
Abstract
Abstract
Background:
In Japan, palliative home care is subject to increasing demand from patients. However, the number of deaths at home is still not as high as that of palliative home care users.
Objective:
This study aimed to clarify factors influencing the place of death and home care rates, involving end-stage cancer patients targeted for palliative care by a general home-visit nursing agency.
Methods:
A total of 87 patients who had used palliative home nursing care services provided by the study facility within a 6-year period after its opening were studied.
Results:
The numbers of deaths at home supported by family physicians and those in hospital after readmission were 70 and 17, respectively. The numbers of deaths at home using services provided by the study facility and nurses belonging to it time-dependently increased, revealing a strong correlation between them. Furthermore, the place of death and home care rates were closely associated with the mean duration of home nursing services and home visits in collaboration with family physicians in charge.
Conclusion:
These results suggest that it may be possible to increase the rate of home care for end-stage cancer patients and meet their desires regarding the place of death through approaches to establish trust-based relationships with them and their families, such as strengthening manpower in home-visit nursing agencies and promoting collaboration between visiting nurses and family physicians in charge during home visits.
Introduction
I
Regarding medical systems to provide palliative home care services, designated cancer centers, palliative care wards, outpatient services and teams, home care support clinics, community-based pharmacies corresponding to palliative home care services, and home-visit nursing agencies, as well as information-sharing and collaboration among medical professionals in each community, have been promoted based on the Basic Plan to Promote Cancer Control Programs (established in 2007). 3 New instruments to share patient information (such as community liaison clinical pathways) have been developed and examined in empirical studies. 4 On the other hand, the number of clinics supporting palliative home care is reportedly increasing in general, but varies among communities. According to a survey conducted by the Ministry of Health, Labour, and Welfare, the number of each type of registered facility changed within the period between 2008 and 2014, as follows: home care support clinics: from 11,450 to13,7585; home-visit nursing agencies: from 5434 to 6590; and home care service providers: from 28,121 to 35,885.6,7 The number of home-visit nursing agencies in 2014, for example, markedly varied among prefectures, from 39 to 613. 8 In addition, the number of deaths at home during a 1-year period was 0 in half of the registered home care support clinics. 9
In addition, although the majority of home nursing service users are discharged from the hospital, based on their desire to receive end-of-life care at home, the number of deaths at home is not as high as this proportion. This situation is regarded as a challenge associated with undeveloped systems to provide care in places desired by patients3,4; for example, small-scale home-visit nursing agencies with fewer than five full-time nurses account for 66.3% of all facilities providing such care. 10 However, there is no evidence that an increasing number of visiting nurses reduces the number of deaths at home, leading to difficulty in making administrative judgments to ensure sufficient human resources.
In short, in Japan, delays in the development of systems to offer desired places of terminal care to patients have been noted. The proportion of deaths at home among cancer patients does not reach 10%.3,11 Home-visit nursing agencies are expected to play an important role in supporting palliative care and death at home in consideration of the intentions of cancer patients desiring home care, 12 and the promotion of multiprofessional liaisons, as well as manpower development on a community-wide basis, involving designated cancer hospitals, has been reported to be indispensable.13,14 In a previous study conducted in Japan, 15 it was suggested that family physicians sharing patient information with end-of-life home care and home-visit nursing agencies was an important factor in making home deaths feasible. In addition, a systematic review conducted by Gomes and Higginson 16 clarified patient-related determinants for the promotion of deaths at home, such as patients' and their families' desire to use home care services. However, factors related to home nursing service providers' background, as well as the influences of home nursing and multiprofessional liaisons on the place of death and home care rates for end-stage cancer patients, have not yet been fully clarified.
Therefore, this study targeted the Hibari Home Visit Nursing Agency based in Japan as a general home-visit nursing agency (study facility) to clarify home-visit nursing agency–related factors influencing the place of death and home care rates by examining the following items: 1) the correlation between the number of deaths at home and home-visit nursing agency–related factors, and 2) influences of home visits in collaboration with family physicians belonging to cooperative medical institutions and clinical nurse specialists (CNS) certified for palliative care or oncology nursing as part of multiprofessional liaisons on the place of death and home care rates for end-stage cancer patients.
Methods
Outline and background of the study facility
Data collected through clinical practice in the study facility as a model were retrospectively analyzed. Palliative home care services were provided through team approaches in collaboration among doctors, CNS, and professionals belonging to other medical institutions, and team members varied among the patients.
The study facility opened in November 2007, with a number of staff members equivalent to 2.5 full-time workers, to provide care services corresponding to the categories of additional medical fees for the provision of care on a 24-hour basis and special management services. The number of full-time staff members was 6.5 (6 full- and 1 part-time) in 2012.
Subjects
Among end-stage cancer patients who had used palliative care services provided by the study facility within a 6-year period between November 2007 and October 2013, all those whose death (at home or in hospital after readmission) was confirmed by October 2013 were studied, dividing them into two groups based on the place of death: at home and in hospital. Patients who were alive as of October 2013 and those without experience of home visits (interviews only) were excluded.
Study items
From the target patients' home nursing records stored in the study facility, data regarding background factors (Table 1), the duration of home nursing services, collaborative home-visit members, and information-sharing tool use were extracted. The terms used in this paper and calculated items are defined as follows:
PS, Performance Status; SD, standard deviation.
End-stage cancer patients
This described those patients with the words <cancer>, <end-stage>, or <last-stage condition> in their home nursing order sheets.
Long-term care grade
A this a 7-grade index indicating an increasing higher degree of care needed for a patient, and is determined initially through a computerized system and subsequently by the Certification Committee of Needed Long-Term Care (consisting of those with an academic background in the field of health science, medicine, or welfare) organized in each municipality. It is used to set the upper limit of payment in the long-term care insurance system.
Home care rate
The is the proportion of home care a target patient underwent before death (duration of home care [days]/duration of survival after intervention [days]×100)
Number of full-time nurses belonging to the study facility
This is a value obtained by dividing the total number of work hours (total number of hours engaged in services) by the fixed number of work hours for general full-time workers (40 hours a week in the case of the study facility) to convert the number of part-time workers into that of general full-time workers.
Mean duration of home nursing services (minutes)
This is the mean duration of home nursing services (minutes) provided by visiting nurses per visit.
Home visits in collaboration with family physicians
This describes home visits made by visiting nurses in collaboration with family physicians after obtaining patients' and their families' consent.
Home visits in collaboration with CNS
These are home visits made by visiting nurses in collaboration with hospital CNS after obtaining patients' and their families' consent.
Information-sharing tools
These are tools distributed to patients on discharge from the hospital to home, with a view to sharing information regarding their conditions and doctors' instructions among home care service providers, medical professionals, patients, and their families 4 ; such tools are not applicable in some cases, depending on the cooperative medical institutions' judgments.
Analysis
Background of the study facility and time-dependent changes in the number of deaths at home
The 6-year study period was divided into the first (from November 2007 to October 2010) and second (from November 2010 to October 2013) halves to compare the numbers of deaths in the hospital, those at home, and full-time nurses belonging to the study facility between them. The correlation between items showing marked differences was also examined by calculating Pearson's correlation coefficient.
Influences of home nursing and multiprofessional liaisons on the place of death
Multiple logistic regression analysis was performed, with the place of death as an objective variable. Furthermore, with the mean duration of home nursing services, home visits in collaboration with family physicians, those in collaboration with CNS, and the use of information-sharing tools as explanatory variables, data were adjusted for the target patients' ages and Performance Status (PS) scores when requests for home nursing were made.
Influences of home nursing and multiprofessional liaisons on home care rates
Multiple regression analysis was also performed, with the rates of home care the target patients underwent after discharge before death as an objective variable. The adjustment procedure was implemented, similarly to that in influences of home nursing and multiprofessional liaison on the place of death, with the same factors as explanatory variables.
Ethical considerations
Analytical data were processed through nonlinkable anonymization to prevent identification, and appropriately managed under the supervision of a personal information manager. This study was conducted with the approval of the Ethics Committee of Care Circle Hibari.
Results
Among the 96 end-stage cancer patients who desired palliative home care, 87 meeting the inclusion criteria were targeted. The number of deaths at home was 70 (Fig. 1).
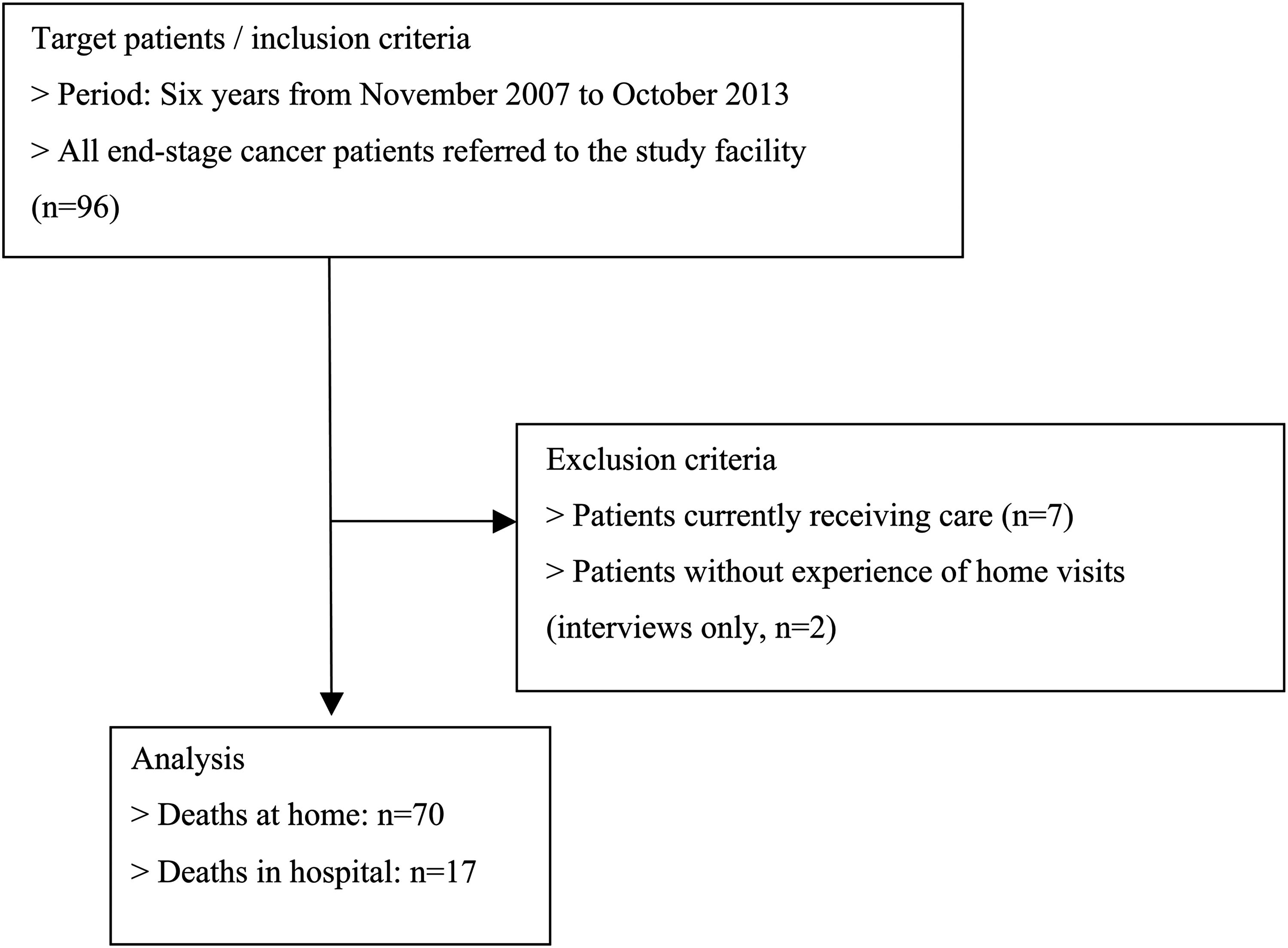
Flowchart of the selection of patients.
Time-dependent changes in the number of deaths at home
The number of deaths at home was markedly higher during the second (17.0±1.0) than during the first (6.3±1.2) half of the study period (p<0.001). The number of full-time nurses belonging to the study facility was also markedly higher during the second (5.9±1.0) than during the first (3.0±0.6) half of the study period (p=0.014). Similarly, both the number of deaths at home and that of full-time nurses belonging to the study facility time-dependently increased, showing a strong correlation with each other (r=0.90, p=0.016).
Influences of home nursing and multiprofessional liaisons on the place of death
Tables 1 and 2 show the extracted background factors influencing the place of death and the results of multivariate analysis, respectively. Among the study items, two factors—the mean duration of home nursing services and home visits in collaboration with family physicians—showed significant differences on both univariate and multivariate analyses.
In short, a longer mean duration of home nursing services per visit frequently led to death at home, and death at home was more common among patients who experienced home visits in collaboration between visiting nurses and doctors in charge once or more.
CNS, clinical nurse specialists; SD, standard deviation.
Influences of home nursing and multiprofessional liaisons on home care rates
To clarify factors influencing home care rates, multivariate analysis was performed, and the results shown in Table 3 were obtained. Home care rates markedly varied in relation to the mean duration of home nursing services and home visits in collaboration with family physicians.
Adjusted coefficient of determination (R2): 0.218.
In short, a longer mean duration of home nursing services and the experience of home visits in collaboration between visiting nurses and doctors in charge frequently led to a higher home care rate.
CNS, clinical nursing specialists.
Discussion
To the authors' knowledge, this study is the first to examine factors influencing time-dependent changes in the number of end-stage cancer patients' deaths at home and those associated with the place of death and home care rates, involving a single home-visit nursing agency. The most important result obtained from it was that the experience of home visits in collaboration with family physicians and mean duration of home nursing services influenced both the place of death and home care rates for end-stage cancer patients undergoing home nursing. Collaboration with family physicians during home visits deepens visiting nurses' insight into patients, and helps them to establish “face to face relationships.” 17 To promote palliative home care, it is important to enable patients to choose home care services based on their own desires and sense of security, rather than simply focusing on deaths at home. 3 In line with this, the identification of factors influencing the place of death and home care rates is likely to be very useful for visiting nurses supporting patients desiring to spend their last days of life at home and their families, as it may provide an important basis for their home nursing activities.
Regarding the mean duration of home nursing services as a factor influencing the place of death, Fukui and colleagues reported that such an influence arises when the weekly number of home visits made to a patient immediately after discharge was 3.7 or higher. 18 Similarly, Wakabayashi and Yuzawa compared deaths at home between cancer and noncancer patients, and confirmed that the duration of home nursing services needed by the former is longer. 19 These findings, similarly to those from the present study, suggest that, in end-of-life support for end-stage cancer patients, the appropriate duration of home nursing services may be longer.
The second most important result of the present study was that the numbers of deaths at home and full-time nurses belonging to the study facility time-dependently increased, showing a significant and strong correlation between them. Although the causal relationship between them remained unclear, it may be possible to increase the number of deaths at home by increasing the number of full-time nurses belonging to home-visit nursing agencies and the duration (quality) of home nursing services in consideration of the influence of the mean duration of home nursing services on the place of death and home care rates.
When revising the medical insurance system in 2014, 20 the Ministry of Health, Labour, and Welfare adopted a new system to benefit home-visit nursing agencies actively providing end-of-life care and dealing with patients in serious conditions with a particular incentive, with a view to promoting home medical services. In line with this, it became obligatory to ensure the availability of five or more full-time workers within the facility; in the study facility, the number of such workers exceeded five during the second half of the study period, which may have contributed to the increased number of deaths at home and the home care rate. Therefore, the availability of a sufficient number of full-time staff members may be an important index for home-visit nursing agencies aiming to meet patients' desire to spend their last days of life at home.
Regarding study limitations, although a strong correlation between the numbers of full-time nurses belonging to the study facility and deaths at home was revealed, the retrospective analysis did not clarify the mean number of full-time nurses belonging to the study facility on intervention. To examine the causal relationship between the number of full-time nurses belonging to the study facility or mean duration of home nursing services and the number of deaths at home, prospective intervention studies may be needed. In this preliminary study, data were collected from a single facility, targeting a limited number of subjects. Furthermore, factors possibly influencing the place of death (such as the management of symptoms during home care, caregivers' skills, living with relatives, and availability of extended family support 16 ) were not measured; therefore, it was difficult to rule out their influences even through multivariate analysis, and this should also be noted as a limitation.
Despite such limitations, the study is still likely to provide an important future perspective on these issues (the influences of home nursing service use and collaboration among multiple professionals on the place of death, as well as those related to home-visit nursing agencies), which have been rarely examined in previous studies. On the basis of the obtained results, it may be possible to increase the rate of home care for end-stage cancer patients and meet their desires regarding the place of death through approaches to establish “face-to-face relationships” as a relatively feasible and effective measure to deal with the increasing number of deaths at home.
Footnotes
Acknowledgments
The authors would like to thank Makoto Hirano (Director of Hirano Clinic), Hiroshi Nozawa (Director of Nozawa Clinic), Hitomi Harada (Chief Director of Care Circle Hibari, an NPO), JunkoMiyai (Manager of Kokage Home Nursing Agency), and staff members of Hibari Home Nursing Agency, as well as those of medical institutions who cooperated with this study.
This study was supported by Grants-in-Aid for Scientific Research from the Japan Society for the Promotion of Science (JSPS,25460892) and an administrative grant from the University of Toyama.
Author Disclosure Statement
No competing financial interests exist.
This study was supported by a grant 25460892 from the Japan Society for the Promotion of Science.