of interest was undergraduate allopathic medical students and if the article described the evaluation of a curriculum in a palliative care topic. Articles that described new curricula but did not include evaluation of any learner outcome were excluded.
Study identification
In collaboration with a medical librarian we designed searches of Medline via PubMed, Scopus, and Educational Resource Information Center (ERIC) databases for relevant articles. We performed iterative searches in each database to optimize the relevance and comprehensiveness of the results. We last performed the searches on January 16, 2014. The search strings used were:
Medline: ((terminal care OR “palliative care” OR “palliative medicine” OR “end of life” OR “end-of-life”) AND (education, medical, undergraduate OR “medical students”))
Scopus: ((“palliative care” OR “palliative medicine” OR “end of life” OR “end-of-life” OR “hospice”) AND (“undergraduate medical education” OR “medical students”))
ERIC: ((“palliative care” OR “palliative medicine” OR “end of life” OR “end-of-life” OR “hospice” OR “terminal illness” OR death) AND (“medical students”))
Study selection
Two authors (JD and JM) independently screened all articles, first reviewing titles and abstracts and then full texts. Conflicts were resolved by consensus. In the three instances in which a single intervention was reported in more than one article, we identified the article that provided the most complete description and excluded the others.
Data extraction
Study characteristics for each included article were summarized, including country, learner level, instructors, setting, educational modality, duration of intervention, and palliative care topics addressed.
Two authors (JD and JM) independently tabulated a Medical Education Research Study Quality Instrument (MERSQI) score 9 for all articles that included a quantitative evaluation. Disagreements between the two raters were resolved by re-review and consensus to assign the final score. The MERSQI was developed by Reed, et al. in 2007 as a measure of methodological rigor of medical education studies. The MERSQI scores studies across six domains: study design, sampling, type of data, validity of evaluation instrument, data analysis, and outcomes. These domains are further divided to yield 10 items. Each of the six domains has a maximum score of 3, giving a possible score for each study ranging from a minimum of 5 to a maximum of 18. This scoring system is summarized in the first three columns of Table 1.
Results
Trial flow
Our initial database searches identified 1167 results, and after de-duplication, 829 were found to be unique articles. After filtering the results for English language and date of publication, we reviewed the titles and abstracts of the remaining 299. Sixty-eight met our inclusion criteria based on review of titles and abstracts. Full-text review led to the exclusion of an additional 20, yielding a final sample of 48 articles (see Fig. 1).
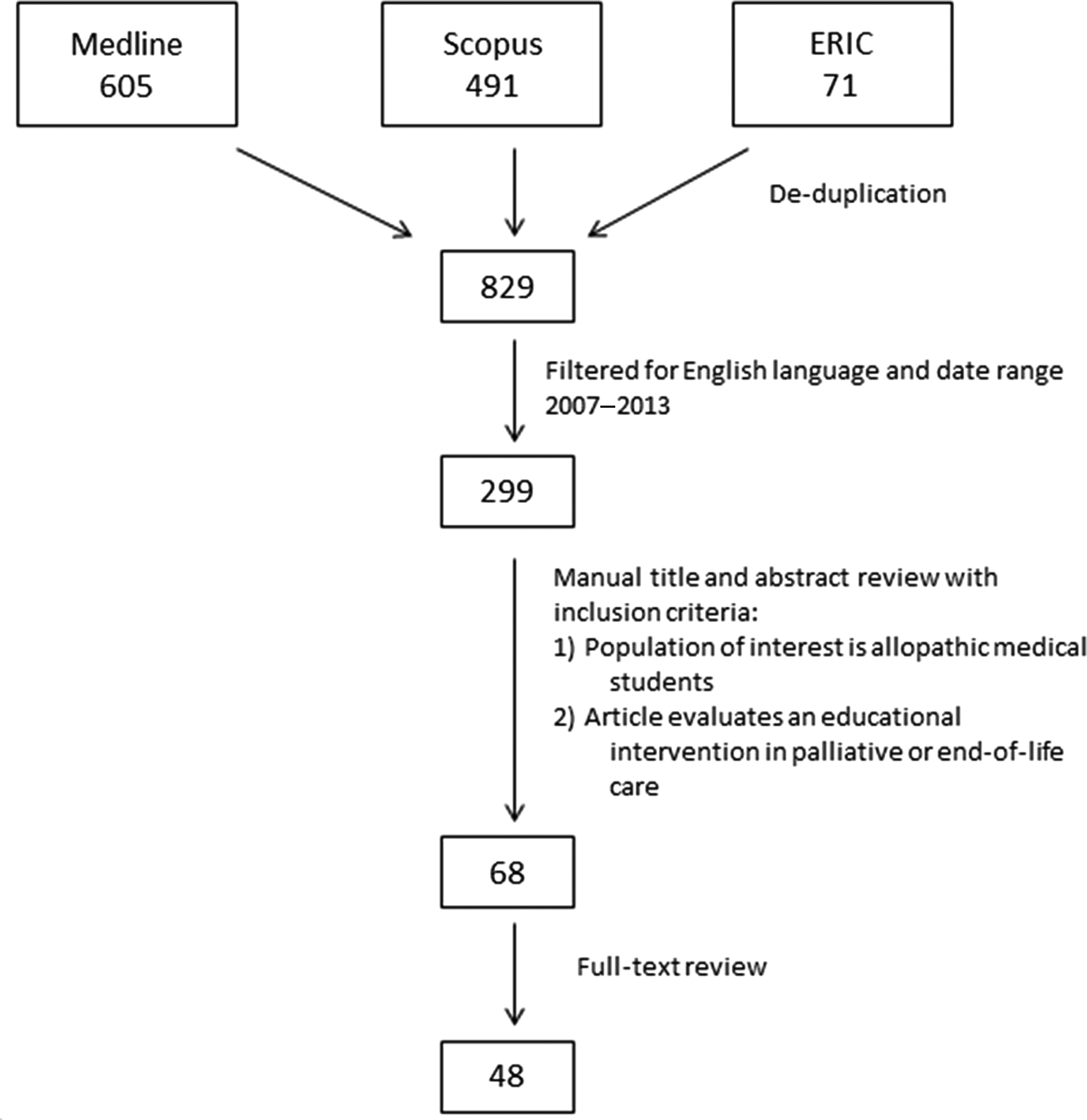
Trial flow for systematic review.
Study characteristics
The included studies describe 48 unique curricula delivered in 12 countries, which are summarized in Appendix 1: Summary of Curriculum Characteristics.10–57 Twenty-two articles were from the United States; 7 from the United Kingdom; 4 from Canada; 3 from Taiwan; 2 each from Australia, Croatia, and Germany; and 1 each from Brazil, Hungary, India, Ireland, Japan, and Poland. Educational setting was most often a mix of classroom and clinical settings (n=21, 44%). Seventeen (35%) were in a classroom setting only, 7 (15%) in a clinical setting only, and 6 (13%) included online instruction.
The targeted learners were clinical medical students (I=27, 56%), preclinical medical students (I=17, 35%), or both (n=3, 6%). Five studies (10%) delivered the intervention to medical students together with other learners, such as nursing students, social work students, pharmacy students, residents, and/or practicing health professionals.
Physicians served as instructors for 29 interventions (60%), including 19 (40%) in which the faculty included hospice and palliative medicine specialists. It was also very common to involve other health professionals as teachers, most commonly nurses or nurse practitioners (n=15, 31%), social workers (n=7, 15%), and chaplains (n=7, 15%). In 12 articles (25%) the instructors were not specified.
A variety of educational modalities were employed, including lectures (n=29, 60%), group discussion (n=27, 56%), clinical exposure, which we defined as education that takes place in a clinical setting but does not involve direct patient care responsibilities (n=14, 29%), patient care (n=13, 27%), simulation or role play (n=13, 27%), written assignment (n=12, 25%), online module (n=6, 13%), student presentation (n=6, 13%), reading assignment (n=6, 13%), multimedia (n=6, 13%), and arts activity or performance (n=2, 4%).
The curricular time spent for the educational interventions ranged from 45 minutes to 25 hours. Some articles described single teaching sessions, while others evaluated complex curricula delivered over longer periods (up to four years).
Topics within palliative care addressed by the curricula included communication (n=30, 63%), role of palliative and end-of-life care in the health care system (n=26, 54%), pain and symptom management (n=22, 46%), clinical assessment of patients (n=20, 42%), addressing psychosocial and spiritual needs (n=19, 40%), ethics and the law (n=18, 38%), interdisciplinary teamwork (n=15, 31%), and self-care (n=11, 23%). Five studies (10%) did not specify the topics covered.
Study quality
Of the 48 studies meeting the inclusion criteria, 39 included quantitative methods and were assigned MERSQI scores, while the others were solely qualitative. Table 1 summarizes the MERSQI scoring system and the results for our sample. Scores ranged from 5 to 15 (possible range 5 to 18), with a mean score of 9.9 and standard deviation of 2.7.
The most common study design was single-group pretest and posttest (n=17, 35%). However, 10 studies (21%) involved a control group, including 2 (4%) that randomized their participants.
The domain most likely to receive a high score was data analysis, with a mean of 2.51 out of 3. Twenty-four articles (50%) received the maximum possible score for both appropriateness and complexity of data analysis.
The domains that scored lowest in our sample were validity of the evaluation instrument and outcomes. The mean score for the validity domain was 1.05 out of 3, with 15 articles (31%) scoring zero points on all three items in the domain. The mean score for the outcomes domain was 1.31 out of 3. Twenty-one articles (44%) received the lowest possible score in this domain, indicating that outcomes were measured at the level of satisfaction, attitudes, perceptions, opinions, or general facts, but did not assess knowledge, skills, behaviors, or patient or health care outcomes.
Discussion
Characteristics of palliative and end-of-life care educational interventions
To inform curricular development at our own and other medical schools, we undertook a systematic literature review to describe recent curricular innovations in palliative care education for medical students. We also assessed the quality of the evidence for effectiveness of these curricula. We found that emerging approaches in the field vary widely in scope, ranging from stand-alone didactic sessions to longitudinal four-year curricula. Lecture and group discussion were the most commonly cited educational modalities. However, most interventions employed a mix of modalities, with lecture or group discussions used to prepare for, supplement, or debrief a clinical experience, simulation, or role-play.
One important pattern that emerged from our review is that palliative care curricula tend to employ a broadly interdisciplinary faculty. Of the 36 articles that specified the profession of the instructors, only 9 were taught by physicians alone. The other instructors included not only nonphysician health professionals (nurses, nurse practitioners, social workers, chaplains, psychologists, pharmacists, physical therapists, and massage therapists), but also teachers from nonmedical disciplines such as ethics, law, theology, drama, philosophy, and sociology. Given this wealth of experience in incorporating interdisciplinary faculty, the field of palliative care should serve as a model for how to incorporate nonphysician educators into medical student education to promote interdisciplinary collaboration.
One common limitation of the studies included in this review is that many of the curricula were not described in enough detail to be replicated by other educators. For some articles we were unable to ascertain even basic information such as which palliative care topics were covered or who served as the instructors. As medical educators look to the literature to design their own curricula, this is an important limitation, which likely results from the space constraints of academic journals. One way to address this would be to include online supplemental materials that provide detailed descriptions of educational objectives, content, format, and educational materials. For example, Radwany, et al. addressed this issue effectively even for their complex, longitudinal, four-year intervention. 40 Within the text of the article they provided a broad curriculum map and general description of the curriculum format and content. They then included two additional files, which contained detailed, replicable descriptions of the components that they considered to be “cornerstones” of their curriculum: a mandatory hospice experience and a case-based group discussion prior to graduation.
Another limitation of the sample is the narrow scope of many of the curricula, most of which evaluate the immediate effect of a single teaching session or circumscribed clinical experience. Because the field of palliative care encompasses such breadth of content that spans many medical specialties, more studies should evaluate palliative care curricula longitudinally as students engage the topics within the context of their general medical curriculum. For example, Morrison, et al. used a waitlist-control crossover design to demonstrate improvements in students' knowledge and attitudes following a palliative care curriculum that spanned the entire third year of medical school. 34 Even for smaller-scale interventions, educators should assess the long-term retention of learning objectives whenever possible. For example, Stevens, et al. demonstrated that students who participated in their pain management curriculum performed better on pain management domains of a clinical skills exam 1.5 years later. 48
Study quality
In recent years, increasing emphasis has been placed on improving the methodological rigor of medical education research. Cook and Bordage have found that many essential elements of scientific reporting are frequently absent from articles describing medical education experiments. 58 The MERSQI was developed by Reed and colleagues in 2007 as a measure of rigor for experimental studies in medical education, and has been shown to correlate well with expert quality ratings, number of citations, and journal impact factor. 9 We used this instrument to assess the quality of our sample of recent studies in palliative care.
The studies in our sample had a mean MERSQI score of 9.9 (standard deviation 2.7, range 5–15). This result is quite similar to the mean of 9.95 (standard deviation 2.34, range 5–16) from the first reported MERSQI sample, which was a broad, interdisciplinary sample of 210 medical education studies published between 2002 and 2003. 9 More recently, systematic reviews of medical education in topic areas unrelated to palliative care that utilized MERSQI have reported mean scores ranging from 9.0 to 11.4.59–66 Overall, this suggests that palliative care education studies are of similar methodological quality to other medical education studies.
We found that within our sample most studies received high scores in the domain of data analysis. This indicates that the authors go beyond descriptive analysis to assess statistical significance of the effectiveness of their intervention and that the data analysis methods used are appropriate. Another area of strength was the “response rate” item within the sampling domain, indicating that the authors' conclusions are based on a representative sample of the students exposed to the intervention.
However, also within the sampling domain, the item “number of institutions studied” was the MERSQI item most likely to receive the lowest possible score. In fact, only one study in our sample implemented and evaluated their intervention with students from more than one institution. This aspect of study quality has important implications for generalizing study findings, and future researchers should endeavor to collaborate with other institutions to test the intervention in multiple settings or with multiple student populations. While multiple-institution collaboration is extremely difficult for implementing longitudinal, integrated curricula, it would be feasible for short-term, discrete interventions. For example, Tsai, et al. were able to implement a four-hour curriculum including a lecture, a hospice patient visit, communication skills practice, and group discussion with students in attendance from three local medical schools. 52
Because trainees' self-assessments of their skills may not predict the patient's assessment of the interaction, it is important that educators measure behavioral and patient outcomes, rather than relying solely on student assessments to demonstrate the effectiveness of a curriculum. However, in our sample the vast majority of studies (35 out of 39, 90%) measured outcomes either at the level of satisfaction, perceptions, and attitudes (usually measured by self-assessment on a Likert scale) or at the level of knowledge acquisition (usually measured by multiple-choice examination). Three studies (8%) measured student behaviors, with two measuring behaviors in a simulated patient encounter and one measuring self-reported communication behaviors. Only one study (3%) assessed a patient outcome: Green and Levi measured patient satisfaction after a medical student assisted the patient in filling out an advance directive. 22 Because many of the educational interventions being studied already involve direct patient care, it would likely be feasible in future studies to incorporate patient outcomes into the evaluation.
Finally, validity of the evaluation instrument was a clear weakness in study quality. Fifteen studies reported no attempt to establish validity of their instrument regarding internal structure, content, or relationship to other variables. Instead, most studies relied upon surveys created by the authors, which did not undergo any formal development process. One positive example in this domain was the study by Chang, et al., who developed their instrument to measure changes in palliative care knowledge and attitudes before and after a five-day course. They began with a literature review, piloted the initial form of the instrument, retained only the most reliable items for the final instrument, and calculated the relationship between attitude scores, knowledge scores, and demographic data. 13
Limitations
One limitation of this review is that our methods only assessed the quality of the subset of studies that included quantitative analysis. In the fields of medical education and palliative care, qualitative analysis of data such as focus groups, interviews, open-answer survey responses, and written reflections form the core of many studies. In our sample, 9 of the 48 studies reported qualitative data alone, and another 13 studies used mixed quantitative and qualitative methods. Our review does not speak to the methodological rigor of these qualitative analyses.
Another limitation of our review is that our database searches did not include items published in peer-reviewed repositories of educational products, such as MedEdPortal, which are often used for reporting and dissemination of curricula across medical schools.
Conclusions
Many recent innovations have been made in the field of palliative care education for medical students, representing a variety of learner levels, settings, educational modalities, and topics. One strength of palliative care education is the incorporation of interdisciplinary faculty, which should serve as a model for interdisciplinary collaboration in other parts of the medical curriculum. Future innovations in the field should endeavor to collaborate across multiple institutions, integrate more longitudinal curricula and study longer-term outcomes, make use of better-validated measures of effectiveness, and assess higher-level outcomes including skills, behaviors, and impact on patient care.
Footnotes
Acknowledgments
The authors would like to thank Lauren Maggio for her guidance regarding systematic review methodology. This work was funded by the Medical Scholars program at Stanford University School of Medicine.
Author Disclosure Statement
The authors have no conflicts of interest to disclose.
| Study | Country | Learner level | Instructors | Setting | Educational modalities | Duration | Topics a | MERSQI Score b |
|---|---|---|---|---|---|---|---|---|
| Auret and Starmer 2008 | Australia | Clinical | HPM physicians, non-HPM physician, nurses, pharmacist | Classroom | Group discussion, simulation | 2 hours | 1, 2, 3, 6 | 7 |
| Bell and Crawford 2011 | United Kingdom | Preclinical | Physician, nurse, ethicist, theologian, attorney | Classroom | Lecture, group discussion, written assignment, student presentation, online module, simulation, clinical exposure | 20–25 hours (over 12 weeks) | 5, 6, 7 | 7.5 |
| Brownfield and Santen 2009 | United States | Clinical | Unspecified | Clinical, classroom | Lecture, group discussion, patient care | 1 week | 3, 6 | 10.5 |
| Chang, et al. 2009 | Taiwan | Preclinical | HPM physicians, nurse, social workers, chaplain | Clinical, classroom | Lecture, group discussion, clinical exposure | 1 week | 4, 5, 6, 7 | 14 |
| Chittenden, et al. 2013 | United States | Clinical | None | Online | Online module | 45 minutes | 2 | 14 |
| Corcoran, et al. 2013 | United States | Clinical, preclinical | Nurses, social workers, chaplains | Clinical | Clinical exposure | 4 hours | Unspecified | Q |
| Dando, et al. 2012 | United Kingdom | Clinical, also nursing, physical therapy, and occupational therapy students | Physician, nurse, physical therapist | Clinical | Group discussion, patient care | 3 weeks | 7 | 5 |
| Ellman, et al. 2009 | United States | Clinical | HPM physician, non-HPM physicians | Clinical, classroom | Written assignment, student presentation, patient care | Variable | 1, 2, 3, 7, 8 | 7 |
| Ellman, et al. 2012 | United States | Clinical, also nursing, social work, and chaplaincy students | Physician, nurse, social worker, chaplain | Classroom, online | Group discussion, online module, simulation | 2 hours | 1, 2, 3, 4, 6, 7 | 10.5 |
| Gadoud, et al. 2013 | United Kingdom | Clinical | Unspecified | Clinical | Patient care | Unspecified | Unspecified | Q |
| Goldberg, et al. 2011 | United States | Clinical | HPM physicians, nurse, social worker, chaplain, massage therapist | Clinical, classroom | Lectures, group discussion, patient care | 1 week | 2, 3, 4 | 10 |
| Goldsmith, et al. 2011 | United States | Clinical | HPM physician, non-HPM physicians, nurses, social workers, chaplains, psychologists, patients | Clinical, classroom | Lectures, multimedia, patient care | 12 hours | 1, 2, 3, 6, 7 | Q |
| Green and Levi 2011 | United States | Preclinical | None | Clinical, online | Online module, patient care | Variable | 2, 5 | 15 |
| Hall, et al. 2011 | Canada | Clinical, also interprofessional students | Physicians, nurses, interdisciplinary health professionals | Classroom | Group discussion, simulation | 3 hours | 1, 2, 3, 4, 5, 7 | 8 |
| Head, et al. 2012 | United States | Clinical | Unspecified | Clinical | Written assignment, patient care | 1 week | 2, 3, 8 | Q |
| Hegedus, et al. 2008 | Hungary | Preclinical, also health care professionals | Unspecified | Classroom | Lectures | Unspecified | 2, 3, 4, 6 | 11 |
| Jacoby, et al. 2011 | United States | Clinical | Unspecified | Clinical | Lecture, reading assignments, written assignment, patient care | 1 week | 1, 2, 6, 7 | Q |
| Jeffrey, et al. 2012 | United Kingdom | Clinical and preclinical | HPM physicians, drama educators | Classroom | Drama performance, group discussion, reading assignment, written assignment | 2 weeks | 2 | Q |
| Kato, et al. 2011 | Japan | Clinical | Unspecified | Classroom | Lecture | 1 hour | 3, 6 | 10 |
| Kaufert, et al. 2010 | Canada | Preclinical | Physicians, patients | Classroom | Lecture, group discussion | 4 hours | 4, 5 | Q |
| Kitzes, et al. 2008 | United States | Clinical | HPM physicians, non-HPM physicians | Classroom | Group discussion | 4 hours | 1, 2, 3, 4, 5, 6, 8 | 8.5 |
| Korzeniewska-Eksterowicz, et al. 2012 | Poland | Clinical | Physicians, psychologist | Classroom | Lecture, group discussion | 10 hours | 1, 2, 3, 4, 5, 6, 8 | 7 |
| Lubimir and Wen 2011 | United States | Clinical | Unspecified | Classroom | Group discussion, written assignment, simulation | 3 hours | 2, 4, 5 | 6 |
| Mason and Ellershaw 2010 | United Kingdom | Clinical | Unspecified | Clinical, classroom | Lecture, group discussion, student presentation, patient care | 2 or 4 weeks | 2, 5 | 10.5 |
| Morrison, et al. 2012 | United States | Clinical | HPM physicians, interdisciplinary health professionals | Clinical, classroom, online | Lectures, group discussion, written assignment, student presentation, online module, clinical exposure | 8 hours (over 46 weeks) | 1, 4, 6, 7 | 13 |
| Murtagh, et al. 2012 | Ireland | Preclinical | HPM physicians | Clinical, classroom | Lecture, reading assignments, student presentation, clinical exposure | 15 hours (over 10 weeks) | 1, 4, 6, 7 | 11 |
| Nwosu, et al. 2013 | United Kingdom | Clinical | Physician | Online | Written assignment | 11–59 minutes | Unspecified | 7 |
| Oliver and Jezek 2013 | Croatia | Preclinical | HPM physician | Classroom | Lectures, group discussion, multimedia | 3 days | 1, 2, 3, 4, 6 | 7.5 |
| Philip and Remblabeevi 2010 | India | Preclinical | Nurses, hospice volunteers | Clinical, classroom | Lecture, group discussion, simulation, multimedia, clinical exposure | 3 days | 2, 6, 7 | 6 |
| Pinheiro, et al. 2010 | Brazil | Unspecified medical students, also residents | Not specified | Clinical | Reading assignments, written assignment, patient care | Variable | Unspecified | Q |
| Radwany, et al. 2011 | United States | Clinical and preclinical | Physicians, interdisciplinary health professionals | Clinical, classroom | Lectures, group discussion, simulation, written assignments, clinical exposure | 4 years | 1, 2, 3, 4, 5, 6, 7, 8 | 6.5 |
| Sanchez-Reilly, et al. 2007 | United States | Clinical | HPM physicians, nurses, social workers, chaplains, psychologists, patients | Clinical, classroom | Lectures, written assignments | 8 hours (over 4 weeks) | 1, 2, 6, 7, 8 | 13 |
| Schillerstrom, et al. 2012 | United States | Preclinical | HPM physicians, psychiatrists, psychologists, interdisciplinary health professionals | Classroom | Lecture, group discussion | 4 hours | 6 | 9 |
| Schulz, et. al. 2013 | Germany | Clinical | Unspecified | Clinical, classroom | Lectures, group discussion, simulation, written assignment, clinical exposure. | 23 hours (over 2 semesters) | 1, 2, 3, 6, 7, 8 | 10.5 |
| Shih, et al. 2013 | Taiwan | Preclinical | HPM physicians, interdisciplinary health professionals | Clinical, classroom | Lectures, simulation, multimedia, clinical exposure | 1 day | 1, 2, 5, 7 | 13 |
| Silk, et al. 2009 | United States | Clinical | Unspecified faculty, nurses | Clinical, classroom | Lecture, group discussion, simulation, multimedia, clinical exposure | 7.5 hours | 2, 6 | 9 |
| Sorta-Bilajac, et al. 2007 | Croatia | Preclinical | Physician, ethicist, theologian, philosopher, sociologist, attorney | Classroom | Lectures, multimedia, written assignment, student presentation | 7.5 hours | 4, 5, 6 | 10.5 |
| Stecho, et al. 2012 | Canada | Preclinical | Nurse, hospice volunteers | Clinical, classroom | Lectures, patient care | 30–40 hours | Unspecified | 10 |
| Stevens, et al. 2009 | United States | Preclinical | HPM physicians, non-HPM physicians, nurses | Classroom | Lectures, group discussion, simulation | 10 hours | 1, 2, 3 | 14 |
| Tai, et al. 2013 | Australia | Clinical | Unspecified | Clinical, classroom | Lectures, group discussion, patient care | 1 week | 3, 4, 5 | 12 |
| Tan, et al. 2013 | Canada | Clinical | None | Online | Online module | Variable | 1, 3, 4 | 11 |
| Tchorz, et al. 2013 | United States | Clinical | Non-HPM physicians, ethicist | Classroom | Group discussion, multimedia, simulation | 2 hours | 1, 2, 3, 4, 5 | 11 |
| Tsai, et al. 2008 | Taiwan | Preclinical | HPM physicians | Clinical, classroom | Lecture, group discussion, reading assignment, clinical exposure | 4 hours | 2, 5, 6 | 14 |
| von Gunten, et al. 2012 | United States | Clinical | HPM physicians, nurses, social workers, chaplains | Clinical, classroom | Lectures, simulation, patient care | 4 days (over 4 weeks) | 1, 2, 3, 4, 5, 6, 7, 8 | 13 |
| Weber and Mascagna 2008 | United States | Preclinical | HPM physician | Clinical, classroom | Arts activity or performance, group discussion, written assignment, student presentation, clinical exposure | Unspecified | 6 | Q |
| Weber, et al. 2011 | Germany | Preclinical | HPM physicians | Clinical, classroom | Lecture, group discussion, clinical exposure | 1.5 hours | 4, 6, 8 | 9.5 |
| Wechter, et al. 2013 | United States | Preclinical | HPM physicians | Clinical, classroom | Group discussion, reading assignments, clinical exposure | 4 hours | 2, 4, 5, 6, 8 | 9.5 |
| Yardley, et al. 2013 | United Kingdom | Clinical | Unspecified | Classroom | Lecture, group discussion, simulation | 7 hours | 1, 2, 3, 5, 6 | 7 |
Palliative and End-of-Life Care topics are listed only if they were specifically reported in the article. Coding is as follows: 1=patient assessment, 2=communication, 3=pain and symptom management, 4=addressing psychosocial and spiritual needs, 5=ethics and the law, 6=role in the health care system, 7=interdisciplinary teamwork, 8=self-care.
Q indicates that the study was qualitative, and did not receive a MERSQI score.
HPM, hospice and palliative medicine; MERSQI, Medical Education Research Study Quality Instrument.