
Abstract
Abstract
Background:
Malignant psoas syndrome (MPS) is a relatively rare syndrome that accompanies malignancy; the pain associated with MPS is often difficult to control. Methadone is known to be effective in relieving both nociceptive and neuropathic pain.
Objective:
Herein we describe treatment strategies for three patients with MPS, diagnosed by imaging and clinical findings, who responded to methadone treatment.
Methods:
Patient diagnoses, pain characteristics, and treatment were analyzed retrospectively.
Subjects were three patients with MPS who presented to Hyogo Cancer Center with pain. A numeric rating scale (NRS; 0–10) was used to assess patients' pain levels.
Results:
All three patients were diagnosed with malignancies (prostate, cervical, and urachal) and had impaired gait and thigh extension. All had tumor invasion to the iliopsoas muscle, as determined by imaging, and were diagnosed with MPS. After starting methadone, symptoms improved in all patients and they were able to extend the thigh and walk normally. The NRS scores improved by an average of −7.3 points (95% confidence interval [CI] −4.97, −9.69) on Day 14; and the average time until symptom improvement after starting methadone was 2.3 days (95% CI 1.86, 2.80).
Conclusions:
Methadone may be considered a treatment choice for MPS patients in whom pain is difficult to control.
Introduction
M
Although it has been used worldwide for more than 60 years, methadone was first approved for use in Japan in 2013. Methadone has no active metabolite and may be administered to patients with declining renal function. In addition, it has low cross-resistance with other opioids and exhibits N-methyl-
However, the half-life of methadone can range from 12 to 150 hours. It takes approximately one week for stable blood concentrations to be reached, and there is a risk of drug accumulation in the body because methadone is fat soluble. 3 One of the issues considered during the approval process of methadone in Japan was the high mortality rate associated with its use compared with other opioids. 4 Following the approval of methadone in Japan, the Ministry of Health, Labour and Welfare recommends that the use of methadone be rotated with 60 mg/day morphine, or an equivalent dose of other opioids, when pain is not well controlled.
Methadone has been used primarily to treat drug addiction, 5 and although the use of methadone in cancer is increasing, there are few reports describing its use for the treatment of cancer pain. 6 We have experienced three patients who were diagnosed with MPS in whom methadone treatment was effective. Herein we describe these cases and their respective treatment strategies.
Methods
The present study was a retrospective analysis of three MPS patients who responded to methadone. The switch from morphine to methadone was made by stopping morphine with an immediate substitution of methadone using a stop-and-go (SAG) approach; in the case of transdermal fentanyl, the drug was discontinued six hours before patients were started on oral methadone.7,8
A numeric rating scale (NRS; 0–10) was used to assess patients' pain levels, as per the MD Anderson Symptom Inventory. The highest and lowest possible scores are referred to as the NRSmax and NRSmin, respectively. Toxicity was evaluated on the basis of Common Terminology Criteria for Adverse Events version 4.0. In this article we define the day we started oral methadone as Day 1.
Results
Three patients with MPS presented to Hyogo Cancer Center between April 2013 and July 2014. Pain was not well controlled in any of the patients with opioids (morphine, oxycodone, and fentanyl); and there was evidence of opioid toxicity; thus, all three patients were switched to oral methadone. The status of each patient at the time of presentation is given in Table 1, and each case is reviewed in detail below.
BSC, ; IPS, ; MPS, ; Obs,.
Case I
A 59-year-old man presented because of intractable pain in May 2013. He had been diagnosed previously with prostate cancer and had been undergoing hormone therapy and chemotherapy since September 2010. No other clinical history was noted.
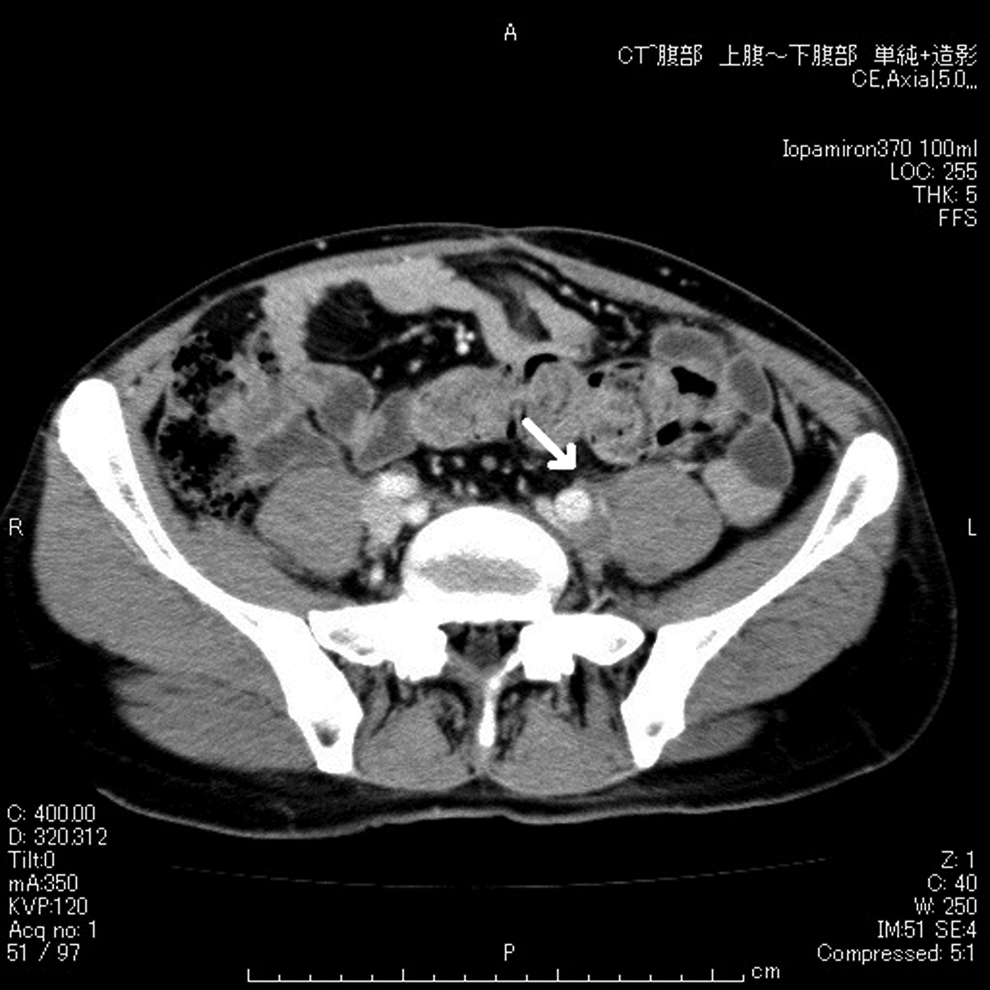
The patient had pain in his back and left lower abdomen and had difficulty walking and extending his thigh because of the pain. The psoas muscle stretch test was positive. On positron emission tomography (PET)/ computed tomography (CT), high uptake (maximum standardized uptake value 8.39) was observed at the right common iliac lymph nodes, indicating metastases. These metastases directly infiltrated the iliopsoas muscle. In addition, external iliac lymph node metastases and spinal metastasis to L2 were observed (see Figure 1).

Positron emission tomography/computed tomography of Case 1 on admission.
Upon presentation, the patient was administered transdermal fentanyl (nearly equivalent to 1.75 mg fentanyl by continuous intravenous infusion [c.i.v.]), morphine hydrochloride hydrate as a rescue dose, and 1 mg dexamethasone, but his pain was not controlled and he did not respond to the rescue dose of morphine other than becoming extremely sleepy. Despite the addition of 400 mg etodolac, the patient's pain did not improve.
Six hours after discontinuing transdermal fentanyl, the patient was started on oral methadone (30 mg/day). On Day 3 his pain had resolved such that he was able to extend his thigh and walk. On Day 5, Grade 2 nausea developed. On Day 7 the methadone dose was reduced to 20 mg/day. On Day 13 the patient was admitted to hospital because of cellulitis of the right lower limb, but he soon recovered with intravenous antibiotics. On Day 14 the patient's NRSmax was reduced from 10 (on Day 1) to 2, and the NRSmin was reduced from 2 (on Day 1) to 0. Although the patient died approximately six months after starting methadone treatment, his pain was well controlled up until one week before he died, at which time he was no longer able to take oral medication. The changes in NRS scores and doses are shown in Figure 2.
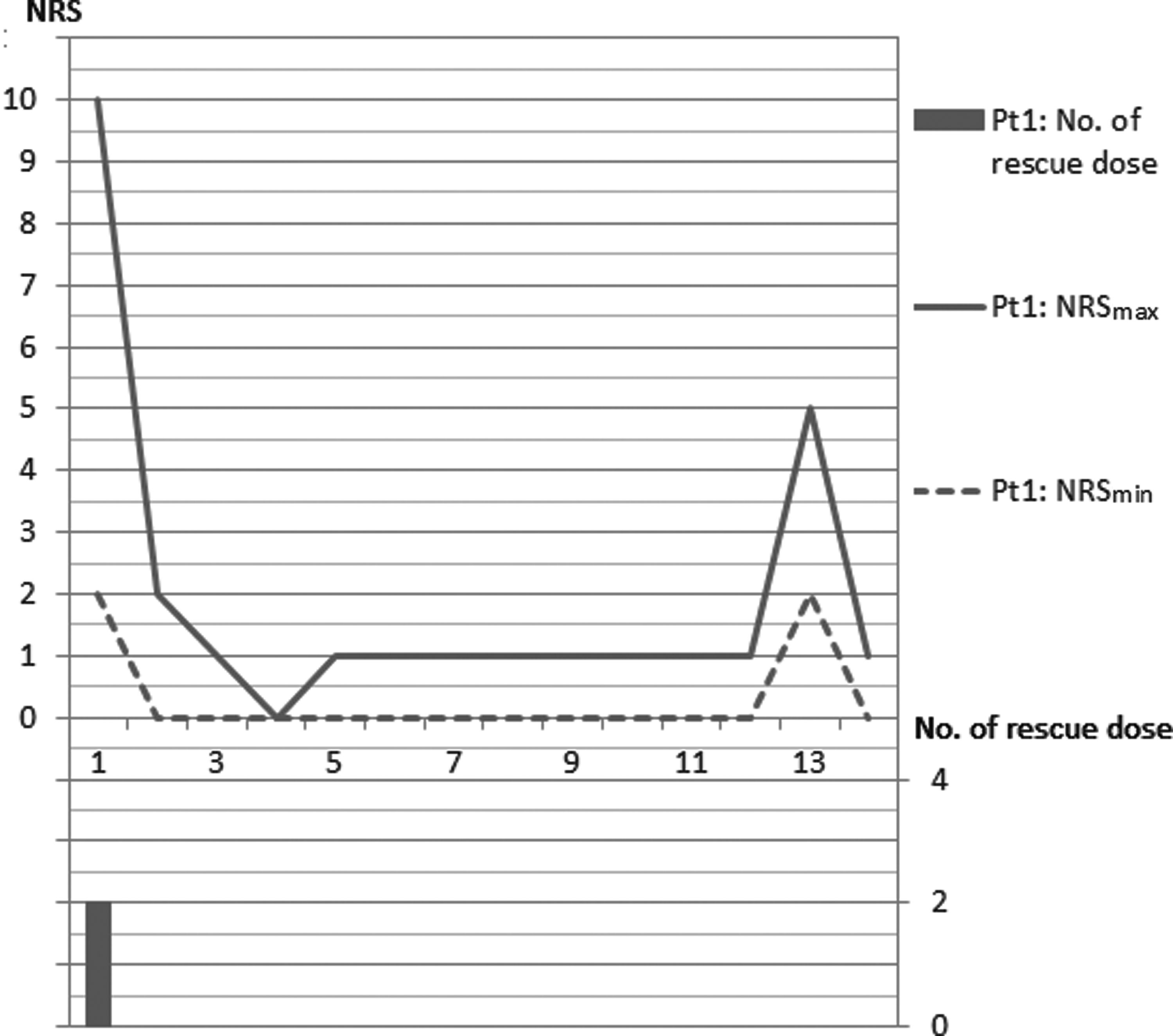
The change of NRS and the number of rescue doses in Case 1.
Case II
A 35-year-old man was referred to Hyogo Cancer Center in February 2014 because of pain in his left leg. He had been diagnosed previously with urachal cancer and treated surgically (in 2008, 2009, and 2012) and with adjuvant chemotherapy with cisplatin and S-1 in 2010. No other clinical history was noted.
The patient had left inguinal and thigh pain with leg edema. He also had strong pain when we straightened his left knee, such that he was unable to lie on a bed. The psoas muscle stretch test was positive. CT revealed swelling of the left common iliac lymph node to 11 mm and infiltration into the left iliopsoas muscle; the left inguinal lymph nodes were also swollen, but there was no apparent obstruction of the circulation (see Figure 3).
Computed tomography of Case 2 on admission.
The patient had been given 200 mg tramadol hydrochloride for pain control, but this did not work, so he was switched to oxycodone SR (60 mg/day). In addition, the patient was on 75 mg/day pregabalin and 180 mg/day loxoprofen sodium hydrate. Despite this, the patient's pain remained uncontrolled and the rescue medication (10 mg oxycodone) was ineffective, inducing only strong sleepiness.
After admission, the patient was started on oral methadone (15 mg/day) with a rescue dose of 10 mg oxycodone. On Day 2 his symptoms had improved and he could lie on a bed and walk with less pain. On Day 5 the patient could assume the position for palliative irradiation, so he was treated with palliative irradiation to the pelvis with a total dose of 37.5 Gy (15 fractions [Fr]). On Day 14, despite the fact that the palliative irradiation had not been completed, the patient's NRSmax was reduced from 10 (on Day 1) to 1, and the NRSmin was reduced from 7 (on Day 1) to 1. At the time of writing, the patient is still alive and undergoing chemotherapy; his pain continues to be well controlled with methadone. The change in NRS scores and doses are shown in Figure 4.
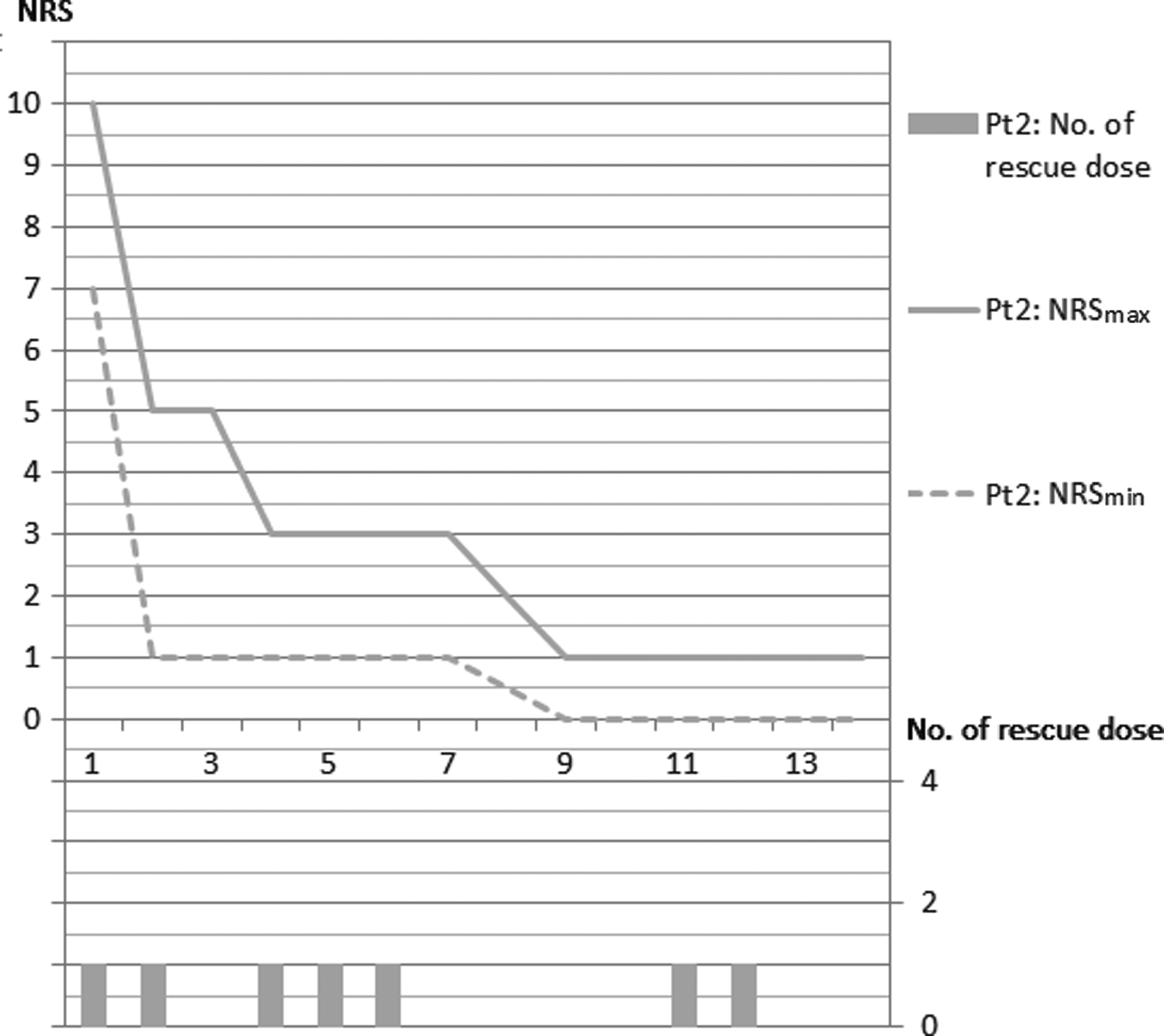
The change of NRS and the number of rescue doses in Case 2.
Case III
A 70-year-old woman was referred to Hyogo Cancer Center in April 2014 because of pain when moving. She had been diagnosed with cervical cancer in 2013 and had been treated with chemoradiation, including radiation to the pelvis (65 Gy/35 Fr) and uterovaginal brachytherapy (14.83 Gy/3 Fr), and chemotherapy with cisplatin. The patient had also been diagnosed previously with oropharyngeal carcinoma and treated with induction chemotherapy followed by chemoradiation, but it is unlikely that this tumor was associated with her current pain. A clinical history of an appendectomy at 18 years of age was noted.
The patient had pain in the left lower abdomen, along with left inguinal and thigh pain; she also had difficulty moving, especially walking. The psoas muscle stretch test was positive. Direct invasion to the left iliopsoas muscle was observed on PET/CT, as were lung metastases, invasion into the right muscle under the shoulder blade, and a residual lesion at the cervix and urethra (see Figure 5).
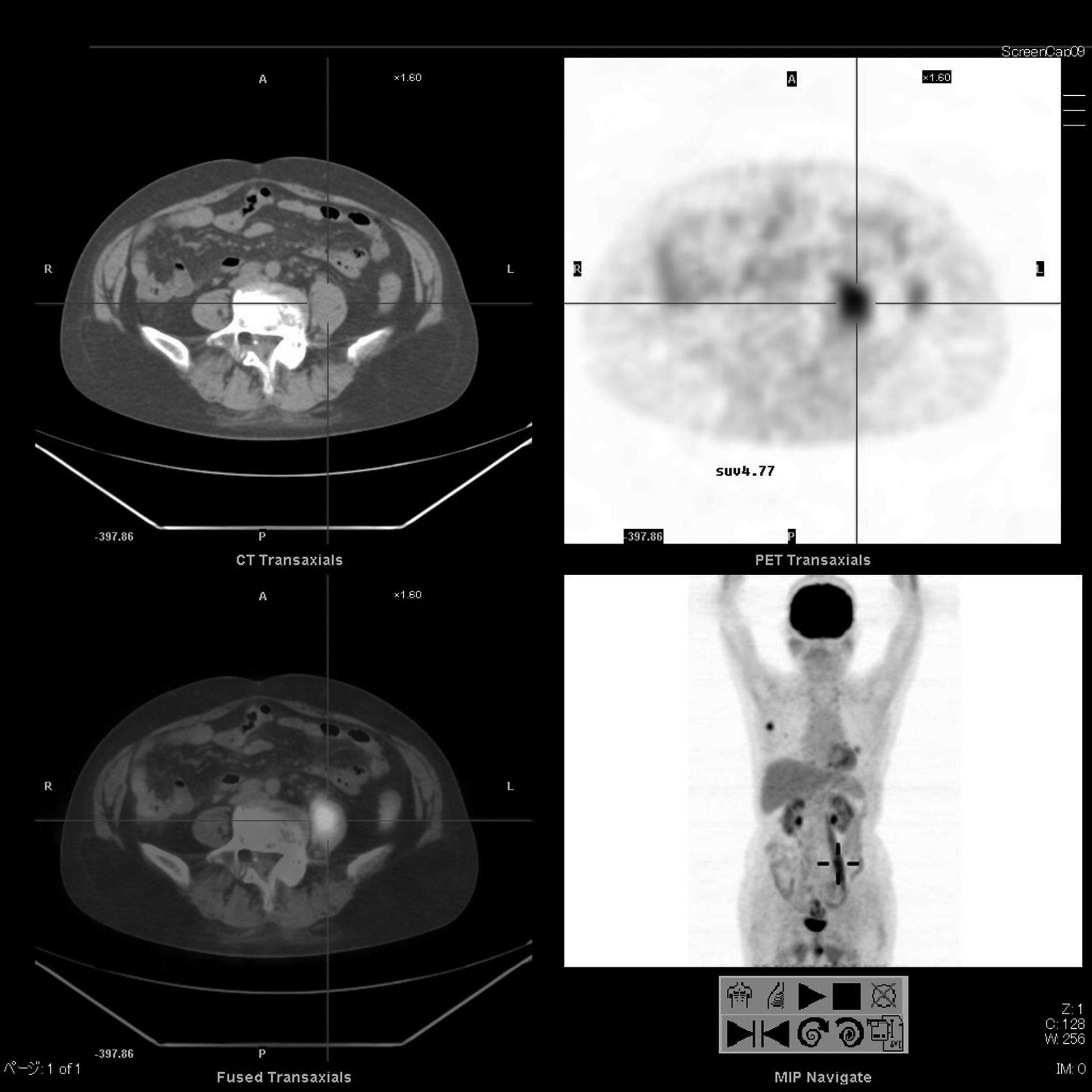
Positron emission tomography/computed tomography of Case 3 on admission.
Despite being treated with 10 mg/day oxycodone SR and 180 mg/day loxoprofen, the patient was admitted to Hyogo Cancer Center because of her pain. Loxoprofen was stopped at the time of hospitalization because of reduced renal function, and titration with oxycodone c.i.v. was started. However, the patient felt strong, unpleasant sleepiness with 14.4 mg/day oxycodone c.i.v. The dose of oxycodone was reduced to 12 mg/day c.i.v., but the patient's pain was not controlled with this dose. The patient was switched to 1.2 mg fentanyl c.i.v. in an attempt to decrease her sleepiness, but she remained sleepy and her pain remained uncontrolled.
The patient was then started on oral methadone (15 mg/day), and at the end of Day 1 of treatment she was able to extend her left thigh; on Day 2 her movement-related pain had improved. On Day 7, despite good pain control, the dose of oral methadone was reduced from 15 mg/day to 10 mg/day because delirium was observed. On Day 8 the patient was able to start rehabilitation, but her NRS score worsened. The pain symptoms differed from the MPS pain and were thought to be due to vesical tenesmus caused by bladder invasion. The patient was started on loxoprofen again because her renal function had recovered by that time. On Day 11 the patient's pain levels were again reduced. On Day 14 the patient's NRSmax was reduced from 8 (Day 1) to 4, but her NRSmin was relatively stable at 1 (0 on Day 1). The patient died approximately two months after starting methadone, but her pain was well controlled up until three days before her death, at which time she was no longer able to take oral medication. The changes in NRS scores and doses are shown in Figure 6.
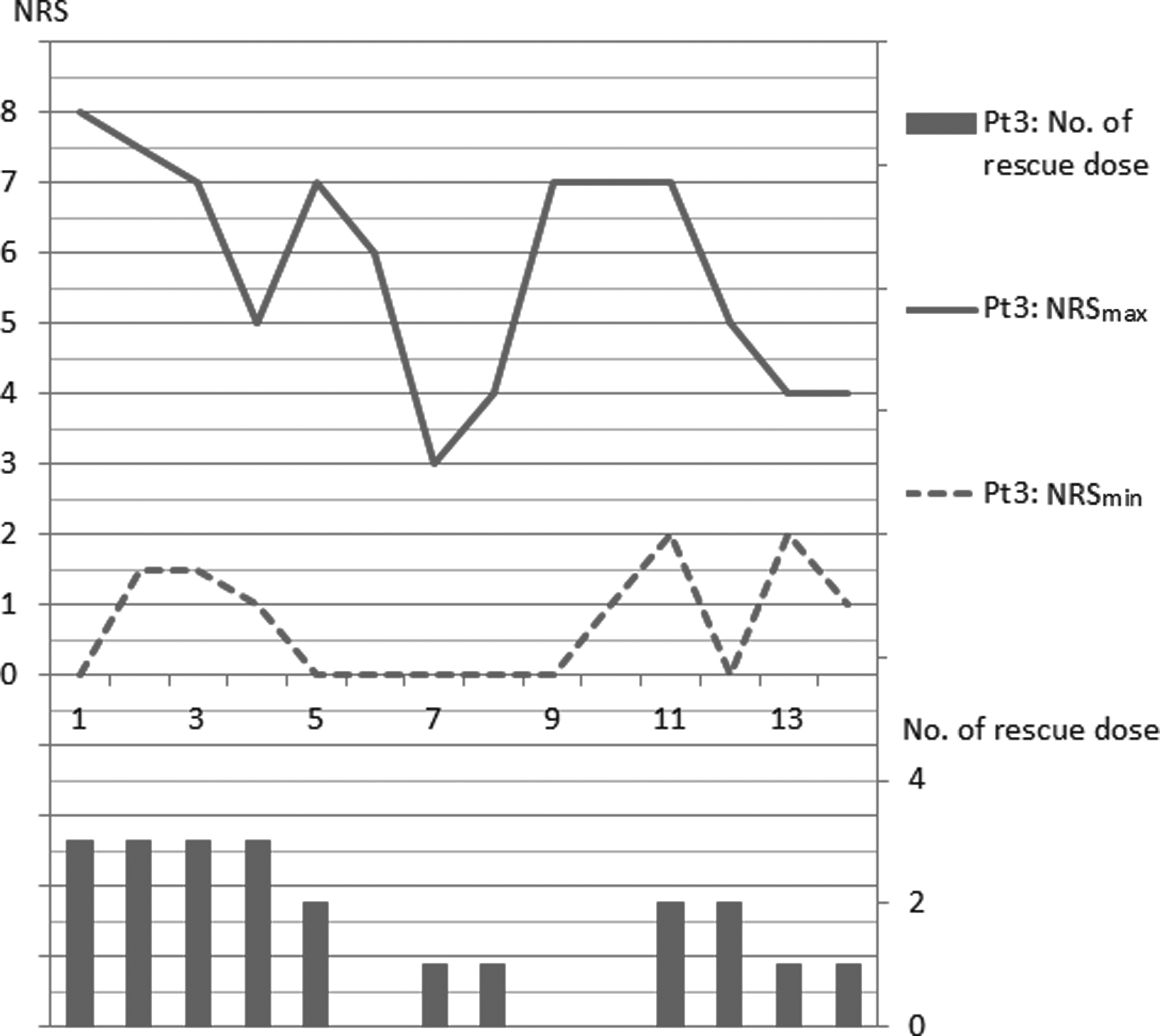
The change of NRS and the number of rescue doses in Case 3.
Efficacy
After methadone initiation, the patients' pain symptoms had improved within three days (average 2.3 days; 95% confidence interval [CI] 1.86, 2.80), and they could all extend their thigh and walk. The NRSmax was reduced by an average of −7.3 points (95% CI −4.97, −9.69) by Day 14. Pain was well controlled in two of the three patients up until they were no longer able to take oral medication.
Discussion
With methadone treatment, all three MPS patients experienced an improvement in their symptoms and could extend their thigh and walk. The NRS scores also clearly improved in a relatively short period of time, and the number of rescue doses used decreased in two of the three patients. In the third patient, the NRS score and the number of rescue doses decreased once, but when she started rehabilitation, her pain worsened transiently due to vesical tenesmus. This pain was resistant to the rescue medication and the patient did not want to use rescue doses. Furthermore, the development of delirium between Days 7 and 10 was another reason for the temporary reduction in rescue doses. This patient's symptoms improved soon after she was restarted on loxoprofen, but some residual pain remained while moving. From the aspect of morphine equivalent daily dose (MEDD), the MEDD of all three patients was decreased by switching to oral methadone (Case I, 175.0 mg to 47.0 mg MEDD/day; Case II, 90.0 mg to 70.5 mg MEDD/day; Case III, 120.0 mg to 47.0 mg MEDD/day). 9
Although there are no standard criteria for the switch from other opioids to methadone, all three patients in the present series had tried up to two different opioids before switching to methadone—Case I: morphine rescue and fentanyl; Case II: tramadol and oxycodone; Case III: oxycodone and fentanyl—which had resulted in a poor response and unacceptable toxicity. For these reasons we decided to use methadone. The switch to methadone was made using the SAG approach.7,8 While switching from the other opioids to methadone, rescue doses were used for breakthrough pain. The rescue doses were effective for Case II, and we continued. For Case I, the rescue medication was changed to a diclofenac suppository, which was used only a few times. Case III continued with fentanyl i.v. at first, but her pain control was not good. After the addition of sublingual fentanyl, this patient's pain improved.
If rescue doses prove to be useful even slightly, we continue them at first. If there is no response at all to rescue doses, changing to another rescue medication is preferable. Furthermore, the addition of rapid-onset opioids may be beneficial. A recent study has reported that switching over three days is preferable to the SAG strategy when changing from high-dose morphine to methadone. 10 However, more information from a greater number of case studies is necessary before definitive recommendations can be made about how best to switch from opioids to methadone.
According to several previous reports, pain associated with MPS is often difficult to control. Of course, the best treatment to control pain is to control the tumor itself.2,11 However, in most cases the tumor is metastatic and inoperable. Chemotherapy or palliative radiation may then be administered. This requires more time to control the tumor, and sometimes the continuation of treatment is difficult because of tumor pain. Other palliative treatment is essential for continuing tumor control.
One reason why MPS pain is difficult to control is that the pain is not purely nociceptive, because neuropathic pain may also be involved.1,11 Neuropathic pain is often difficult to control, and there are currently few drugs effective against this type of pain. In addition, MPS is often resistant to nerve blocks, extradural blocks, and subarachnoid blocks.2,11
Methadone is a newly introduced opioid in Japan. The most important characteristic of this drug is that it acts not only on μ-opioid receptors, but also on NMDA receptors.12–14 In Japan, methadone is to be used only if other opioids are not effective; therefore, prior opioid use is noted in most patients. In a previous study, approximately 80% of patients whose pain was not well controlled with other opioids responded to oral methadone. 8 Intractable pain is one of the most common problems that results in deterioration of cancer patients' quality of life. 15 In previous studies, less than 50% of MPS patients were able to control their pain with multimodal treatments, including NSAIDs, opioids, adjuvant drugs, and epidural or intrathecal anesthesia.1,2,11 It is currently unclear why the pain in these MPS patients responds to methadone, but it seems that methadone may be one of the treatment choices for MPS refractory to other opioid therapy and with difficult-to-control pain.
Furthermore, the recognition of MPS is low, and so MPS may be underdiagnosed. 11 Both clinical symptoms and imaging scans are important in the diagnosis of MPS. If patients have difficulty extending their thigh and walking, imaging or reevaluation of imaging may be considered to assess involvement of the iliopsoas muscle. Although not unique to MPS, it is necessary to accurately assess the origin of pain to appropriately control cancer-related pain.
There are certain limitations to the present study. In particular, the study was a retrospective study with very few cases. All patients had severe pain, and two patients did not have enough time to try other adjuvant drugs except for NSAIDs. However, no previous study has described highly effective treatment choices for MPS. The findings of the present study indicate that there is the possibility that MPS will respond to methadone, but further studies are required to prove the benefits of methadone in these patients.
In conclusion, further studies are needed to validate the efficacy of methadone treatment for MPS. In addition, it will be beneficial to identify predictive markers or symptoms of responsiveness to methadone.
Footnotes
Author Disclosure Statement
No competing financial interests exist.