
Abstract
Abstract
Background:
Palliative sedation (PS) can be classified as either continuous or intermittent. Continuous PS is most commonly used in end-of-life care, while no specific indication for intermittent PS exists.
Case Presentation:
Here we describe two cases of refractory severe cancer pain with psychological anguish that were controlled successfully by intermittent IPS for the long time. One patient complained of refractory severe cancer pain and insomnia. The other patient had uncontrollable pain and delirium, whose sufferings were relieved by intermittent PS.
Case Management and Outcome:
Intermittent PS was offered to the cases every night-time with family member/patient's consent. After providing intermittent PS, cancer pain decreased to mild intensity and psychological symptoms were significant improved simultaneously with patients awake during day time.
Conclusions:
Palliative PS may stop vicious cycle of physical and psychological distress in terminal cancer patients. Furthermore, intermittent type of PS could keep patients consciousness alert during day time and may be performed repeatedly for the long time.
Introduction
P
PS can be divided into continuous and intermittent sedation. Although PS usually refers to continuous sedation of a patient until death, intermittent (respite) sedation may be considered in selected cases. 4 With intermittent palliative sedation (IPS), patients are sedated temporarily and then awakened after a predetermined time to assess whether refractory symptoms have improved. However, no specific criteria exist for the optimal time and indications of IPS.
Most cancer pain can be successfully treated with pharmacological and/or nonpharmacological interventions. However, in some cases, cancer pain may remain severe and intractable despite aggressive efforts. 6 Uncontrolled cancer pain is a multidimensional syndrome associated with other physical symptoms, depression, insomnia, and decreased quality of life. 7 Notably, unrelieved cancer pain can disturb sleep, and poor sleep can worsen pain states. 8 Controlling cancer pain and sleep disturbance with intermittent sedation may break the vicious cycle of distress in terminal cancer patients with refractory pain. 9
Here we report two cases of severe cancer pain with psychological symptoms that were controlled successfully by long-term IPS. The current study was approved by the institutional review board of the Gyeongsang National University Hospital.
Case 1
A 46-year-old woman with rectal cancer metastatic to multiple bones was admitted to the inpatient hospice unit with severe pelvic pain—8/10 on the numeric rating scale (NRS) during rest and 10/10 with movement. Her Karnofsky performance status was 30. She had been diagnosed with rectal cancer three years before and had undergone low anterior resection. Unfortunately, the rectal cancer recurred in the lung and bone, and the patient received multiple cycles of irinotecan- and oxaliplatin-based chemotherapy with no response. She had been under best supportive care for three months. The pelvic pain was described as dull or aching in the pelvis which was aggravated by movement. Computed tomography (CT) revealed multiple metastatic bone lesions in her pelvic bones (see Fig. 1). She had received various treatments to control her severe pain, including high doses of multiple opioids, radiotherapy, and epidural nerve blocks. High doses of oxycodone, hydromorphone, morphine, and fentanyl were given sequentially for pain control (see Fig. 2). The morphine equivalent daily dose (MEDD) increased from 180 mg/day up to 900 mg/day with no relief of her pain. Various adjuvant pharmacologic medications, including intravenous ketamine (300 mg/day), haloperidol (5 mg/day), antidepressants, and diclofenac were administered simultaneously. However, the pain intensity remained consistently above 5/10. Previously used opioids were retried before a trial of IPS was started but unfortunately did not improve her pain severity.
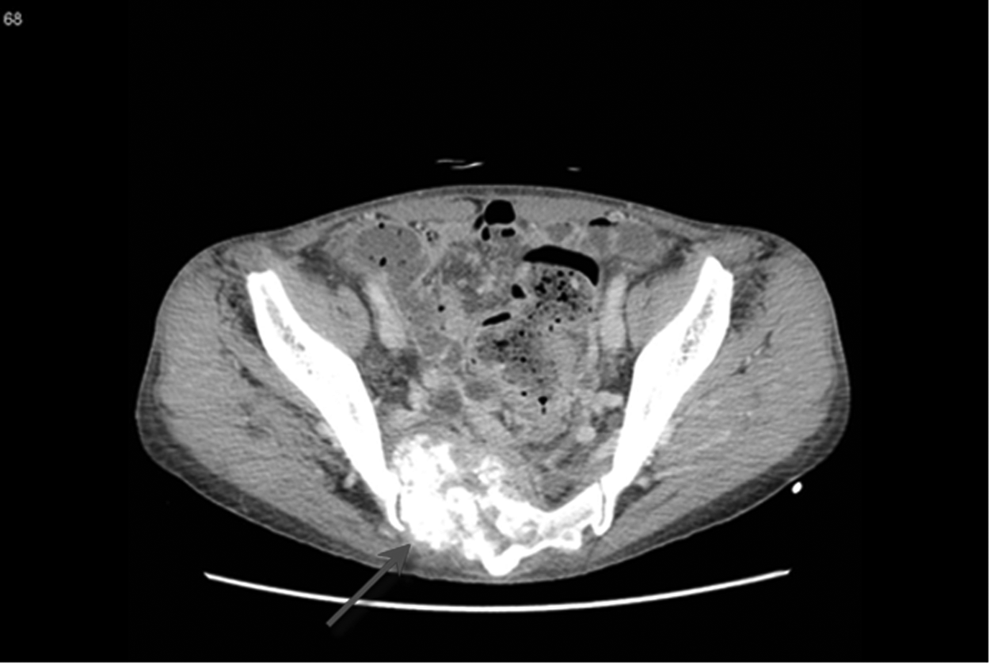
CT scan showing metastatic cancer with destruction of iliac bone.
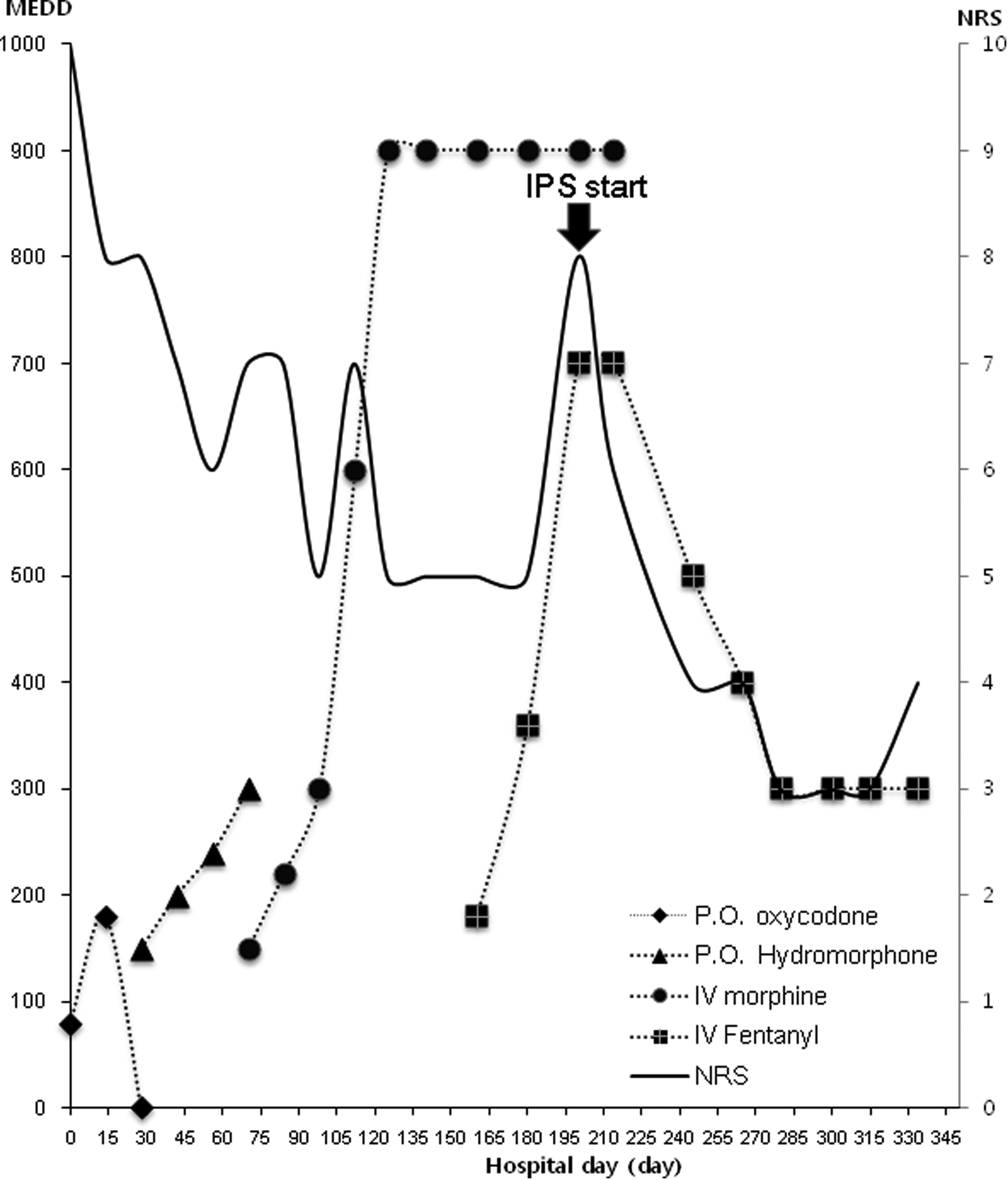
Graph of pharmacological and interventional treatments for cancer pain in case 1 (P.O., per Os; IV, Intravenous).IPS, intermittent palliative sedation; MEDD, morphine equivalent daily dose; NRS, numeric rating scale.
The patient also complained of insomnia due to severe bone pain. Zolpidem was administered orally, but had no effect. On admission and as-needed, a psychologist provided consultation to assess psychoexistential suffering. Antidepressants and anxiolytics were given for adjustment disorder and mood disorder, but had no effect on her pain experience. The treating team proposed to the patient and caregivers sedation limited to nighttime only. Intravenous midazolam was given every night (9 p.m. to around 6 a.m.) to induce unconsciousness. The dose was 2.5 mg for induction of sedation, and then 0.1 mg/kg/h as a continuous infusion. After sedation was held in the morning, the malignant bone pain was significantly reduced in severity, rated as 3/10 on the NRS during the daytime. Intermittent sedation was continued each night and the pain level remained constant. The patient died peacefully four months afterwards.
Case 2
A 65-year-old man was referred to our hospital for severe left upper abdominal pain. He had been diagnosed with metastatic pancreatic sarcomatoid carcinoma and had received gemcitabine- and fluoropyrimidine-based chemotherapy with no response. Intravenous oxycodone and fentanyl were given sequentially for pain control, and the MEDD was increased to 440 mg/day. Adjuvant medications, including gabapentin, ketamine, diclofenac, and dexamethasone, were given for pain control. Despite this treatment, the patient continued to have severe abdominal pain, graded as 8/10. A celiac plexus nerve block was attempted to control the pain, but it showed no response. Two days later the patient showed agitation and disorientation. The precipitating cause of delirium was scrutinized and was assumed to be multifactorial, including the rapid increase of opioids. His delirium did not respond to sequential medications including haloperidol, olanzapine, and venlafaxine. Pain also persisted above 5/10 as indicated on the FACES® Pain Rating Scale.
The patient's physician proposed IPS and offered palliative sedation every night (9 p.m. to about 4 a.m.) with a family member's consent. After IPS, cancer pain decreased to a mild intensity, graded 2/10 on the NRS, and the delirium improved at the same time. The patient died peacefully four weeks after intermittent sedation was started.
Discussion
PS is an intervention to control refractory symptoms during end-of-life care. The controversy concerning palliative sedation is surrounded by methodological rather than ethical issues. 10 Although PS is an ethically and legally proven intervention, many physicians are still reluctant to perform it because of fear that PS may hasten death. 11 However, several studies have not found a major association between PS and life shortening.12–14
As for type of PS, continuous sedation is more commonly used in practice. Although guidelines have suggested indications for PS, such as refractory symptoms including pain, delirium, and agitation,15–17 the type of sedation (i.e., continuous or intermittent) has not been specified. Literature regarding IPS is limited to several indications (see Table 1). The indications for IPS in those studies included incidental pain, dyspnea, agitation, and general malaise.4,9 No accurate data exist for the proportion of IPS cases encountered clinically. In one study, 23% of sedated patients were discharged alive, hinting that IPS was not an uncommon practice. 18
IPS, intermittent palliative sedation.
We have described two patients who sought alternative solutions from physicians concerning the dilemmatic situation of persistent intractable symptoms and fear of shortened survival. The patients spent the remainder of their lives alert during daytime with control of the severe symptoms by using intermittant palliative sedation. The indications for PS in our cases were simultaneous intractable pain and other symptoms such as insomnia and delirium. Those symptoms were controlled to tolerable stages by IPS during the final weeks of their lives.
Our cases revealed two important clinically significant findings. The first finding was the safety and conscious reversibility of IPS. The durations of IPS in our cases were four months and four weeks, respectively. During the hospitalization periods the patients were alert and communicating with family members during the day after stopping midazolam infusion. The consciousness reversibility of IPS indicating that patients were alert and communicating with family members during the daytime after stopping sedation. This may justify its use, along with decreased psychological burden among caregivers and clinicians. Therefore, patients in the dying stage who have refractory symptoms and want to preserve their awareness might be appropriate candidates for IPS.
The other finding was the efficacy of IPS. Both patients were relieved simultaneously of their pain and psychological distress by IPS. We assumed those effects of IPS stemmed from stopping the vicious cycle of physical and psychological distress. More research is needed to confirm our findings regarding safety and effectiveness in larger number of patients.
Our study has some limitations. The possibility of psychological or existential suffering contributing to pain expression could not be ruled out in our cases. However, both patients were assessed by an experienced psychologist, and antidepressants and anxiolytics were tried unsuccessfully to control pain. In addition, the pain characteristics supported somatic cancer pain, and the locations of pain were consistently specific, not diffuse, signifying an organic origin rather than a psychological problem.
The other drawback of the present study was the absence of pharmacodynamic or pharmacokinetic information. Considering the gradual deterioration of kidney and liver function during the terminal phase, patients may be exposed to the potential risk of permanent sedation after IPS. Dose modification should be determined depending on the individual response to midazolam.
In summary, we have described two patients who received IPS at night safely and while awake, and who were alert during the daytime for four weeks and four months until their death, respectively. Although IPS was not sufficient to completely end their distress, it offered relief of their unbearable symptoms to a tolerable intensity and contributed to their quality of life during the dying stage. Further prospective or larger retrospective cohort studies to address this issue are warranted.
Author Disclosure Statement
No competing financial interests exist.