
Abstract
Abstract
Background:
The use of physical restraints in dying patients may be a source of suffering and loss of dignity. Little is known about the prevalence or predictors for restraint use at end of life in the hospital setting.
Objective:
The objective was to determine the prevalence and predictors of physical restraint use at the time of death in hospitalized adults.
Methods:
Secondary analysis was performed on data from the “Best Practices for End-of-Life Care for Our Nation's Veterans” (BEACON) trial conducted between 2005 and 2011. Medical record data were abstracted from six Veterans Administration Medical Centers (VAMCs). Data on processes of care in the last seven days of life were abstracted from the medical records of 5476 who died in the six VAMCs. We prospectively identified potential risk factors for restraint use at the time of death from among the variables measured in the parent trial, including location of death, medications administered, nasogastric tube, intravenous (IV) fluids, family presence, and receipt of a palliative care consultation.
Results:
Physical restraint use at time of death was documented in 890 decedents (16.3%). Restraint use varied by location of death, with patients in intensive settings being at higher risk. Restraint use was significantly more likely in patients with a nasogastric tube and those receiving IV fluids, benzodiazepines, or antipsychotics.
Conclusions:
This is the first study to document that one in six hospitalized veterans were restrained at the time of death and to identify predictors of restraint use. Further research is needed to identify intervention opportunities.
Introduction
T
Clinical rationales for physical restraint use focus on protection of the patient and include concerns about disruption of necessary therapy, infliction of harm to oneself or others, and occurrence of falls. 3 However, evidence suggests that physical restraints do not have these beneficial effects.4,5 In fact, restraint use has been associated with negative patient outcomes, including increased risk of delirium and agitation,6,7 pressure ulcers,8,9 falls,5,8,10 contractures,8,9 lengthened hospital stay, 11 and death.9,12 Often, their use is a source of moral distress for family members and professional staff.13,14 Older adult patients generally report being traumatized and depersonalized by the use of physical restraints, and in some studies family members expressed similar concerns.15,16
Although physical restraints have been utilized in patient care for more than a century, 17 little is known about the prevalence of their use among actively dying patients in acute care settings. In 1986 Frengley and Mion, et al. reported that restrained patients accounted for nearly 50% of deaths among geriatric inpatients during the study's observation period, and attributed this finding to an association between restraint use and “severity of illness.” 18 A 1998 chart audit study in two hospitals found that one-fifth of decedents observed were physically restrained in the last two days of life. 19 In intervening years, one would anticipate that regulatory forces and growing awareness of palliative and comfort care principles would reduce the likelihood of restraint use at the end of life. However, no subsequent studies were identified that reported on this issue. A direct observation study of processes of care in U.S. hospitals showed physical restraints were used in an average of 50 patient days out of every 1000; 20 however, numbers of patients who died in restraints were not reported.
A number of variables have been associated with the use of physical restraints in hospitalized patients, including patient factors, staffing factors, and setting factors.3,9,21–23,24 Research consistently shows that physical restraint use is related to the site of care, with the highest rates reported in adult intensive care units (ICUs).20,25 Since one in five patients die in the ICU, 26 it is likely that a significant proportion of patients could be spending their last days of life in physical restraints.
Given the limited information about this potential source of suffering in terminally ill patients, we sought to describe the prevalence and predictors of restraint use at the time of death. Identifying potentially modifiable factors may indicate potential targets for development of interventions to reduce restraint use in this vulnerable population.
Methods
We conducted a secondary analysis of data from the “Best Practices for End-of-Life Care for Our Nation's Veterans” (BEACON) trial, which is described elsewhere.27,28 Briefly, BEACON was a pragmatic, multisite implementation trial to evaluate the impact of an educational intervention on end-of-life care processes in six VA Medical Centers (VAMCs). The intervention included training inpatient staff to identify actively dying patients and to implement home hospice best practices in the acute care setting. Training was supported with educational resources, including pocket card decision support tools and an electronic comfort care order set. The intervention also facilitated policy changes to ensure availability of palliative care clinical interventions. The study was approved by the institutional review boards of the coordinating site and all participating clinical sites.
Sample and cata collection
During the study period (January 2005 through February 2011), medical records were abstracted for 6066 veterans who died in the six participating VAMCs during the pre- or post- intervention periods. Using a chart abstraction tool designed for the study, a registered nurse derived data from the decedents' electronic and paper records on the processes of care during the last seven days of life. Interrater reliability for the primary outcome measures was established between the chart abstractor and the director of palliative care at the coordinating center. For the purpose of this analysis we excluded the records of 590 veterans who died within a nursing home unit, leaving a sample of 5476 decedent records.
From the variables available in the database we selected potential predictors based on literature review and clinical experience. Predictors included location of death, medications administered (e.g., benzodiazepine, opioids, etc.), presence of nasogastric tube, IV fluids infusing, family presence at time of death, and palliative care consultation during the last seven days of life. Restraint use at time of death was operationalized as the documentation of an active order for restraints present in the electronic medical record at the moment of death. VAMC policy requires an active order for use of physical restraints. Demographic data (age, gender, race/ethnicity, and income) were obtained from the VA National Datasets.
Statistical analysis
Data from the six sites were pooled. To account for the clustered nature of the observations (patients nested within hospitals), generalized estimating equations (GEE) were used. 29 Initial statistical analyses estimated the association between the restraint use and the hypothesized predictors: location of death, medications administered, presence of nasogastric tube, IV fluids infusing at time of death, family presence, and palliative care consultation. For these preliminary analyses, we controlled for other variables that also might explain the variation in restraint use: the year of study, whether the observation was made before or after the intervention, and whether the patient had a diagnosis of anxiety or agitation. Careful adjustment of the degrees of freedom was conducted to account for the known issues of using GEE with small numbers of clusters.29–33
All predictors that achieved a significance level of 0.10 in the initial analyses were included in a multivariable modeling approach. Specifically, to account for the correlation among the predictors and to provide a final model, an iterative backward elimination approach was used in which the predictor with the largest p-value was removed. This iterative process continued until all remaining predictors reached a significance level of 0.05. Data were analyzed using statistical software SAS (SAS version 9.3, SAS Institute., Cary, NC).
Results
Characteristics of the sample
The characteristics of the sample are presented in Table 1. The sample was predominantly male (98%) and white (58%) or African American (31%), with a mean age of 70.4 years. The most common terminal conditions were cancer (30%) and heart disease (20%). In 890 cases (16.3%), the patient was in restraints at the time of death; 65% of patients who died in restraints were in an intensive care setting (ICU or surgical ICU), representing 24% of all ICU patients.
Between groups p-values not meaningful because parent study was a stepwedge design cluster analysis with data influenced by site and time in a manner that cannot be adequately controlled for in this analysis.
Predictors of physical restraint use
Bivariate analyses of predictors of restraint use at the time of death are presented in Table 2 and depicted in a forest plot in Figure 1. Bivariate analyses demonstrated a significant association between restraint use at the time of death and the ICU location of death; presence of a nasogastric tube; IV fluids; and administration of benzodiazepines, antipsychotics, or corticosteroids. Factors negatively associated with restraint use at the time of death were receiving a palliative care consultation and administration of death rattle medications. Opioid administration and family presence were not associated with restraint use.
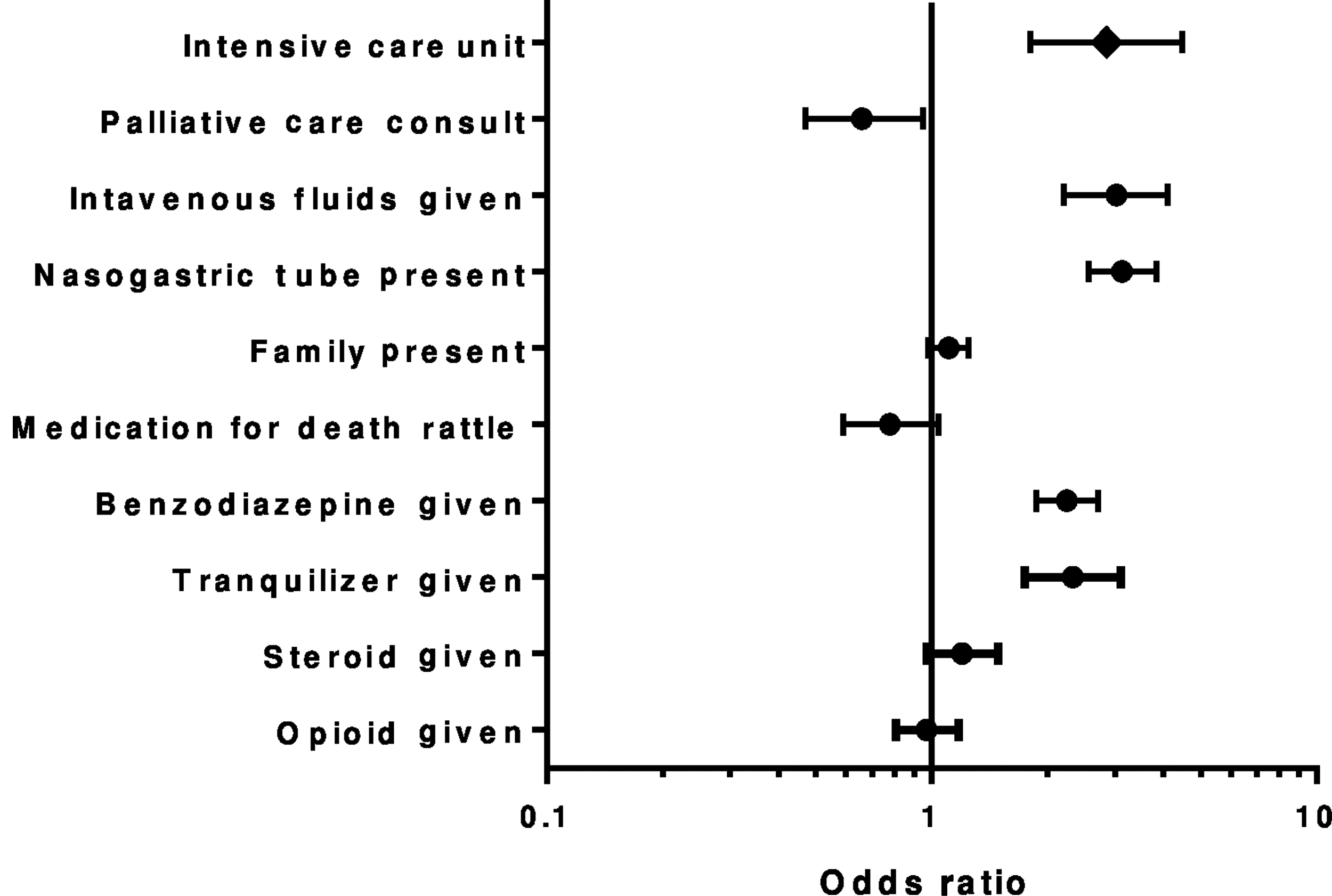
Forest plot of odds ratio for restraint use with exposure to variable.
All models controlled for year of observation, intervention period, and presence of anxiety or agitation.
In the final multivariable model, ICU location of death, nasogastric tube, IV fluids, and administration of an antipsychotic or benzodiazepine remained significantly associated with restraints (see Table 3).
All models controlled for year of observation, intervention period, and presence of anxiety or agitation.
Discussion
The results of this analysis show that one in six veterans who died in the inpatient setting were restrained at the time of death. Restraint use was associated with presence of a nasogastric tube, IV fluids, use of an antipsychotic or benzodiazepine medication, and death in an intensive care setting.
Invasive medical treatments like nasogastric tubes and IV fluids previously have been reported to be associated with agitated and disruptive behavior. 34 While these interventions may have a role in symptom management, other, less-intrusive palliative management strategies often are available, such as medical management of intestinal obstruction and sublingual medication administration. The use of nasogastric tubes and IV lines may reflect family preference for life-sustaining treatments or may represent staff or family lack of awareness that the patient's death may be imminent.
There are a number of plausible explanations for the association between the use of restraints and use of antipsychotics and benzodiazepines at end of life. First, these medication classes have been associated with the development and perpetuation of delirium and disruptive behaviors in older adults,35,36 which can lead to physical restraint use. Second, these medications can be indicated to manage terminal delirium; therefore the association may reflect the appropriate management of delirium. 37 And third, it is possible that these medications were a component of a prehospitalization management plan treating preexisting disruptive behaviors that invariably worsen in the hospital and decline in health and function. The study design did not allow us to evaluate whether some proportion of the decedents in this study were “appropriately” restrained to avoid harm to self and others when less-invasive interventions had failed.
Our finding that patients in an intensive care unit were 1.7 times as likely as other hospitalized patients to be restrained at time of death is consistent with previous studies demonstrating higher prevalence of restraint use in intensive settings. With 22% of deaths occurring in intensive settings, ICU admission has been likened to a “therapeutic trial” of maximal support, with a tradeoff in compromised quality of life as a potentially acceptable risk. 38 ICU therapies that could be disrupted by an agitated patient, such as ventilator support, arterial lines, IV lines, nasogastric tubes, and bladder catheterization, may contribute to the rate of restraint use. If the “therapeutic trial” of ICU care is judged to be not effective or the burden of treatment greater than the benefit, prompt discontinuation of burdensome and iatrogenic harmful interventions should be insured with possible transfer from ICU to a setting more focused on comfort and support and that provides better access for family at the end of life. The proposed Quality Indicators for End of Life Care in the Intensive Care Unit do not address these issues explicitly, nor is the use of physical restraints at the end of life addressed in the National Quality Forum consensus report on preferred practices for palliative care. 39
Factors that were not associated with restraint use included palliative care consultation, an active order for opioid medication, and family presence. Our initial hypothesis was that these factors would have lessened restraint use. In the bivariate analysis, patients with a palliative care consultation were less likely to have physical restraints at end of life, but this association became nonsignificant in the multivariable analysis. This finding may encourage palliative care consultation teams to routinely review for restraint use and use this as an opportunity in consultation to stress alternative approaches to delirium prevention and management including discontinuing burdensome therapies, especially in the imminently dying patients. 40
Regarding opioid use, the relationship between opioid medications and restraint use is not clearcut. For example, poor pain management can manifest as agitated behavior. 41 However, it is also the case that opioids might be withheld in an effort to manage agitation for fear of worsening the behavior. The complexity of situations where opioids are provided or withheld at life's end can make it difficult to clarify any relationship that might exist between restraint use and opioid use.
The lack of association between family presence and restraint use was surprising. We expected that family members would find the use of restraints objectionable in a dying loved one and would advocate for their discontinuation. However, family members may not be empowered sufficiently to question medical and nursing interventions. The literature related to family response to restraint use is mixed. Some family members perceive restraint use as necessary and acceptable for care plan adherence.16,42 Family and provider education about alternatives to using restraints, such as discontinuing invasive interventions, may result in less restraint use at end of life.
Generalizability of these findings may be limited due to the disproportionately male sample and the unique VA culture and processes of care that may differ from other health systems with regard to the use of restraints. Furthermore, we were limited to variables collected in the parent study, and our examination of predictors of restraint use is not exhaustive. For example, nursing practices, staffing patterns, and training may have a significant influence on the use of physical restraints. We did not have access to these data. Finally, chart abstraction may underestimate the use of restraints, affecting our prevalence estimate, which may be higher than the 16.3% identified in this sample.
The evidence base does not currently support recommendations for systematic changes to reduce the use of restraints in dying patients. Data is limited that supports effectiveness of nursing education interventions to reduce restraint use in the acute care setting. 43 One initial step, however, is to raise awareness of restraint use at the end of life as a negative outcome that may result from extending intensive life-supporting therapies.
Conclusions
This study highlights a number of issues meriting further investigation. As we seek to operationalize dying with dignity in the ICU or acute care setting, 44 optimized end-of-life care would ensure comfort through active symptom identification and management, discontinuation of unhelpful therapies, and implementation of active management of terminal delirium without the need for the use of restraints. It is disconcerting that in this study more than one in six dying patients were restrained at the time of death. Our analysis, however, could not identify how frequently end-of-life restraint use may have been appropriate, necessary, and consistent with the patient/health care agent's treatment goals. Guidelines and the literature underscore alternatives to restraint use in hospitals, particularly ICUs, and our findings suggest that dying patients are an important target population for the development of interventions and education to reduce restraint use.
Footnotes
Acknowledgments
This research was supported by a merit review grant from the Department of Veterans Affairs, Veterans Health Administration, Office of Research and Development, Health Services Research and Development Service (IIR 03-126 “Intervention to Improve Care at Life's End in VA Medical Centers;” PI: KL Burgio, Co-PI: FA Bailey) and the VA Birmingham/Atlanta Geriatric Research, Education and Clinical Center. Dr. Dionne-Odom is a postdoctoral fellow supported by the UAB Cancer Prevention and Control Training Program (5R25CA047888).
The authors thank the participating VA Medical Centers, their site principal investigators, and their palliative care teams for their roles in implementing the BEACON trial: Anna D. Senseney, MD and John Painter, PhD (site principal investigators), Karen Lukacs, RN, APN, and the palliative care team at the Ralph H. Johnson VAMC, Charleston, South Carolina; Theodore M. Johnson II, MD, MPH (site principal investigator), Adam Herman, MD, Orania Tigaieru, MD, Donna Lewis, CRNP, and the palliative care team at the Atlanta VAMC, Decatur, Georgia; Kathlyn Sue Haddock, RN, PhD (site principal investigator), Debra Layer, CRNP, and the palliative care team at the William Jennings Bryan Dorn VAMC, Columbia, South Carolina; Thomas Hartney, MD (site principal investigator), Michael Willoughby, MD, and the palliative care team at the Charlie Norwood VAMC, Augusta Georgia; Leslie Pennypacker, MD (site principal investigator) and the palliative care team at the Malcom Randall VAMC, Gainesville, Florida; and Jessie Spencer, MD (site principal investigator) and the palliative care team at the G. V. Sonny Montgomery VAMC, Jackson, Mississippi.
Author Disclosure Statement
The views expressed in this article are those of the authors and do not necessarily reflect the position or policy of the Department of Veterans Affairs or the U.S. government.
No competing financial interests exist.